Muscles of the Back Editing File Objectives
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
The Structure and Function of Breathing
CHAPTERCONTENTS The structure-function continuum 1 Multiple Influences: biomechanical, biochemical and psychological 1 The structure and Homeostasis and heterostasis 2 OBJECTIVE AND METHODS 4 function of breathing NORMAL BREATHING 5 Respiratory benefits 5 Leon Chaitow The upper airway 5 Dinah Bradley Thenose 5 The oropharynx 13 The larynx 13 Pathological states affecting the airways 13 Normal posture and other structural THE STRUCTURE-FUNCTION considerations 14 Further structural considerations 15 CONTINUUM Kapandji's model 16 Nowhere in the body is the axiom of structure Structural features of breathing 16 governing function more apparent than in its Lung volumes and capacities 19 relation to respiration. This is also a region in Fascla and resplrstory function 20 which prolonged modifications of function - Thoracic spine and ribs 21 Discs 22 such as the inappropriate breathing pattern dis- Structural features of the ribs 22 played during hyperventilation - inevitably intercostal musculature 23 induce structural changes, for example involving Structural features of the sternum 23 Posterior thorax 23 accessory breathing muscles as well as the tho- Palpation landmarks 23 racic articulations. Ultimately, the self-perpetuat- NEURAL REGULATION OF BREATHING 24 ing cycle of functional change creating structural Chemical control of breathing 25 modification leading to reinforced dysfunctional Voluntary control of breathing 25 tendencies can become complete, from The autonomic nervous system 26 whichever direction dysfunction arrives, for Sympathetic division 27 Parasympathetic division 27 example: structural adaptations can prevent NANC system 28 normal breathing function, and abnormal breath- THE MUSCLES OF RESPIRATION 30 ing function ensures continued structural adap- Additional soft tissue influences and tational stresses leading to decompensation. -

Thoracic and Lumbar Spine Anatomy
ThoracicThoracic andand LumbarLumbar SpineSpine AnatomyAnatomy www.fisiokinesiterapia.biz ThoracicThoracic VertebraeVertebrae Bodies Pedicles Laminae Spinous Processes Transverse Processes Inferior & Superior Facets Distinguishing Feature – Costal Fovea T1 T2-T8 T9-12 ThoracicThoracic VertebraeVertebrae andand RibRib JunctionJunction FunctionsFunctions ofof ThoracicThoracic SpineSpine – Costovertebral Joint – Costotransverse Joint MotionsMotions – All available – Flexion and extension limited – T7-T12 LumbarLumbar SpineSpine BodiesBodies PediclesPedicles LaminaeLaminae TransverseTransverse ProcessProcess SpinousSpinous ProcessProcess ArticularArticular FacetsFacets LumbarLumbar SpineSpine ThoracolumbarThoracolumbar FasciaFascia LumbarLumbar SpineSpine IliolumbarIliolumbar LigamentsLigaments FunctionsFunctions ofof LumbarLumbar SpineSpine – Resistance of anterior translation – Resisting Rotation – Weight Support – Motion IntervertebralIntervertebral DisksDisks RatioRatio betweenbetween diskdisk thicknessthickness andand vertebralvertebral bodybody heightheight DiskDisk CompositionComposition – Nucleus pulposis – Annulus Fibrosis SpinalSpinal LigamentsLigaments AnteriorAnterior LongitudinalLongitudinal PosteriorPosterior LongitudinalLongitudinal LigamentumLigamentum FlavumFlavum InterspinousInterspinous LigamentsLigaments SupraspinousSupraspinous LigamentsLigaments IntertransverseIntertransverse LigamentsLigaments SpinalSpinal CurvesCurves PosteriorPosterior ViewView SagittalSagittal ViewView – Primary – Secondary -

