Advising Customers About Scars and Stretch Marks
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

The Nutritional Relationships of Zinc David L
The Nutritional Relationships of Zinc David L. Watts, D.C., Ph.D., F.A.C.E.P.i Zinc was discovered to be essential for the also indicate tissue redistribution.12 The normal growth of living organisms in 1869. The range of zinc in the hair has been reported suspicion that zinc deficiency occurs in man is between 15 and 22 milligrams percent,4 the ideal relatively recent. In 1963, studies reported by being 20 milligrams Prasad and co-workers on Iranian men suffering percent. from dwarfism and hypogonadism found that nutritional zinc deficiency was a causative factor Manifestations of Zinc Deficiency Absolute or in these disorders.1 2 3 Since that time zinc has Relative gained a greater recognition for its role in human Manifestations of zinc deficiency will vary health and has stimulated extensive research. It is from one individual to another. This is true of now known that zinc is essential to over 100 almost any nutrient, and can be explained by enzymes in the body. Perhaps one of the most recognizing that two types of a deficiency state important discoveries is zinc's involvement in the can occur, either a relative deficiency, or synthesis of RNA. absolute deficiency. An absolute deficiency develops as a result of inhibited absorption Distribution accompanied by a concurrent increase in zinc The highest concentration of zinc is found in excretion or utilization. TMA patterns usually the choroid of the eye and optic nerve, followed reveal a low tissue zinc (less than 12 mg.%). An by the prostate, bone, liver and kidneys, muscles absolute deficiency of zinc can be contributed to (zinc content varies with colour and function of by hypoadrenocorticism, hyperthyroidism and muscles), heart, spleen, testes, brain, and other endocrine factors. -

The Skin in the Ehlers-Danlos Syndromes
EDS Global Learning Conference July 30-August 1, 2019 (Nashville) The Skin in the Ehlers-Danlos Syndromes Dr Nigel Burrows Consultant Dermatologist MD FRCP Department of Dermatology Addenbrooke’s Hospital Cambridge University NHS Foundation Trust Cambridge, UK No conflict of interests or disclosures Burrows, N: The Skin in EDS 1 EDS Global Learning Conference July 30-August 1, 2019 (Nashville) • Overview of skin and anatomy • Skin features in commoner EDS • Skin features in rarer EDS subtypes • Skin management The skin • Is useful organ to sustain life ØProtection - microorganisms, ultraviolet light, mechanical damage ØSensation ØAllows movement ØEndocrine - vitamin D production ØExcretion - sweat ØTemperature regulation Burrows, N: The Skin in EDS 2 EDS Global Learning Conference July 30-August 1, 2019 (Nashville) The skin • Is useful organ to sustain life • Provides a visual clue to diagnoses • Important for cultures and traditions • Ready material for research Skin Fun Facts • Largest organ in the body • In an average adult the skin weighs approx 5kg (11lbs) and covers 2m2 (21 sq ft) • 11 miles of blood vessels • The average person has about 300 million skin cells • More than half of the dust in your home is actually dead skin • Your skin is home to more than 1,000 species of bacteria Burrows, N: The Skin in EDS 3 EDS Global Learning Conference July 30-August 1, 2019 (Nashville) The skin has 3 main layers Within the Dermis Extracellular Matrix 1. Collagen 2. Elastic fibres 3. Ground Substances i) glycosaminoglycans, ii) proteoglycans, -

Rapid Development of Perifolliculitis Following Mesotherapy
CASE LETTER Rapid Development of Perifolliculitis Following Mesotherapy Weihuang Vivian Ning, MD; Sameer Bashey, MD; Gene H. Kim, MD patient received mesotherapy with an unknown substance PRACTICE POINTS for cosmetic rejuvenation; the rash was localized only to the injection sites.copy She did not note any fever, chills, • Mesotherapy—the delivery of vitamins, chemicals, and plant extracts directly into the dermis via nausea, vomiting, diarrhea, headache, arthralgia, or upper injections—is a common procedure performed respiratory tract symptoms. She further denied starting in both medical and nonmedical settings for any new medications, herbal products, or topical therapies cosmetic rejuvenation. apart from the procedure she had received 2 weeks prior. • Complications can occur from mesotherapy treatment. Thenot patient was found to be in no acute distress and • Patients should be advised to seek medical care with vital signs were stable. Laboratory testing was remarkable US Food and Drug Administration–approved cosmetic for elevations in alanine aminotransferase (62 U/L [refer- techniques and substances only. ence range, 10–40 U/L]) and aspartate aminotransferase (72 U/L [reference range 10–30 U/L]). Moreover, she had Doan absolute neutrophil count of 0.5×103 cells/µL (refer- ence range 1.8–8.0×103 cells/µL). An electrolyte panel, To the Editor: creatinine level, and urinalysis were normal. Physical Mesotherapy, also known as intradermotherapy, is a examination revealed numerous 4- to 5-mm erythematous cosmetic procedure in which multiple -