Trunk Control During Gait: Walking with Wide and Narrow Step Widths Present Distinct 4 Challenges 5 6 Hai-Jung Steffi Shih, James Gordon, Kornelia Kulig
bioRxiv preprint doi: https://doi.org/10.1101/2020.08.30.274423; this version posted November 17, 2020. The copyright holder for this preprint (which was not certified by peer review) is the author/funder, who has granted bioRxiv a license to display the preprint in perpetuity. It is made available under aCC-BY-NC-ND 4.0 International license. 1 Original Article 2 3 Trunk Control during Gait: Walking with Wide and Narrow Step Widths Present Distinct 4 Challenges 5 6 Hai-Jung Steffi Shih, James Gordon, Kornelia Kulig 7 Division of Biokinesiology and Physical Therapy, University of Southern California, Los Angeles, 8 CA, USA 9 10 11 Corresponding Author: 12 Hai-Jung Steffi Shih 13 Address: 1540 E. Alcazar St, CHP 155, Los Angeles, CA, 90033 14 Telephone: +1 (323)442-2089 15 Fax: +1 (323)442-1515 16 Email: [email protected] 17 18 19 Keywords: Gait stability, Lateral stability, Trunk coordination, Muscle activation, Foot placement 20 Word count (intro-discussion): 3519 21 1 bioRxiv preprint doi: https://doi.org/10.1101/2020.08.30.274423; this version posted November 17, 2020. The copyright holder for this preprint (which was not certified by peer review) is the author/funder, who has granted bioRxiv a license to display the preprint in perpetuity. It is made available under aCC-BY-NC-ND 4.0 International license. 22 Abstract 23 The active control of the trunk plays an important role in frontal plane gait stability. We 24 characterized trunk control in response to different step widths using a novel feedback system 25 and examined the different effects of wide and narrow step widths as they each present unique 26 task demands. -

Indications and Treatment of Myofascial Pain
2/25/2017 Indications and Treatment of Myofascial Pain Lisa DeStefano, DO Associate Professor and Chair Department of Osteopathic Manipulative Medicine College of Osteopathic Medicine Michigan State University Common Myofascial Pain Syndromes 1 2/25/2017 2 2/25/2017 Greater Occipital Nerve Impingement Sites . 1: Origin of the third occipital nerve and proximal connection with the greater occipital nerve. 2: Greater occipital nerve as it courses inferior to the inferior oblique muscle. 3: Greater occipital nerve coursing through the semispinalis capitis muscle. 4: Greater occipital nerve exiting the aponeurosis of the trapezius muscle. 5: Greater occipital nerve traveling with the occipital artery. 6: Origin of the greater occipital nerve and relationship to the descending branch of the occipital artery. 7: Suboccipital nerve relation to the vertebral artery and the descending branch of the occipital artery and this nerves interconnection to the greater occipital nerve. 8: Relationship between the third occipital nerve and the C2‐C3 joint complex. Common Treatment Approaches • MFR • MET • Soft Tissue Release • Counterstain • HVLA Etiology of Head and Neck Myofascial Pain Syndromes • Overuse • Posture –Head over the pelvis • Posture – Scapular function • Occlusion –how the teeth control for the proper placement of the mandibular condyle. 3 2/25/2017 Stabilization of the torsobegins with spinotransverse muscle transmission of force onto the epaxial fascia or vertebral aponeurosis. 4 2/25/2017 This then transmits tension into the serratus posterior superior and inferior, which then lifts the upper four ribs and sternum and lowers the lower ribs respectively. In response a force‐ couple is generated between the serratus posterior inferior fascia, external oblique fascia, and the rectus sheath. -

Isolated Trapezoid Fractures a Case Report with Compilation of the Literature
Bulletin of the NYU Hospital for Joint Diseases 2008;66(1):57-60 57 Isolated Trapezoid Fractures A Case Report with Compilation of the Literature Konrad I. Gruson, M.D., Kevin M. Kaplan, M.D., and Nader Paksima, D.O., M.P.H. Abstract as an axial load5,6 or bending stress7 transmitted indirectly Isolated fractures of the trapezoid bone have been rarely to the trapezoid through the second metacarpal. We present reported in the literature, the mechanism of injury being a case of an acute, isolated trapezoid fracture that resulted an axial or bending load transmitted through the second from direct trauma to the distal carpus and that was treated metacarpal. We report a case of an isolated, nondisplaced nonoperatively. Additionally, strategies for diagnosis and trapezoid fracture that was sustained by direct trauma treatment, as well as a synthesis of the published results and subsequently treated successfully in a short-arm cast. for both isolated and concomitant trapezoid fractures, are Diagnostic and treatment strategies for isolated fractures presented. of the trapezoid bone are reviewed as well as the results of operative and nonoperative treatment. Case Report A 25-year-old right-hand dominant male presented to the ractures of the carpus most commonly involve the emergency room (ER) complaining of isolated right-wrist scaphoid,1 with typical physical examination findings pain and swelling of 1 day’s duration. The patient stated Fof “snuffbox” tenderness. This presentation is fre- that a heavy metal door at work had closed onto the back quently the result of the patient falling onto an outstretched of his wrist causing an immediate onset of swelling and hand. -

Active Release Techniques Spine Level 2
Active Release Techniques Spine Level 2 Dates of program- Montvale, NJ February 18-21, 2021 Colorado Springs, CO March 4-7, 2021 Orlando, FL June 10-13, 2021 Chicago, IL September 30 – October 3, 2021 Total Hours: 24 Summary: Active Release Techniques® Spine Level 2 offers intense training in 75 manual treatment protocols of the cervical, thoracic, and lumbar spine. ART® treatment utilizes manual techniques to move tissues and joints while under tension. The system allows for relative motion between the tissues and articulations. This seminar emphasizes the manipulation of the neuromusculoskeletal system to diagnose and correct alterations in tissue texture, tension, movement, and function between tissues. Evaluation and treatment occur simultaneously. Learning Outcomes: 1. By the end of the seminar, learners will be able to correctly identify (palpate) 75 facial seams of soft-tissue structures within the spine. 2. By the end of the seminars, learners will be able to correctly state the muscle actions of two adjacent spinal muscles. 3. By the end of the seminar, learners will be able to effectively recognize common symptom patterns of spinal neuromuscular injuries and disorders. 4. By the end of the seminar, learners will correctly identify the structure treated and associated concentric and eccentric muscle actions via video presentations. 5. By the end of the seminar, the learner will correctly move the muscle from its shortened position to elongated position using two-hand placement techniques. 6. By the end of the seminar, the learner can successfully differentiate between healthy and unhealthy tissue utilizing hands-on palpation techniques. 7. By the end of the seminar, the learner will proficiently palpate 75 anatomical soft-tissue structures within the spine, using an appropriate tension, depth, and motion to properly perform the treatment protocol. -

Familial Absenceof the Pectoralis Major, Serratus Anterior, And
J Med Genet: first published as 10.1136/jmg.22.5.390 on 1 October 1985. Downloaded from Journal of Medical Genetics, 1985, 22, 390-392 Familial absence of the pectoralis major, serratus anterior, and latissimus dorsi muscles T J DAVID* AND R M WINTERt From *the Department of Child Health, University ofManchester; and tthe Kennedy-Galton Centrefor Clinical Genetics, Harperbury Hospital, Hertfordshire. SUMMARY Congenital absence of shoulder girdle muscles is described in three generations of a family. The proband, a 3 year old boy, had absence of the sternocostal head of the right pectoralis major. His father had absence of the left serratus anterior and part of the left latissimus dorsi and his paternal grandfather had absence of the lower two-thirds of the left pectoralis major, with absence of the left serratus anterior and latissimus dorsi muscles. The condition is probably the result of a dominant gene. These observations show that absence of the pectoralis major is part of a wider spectrum of shoulder girdle defects. Where genetic advice is sought by persons with apparently sporadic absence of the pectoralis major, examination of the relatives is necessary. The Poland anomaly comprises unilateral absence of of the Poland anomaly or isolated absence of the the pectoralis major combined with an ipsilateral pectoralis. The pedigree is shown in fig 1. malformation of the hand which usually includes syndactyly. It is currently unclear whether isolated Case reports absence of the pectoralis major muscle and the CASE 1 Poland anomaly are part of the same spectrum of IV.3 was a male infant, the product of the first defects or are separate entities.1 Both are consis- 30 year old http://jmg.bmj.com/ tently unilateral and both are usually sporadic pregnancy of a 29 year old mother and 2 father, who had been married for seven years. -