Immunocompromised Districts of Skin: a Case Series and a Literature Review
ID Design Press, Skopje, Republic of Macedonia Open Access Macedonian Journal of Medical Sciences. 2019 Sep 30; 7(18):2969-2975. https://doi.org/10.3889/oamjms.2019.680 eISSN: 1857-9655 Global Dermatology Immunocompromised Districts of Skin: A Case Series and a Literature Review Aleksandra Vojvodic1, Michael Tirant2,3, Veronica di Nardo2, Torello Lotti2, Uwe Wollina4* 1Department of Dermatology and Venereology, Military Medical Academy of Belgrade, Belgrade, Serbia; 2Department of Dermatology, University of Rome “G. Marconi”, Rome, Italy; 3Hanoi Medical University, Hanoi, Vietnam; 4Department of Dermatology and Allergology, Städtisches Klinikum Dresden, Academic Teaching Hospital, Dresden, Germany Abstract Citation: Vojvodic A, Tirant M, di Nardo V, Lotti T, BACKGROUND: The concept of immunocompromised districts of skin has been developed by Ruocco and helps Wollina U. Immunocompromised Districts of Skin: A Case to explain certain aspects of the macromorphology of skin diseases. This concept unites the isomorphic response Series and a Literature Review. Open Access Maced J Med Sci. 2019 Sep 30; 7(18):2969-2975. of Koebner and the isotopic response of Wolf. https://doi.org/10.3889/oamjms.2019.680 Keywords: Immunocompromised districts of the skin; CASE REPORTS: We present different cutaneous conditions which can lead to immunocompromised districts of Macromorphology of skin diseases; Koebner skin such as scars, radiodermatitis, lymphedema, disturbed innervation or mechanical friction etc. Typical and phenomenon; Wolf’s isotopic response rarer skin disorders associated with them are discussed and illustrated by their observations. *Correspondence: Uwe Wollina. Department of Dermatology and Allergology, Städtisches Klinikum CONCLUSION: At this moment, we wish to inform dermatologists and non-dermatologists about Ruocco’s Dresden, Academic Teaching Hospital, 01067 Dresden, Germany. -

Prior Authorization Topical Retinoids – Tazarotene Products
Cigna National Formulary Coverage Policy Prior Authorization Topical Retinoids – Tazarotene Products Table of Contents Product Identifier(s) National Formulary Medical Necessity ................ 1 01541 Conditions Not Covered....................................... 2 Background .......................................................... 2 References .......................................................... 2 Revision History ................................................... 3 INSTRUCTIONS FOR USE The following Coverage Policy applies to health benefit plans administered by Cigna Companies. Certain Cigna Companies and/or lines of business only provide utilization review services to clients and do not make coverage determinations. References to standard benefit plan language and coverage determinations do not apply to those clients. Coverage Policies are intended to provide guidance in interpreting certain standard benefit plans administered by Cigna Companies. Please note, the terms of a customer’s particular benefit plan document [Group Service Agreement, Evidence of Coverage, Certificate of Coverage, Summary Plan Description (SPD) or similar plan document] may differ significantly from the standard benefit plans upon which these Coverage Policies are based. For example, a customer’s benefit plan document may contain a specific exclusion related to a topic addressed in a Coverage Policy. In the event of a conflict, a customer’s benefit plan document always supersedes the information in the Coverage Policies. In the absence of a controlling federal or state coverage mandate, benefits are ultimately determined by the terms of the applicable benefit plan document. Coverage determinations in each specific instance require consideration of 1) the terms of the applicable benefit plan document in effect on the date of service; 2) any applicable laws/regulations; 3) any relevant collateral source materials including Coverage Policies and; 4) the specific facts of the particular situation. -

A Review of the Evidence for and Against a Role for Mast Cells in Cutaneous Scarring and Fibrosis
International Journal of Molecular Sciences Review A Review of the Evidence for and against a Role for Mast Cells in Cutaneous Scarring and Fibrosis Traci A. Wilgus 1,*, Sara Ud-Din 2 and Ardeshir Bayat 2,3 1 Department of Pathology, Ohio State University, Columbus, OH 43210, USA 2 Centre for Dermatology Research, NIHR Manchester Biomedical Research Centre, Plastic and Reconstructive Surgery Research, University of Manchester, Manchester M13 9PT, UK; [email protected] (S.U.-D.); [email protected] (A.B.) 3 MRC-SA Wound Healing Unit, Division of Dermatology, University of Cape Town, Observatory, Cape Town 7945, South Africa * Correspondence: [email protected]; Tel.: +1-614-366-8526 Received: 1 October 2020; Accepted: 12 December 2020; Published: 18 December 2020 Abstract: Scars are generated in mature skin as a result of the normal repair process, but the replacement of normal tissue with scar tissue can lead to biomechanical and functional deficiencies in the skin as well as psychological and social issues for patients that negatively affect quality of life. Abnormal scars, such as hypertrophic scars and keloids, and cutaneous fibrosis that develops in diseases such as systemic sclerosis and graft-versus-host disease can be even more challenging for patients. There is a large body of literature suggesting that inflammation promotes the deposition of scar tissue by fibroblasts. Mast cells represent one inflammatory cell type in particular that has been implicated in skin scarring and fibrosis. Most published studies in this area support a pro-fibrotic role for mast cells in the skin, as many mast cell-derived mediators stimulate fibroblast activity and studies generally indicate higher numbers of mast cells and/or mast cell activation in scars and fibrotic skin. -

Fundamentals of Dermatology Describing Rashes and Lesions
Dermatology for the Non-Dermatologist May 30 – June 3, 2018 - 1 - Fundamentals of Dermatology Describing Rashes and Lesions History remains ESSENTIAL to establish diagnosis – duration, treatments, prior history of skin conditions, drug use, systemic illness, etc., etc. Historical characteristics of lesions and rashes are also key elements of the description. Painful vs. painless? Pruritic? Burning sensation? Key descriptive elements – 1- definition and morphology of the lesion, 2- location and the extent of the disease. DEFINITIONS: Atrophy: Thinning of the epidermis and/or dermis causing a shiny appearance or fine wrinkling and/or depression of the skin (common causes: steroids, sudden weight gain, “stretch marks”) Bulla: Circumscribed superficial collection of fluid below or within the epidermis > 5mm (if <5mm vesicle), may be formed by the coalescence of vesicles (blister) Burrow: A linear, “threadlike” elevation of the skin, typically a few millimeters long. (scabies) Comedo: A plugged sebaceous follicle, such as closed (whitehead) & open comedones (blackhead) in acne Crust: Dried residue of serum, blood or pus (scab) Cyst: A circumscribed, usually slightly compressible, round, walled lesion, below the epidermis, may be filled with fluid or semi-solid material (sebaceous cyst, cystic acne) Dermatitis: nonspecific term for inflammation of the skin (many possible causes); may be a specific condition, e.g. atopic dermatitis Eczema: a generic term for acute or chronic inflammatory conditions of the skin. Typically appears erythematous, -

Advances in Seborrheic Keratosis
A CME/CE-Certified Supplement to Original Release Date: December 2018 Advances in Seborrheic Expiration Date: December 31, 2020 Estimated Time To Complete Activity: 1 hour Participants should read the activity information, Keratosis review the activity in its entirety, and complete the online post-test and evaluation. Upon completing this activity as designed and achieving a passing score on FACULTY the post-test, you will be directed to a Web page that will Joseph F. Fowler Jr, MD Michael S. Kaminer, MD allow you to receive your certificate of credit via e-mail Clinical Professor and Director Associate Clinical Professor of Dermatology or you may print it out at that time. Contact and Occupational Yale Medical School The online post-test and evaluation can be accessed Dermatology New Haven, Connecticut at http://tinyurl.com/SebK2018. University of Louisville School of Adjunct Assistant Professor of Medicine Medicine (Dermatology), Warren Alpert Medical School Inquiries about continuing medical education (CME) Louisville, Kentucky of Brown University accreditation may be directed to the University of Providence, Rhode Island Louisville Office of Continuing Medical Education & Professional Development (CME & PD) at cmepd@ louisville.edu or (502) 852-5329. Designation Statement eborrheic keratosis (SK) has been called keratinizing surface.12 They can develop virtually The University of Louisville School of Medicine the “Rodney Dangerfield of skin lesions”— anywhere except for the palms, soles, and mucous designates this Enduring material for a maximum of 9 1.0 AMA PRA Category 1 Credit(s)™. Physicians should it earns little respect (as a clinical concern) membranes, but are most commonly observed claim only the credit commensurate with the extent of Sbecause of its benignity, commonality, usual on the trunk and face.6,13 The tendency to develop their participation in the activity. -

Case Report an Exophytic and Symptomatic Lesion of the Labial Mucosa Diagnosed As Labial Seborrheic Keratosis
Int J Clin Exp Pathol 2019;12(7):2749-2752 www.ijcep.com /ISSN:1936-2625/IJCEP0093949 Case Report An exophytic and symptomatic lesion of the labial mucosa diagnosed as labial seborrheic keratosis Hui Feng1,2, Binjie Liu1, Zhigang Yao1, Xin Zeng2, Qianming Chen2 1XiangYa Stomatological Hospital, Central South University, Changsha 410000, Hunan, P. R. China; 2State Key Laboratory of Oral Diseases, West China Hospital of Stomatology, Sichuan University, Chengdu 610041, Sichuan, P. R. China Received March 16, 2019; Accepted April 23, 2019; Epub July 1, 2019; Published July 15, 2019 Abstract: Seborrheic keratosis is a common benign epidermal tumor that occurs mainly in the skin of the face and neck, trunk. The tumors are not, however, seen on the oral mucous membrane. Herein, we describe a case of labial seborrheic keratosis confirmed by histopathology. A healthy 63-year-old man was referred to our hospital for evalu- ation and treatment of a 2-month history of a labial mass with mild pain. Clinically, the initial impressions were ma- lignant transformation of chronic discoid lupus erythematosus, syphilitic chancre, or keratoacanthoma. Surprisingly, our laboratory results and histopathologic evaluations established a novel diagnosis of a hyperkeratotic type of labial seborrheic keratosis (SK). This reminds us that atypical or varying features of seborrheic keratosis make it difficult to provide an accurate diagnosis. Clinical manifestations of some benign lesions may be misdiagnosed as malignancy. Consequently, dentists should consider this as a differential diagnosis in labial or other oral lesions. Keywords: Seborrheic keratosis, exophytic lesion, symptomatic lesion, labial mucosa, oral mucous membrane Introduction findings were revealed in his medical history, and he had no known allergies to foods or me- Seborrheic keratosis is a common benign epi- dications. -

Linear Scleroderma “En Coup De Sabre” Coexisting with Plaque-Morphea
661 J Neurol Neurosurg Psychiatry: first published as 10.1136/jnnp.74.5.661 on 1 May 2003. Downloaded from SHORT REPORT Linear scleroderma “en coup de sabre” coexisting with plaque-morphea: neuroradiological manifestation and response to corticosteroids I Unterberger, E Trinka, K Engelhardt, A Muigg, P Eller, M Wagner, N Sepp, G Bauer ............................................................................................................................. J Neurol Neurosurg Psychiatry 2003;74:661–664 progression of skin lesions or any neurological abnormalities A 24 year old woman in the 33rd week of pregnancy during follow up. developed progressive neurological complications with On admission the patient was in the 33rd week of right sided hemiparesis in association with the occurrence pregnancy. She was fully oriented, had normal speech, and of linear scleroderma “en coup de sabre” (LSCS) and pre- presented with a right sided hemiparesis (grade 3/5, MRC existing plaque-morphea, already being treated by scale) with a positive Babinski sign on the right. There was no balneophototherapy. Further progression of neurological history of head trauma. symptoms led to a caesarean section with the delivery of a Routine laboratory testing and comprehensive serological healthy child. Brain magnetic resonance imaging (MRI) screening including antineutrophilic cytoplasmic antibodies showed focal T2 signal increases in the left frontoparietal (ANCA), anticardiolipin antibodies, and antibodies against region directly adjacent to the area of LSCS. -
Nodular Morphea
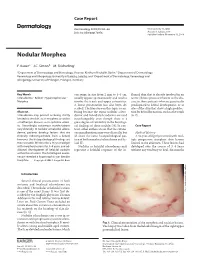
Case Report Dermatology 2009;218:63–66 Received: July 13, 2008 DOI: 10.1159/000173976 Accepted: July 23, 2008 Published online: November 13, 2008 Nodular Morphea a b c F. Kauer J.C. Simon M. Sticherling a b Department of Dermatology and Venerology, Vivantes Klinikum Neukölln, Berlin , Department of Dermatology, c Venerology and Allergology, University of Leipzig, Leipzig , and Department of Dermatology, Venerology and Allergology, University of Erlangen, Erlangen , Germany Key Words can range in size from 2 mm to 4–5 cm, flamed skin that is already involved in an -Scleroderma ؒ Keloid ؒ Hypertrophic scar ؒ usually appear spontaneously and tend to active fibrotic process inherent to the dis Morphea involve the trunk and upper extremities. ease in those patients who are genetically A linear presentation has also been de- predisposed to keloid development, or at scribed. The literature on this topic is con- sites of the skin that show a high predilec- Abstract fusing because the terms ‘nodular sclero- tion for keloid formation, such as the trunk Scleroderma may present as being strictly derma’ and ‘keloidal scleroderma’ are used [6, 7] . limited to the skin, as in morphea, or within interchangeably even though there is a a multiorgan disease, as in systemic sclero- great degree of variability in the histologi- sis. Accordingly, cutaneous manifestations cal findings of these nodules [4] . In con- C a s e R e p o r t vary clinically. In nodular or keloidal sclero- trast, other authors stress that the cutane- derma, patients develop lesions that are ous manifestations may vary clinically, but Medical History clinically indistinguishable from a keloid; all share the same histopathological pat- A 16-year-old girl presented with mul- however, the histopathological findings are tern of both morphea/scleroderma and ke- tiple progressive morpheic skin lesions more variable. -

Acanthosis Nigricans As a Presentation of Severe Insulin
Acanthosis nigricans as a presentation of severe insulin resistance in obese children - a case report - Maria Krajewska, Jędrzej Nowaczyk, Dominika Labochka, Anna Kucharska, Beata Pyrżak Department of Paediatrics and Endocrinology, Medical University of Warsaw, Poland Acanthosis nigricans • Acanthosis nigricans is well known as the skin symptom of insulin resistance, nevertheless children with such skin disorders usually undergo a long way until they are properly diagnosed. • We would like to present the history of two young patients with severe acanthosis nigricans combined with insulin resistance of major grade. Patient 1 Patient 2 A 13-year-old boy referred to the Clinic by dermatologist due to acanthosis nigricans and obesity. A 14-year-old boy referred to the Clinic by general pediatrician due to acanthosis nigricans and obesity. Medical history: Medical history: •born with the forces of nature, from uncomplicated pregnancy, 40 weeks, with body weight 2700g. Delayed • born from uncomplicated pregnancy with the forces of nature, 38 weeks, body psychomotor development since the infancy period. Negative history of chronic diseases and taking weight 3100g, length 51 cm, in infancy fed with modified milk, negative history medications of chronic diseases and taking medications •excessive body weight from the early childhood: • excessive body weight from the age of five: frequent and irregular eating insufficient physical activity frequent and irregular eating, large amounts of sweets and sweet drinks (up to •family history: grandmother suffers from type 2 diabetes, brother is suffering from autism, negative history of 4-5 liters per day), insufficient physical activity; familial acanthosis nigricans and obesity acanthosis nigricans was noticed at the age of 12 years.