Bone Limb Upper
Shoulder Pectoral girdle (shoulder girdle) Scapula Acromioclavicular joint proximal end of Humerus Clavicle Sternoclavicular joint Bone: Upper limb - 1 Scapula Coracoid proc. 3 angles Superior Inferior Lateral 3 borders Lateral angle Medial Lateral Superior 2 surfaces 3 processes Posterior view: Acromion Right Scapula Spine Coracoid Bone: Upper limb - 2 Scapula 2 surfaces: Costal (Anterior), Posterior Posterior view: Costal (Anterior) view: Right Scapula Right Scapula Bone: Upper limb - 3 Scapula Glenoid cavity: Glenohumeral joint Lateral view: Infraglenoid tubercle Right Scapula Supraglenoid tubercle posterior anterior Bone: Upper limb - 4 Scapula Supraglenoid tubercle: long head of biceps Anterior view: brachii Right Scapula Bone: Upper limb - 5 Scapula Infraglenoid tubercle: long head of triceps brachii Anterior view: Right Scapula (with biceps brachii removed) Bone: Upper limb - 6 Posterior surface of Scapula, Right Acromion; Spine; Spinoglenoid notch Suprspinatous fossa, Infraspinatous fossa Bone: Upper limb - 7 Costal (Anterior) surface of Scapula, Right Subscapular fossa: Shallow concave surface for subscapularis Bone: Upper limb - 8 Superior border Coracoid process Suprascapular notch Suprascapular nerve Posterior view: Right Scapula Bone: Upper limb - 9 Acromial Clavicle end Sternal end S-shaped Acromial end: smaller, oval facet Sternal end: larger,quadrangular facet, with manubrium, 1st rib Conoid tubercle Trapezoid line Right Clavicle Bone: Upper limb - 10 Clavicle Conoid tubercle: inferior -
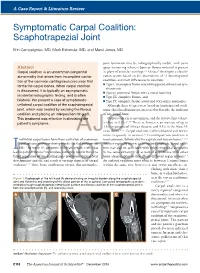
Symptomatic Carpal Coalition: Scaphotrapezial Joint
A Case Report & Literature Review E. Campaigniac et al Symptomatic Carpal Coalition: Scaphotrapezial Joint Erin Campaigniac, MD, Mark Eskander, MD, and Marci Jones, MD joint formation may be radiographically visible, with joint Abstract space narrowing wherein bone or fibrous material is present Carpal coalition is an uncommon congenital in place of articular cartilage.2,4 Minaar8 developed a classifi- abnormality that arises from incomplete cavita- cation system based on his observations of 12 lunotriquetral tion of the common cartilaginous precursor that coalitions and their differences in coalition: ◾ Type I, incomplete fusion resembling pseudarthrosis or syn- forms the carpal bones. When carpal coalition chondrosis is discovered, it is typically an asymptomatic ◾ Type II, proximal fusion with a distal notching incidental radiographic finding, and is often ◾ Type III, complete fusion, and bilateral. We present a case of symptomatic ◾ Type IV, complete fusion associated with other anomalies. unilateral carpal coalition of the scaphotrapezial Although these 4 types were based on lunotriquetral coali- joint, which was treated by excising the fibrous tions, this classification system is used to describe the coalition coalition and placing an interposition fat graft. of any carpal bone. This treatment was effective in alleviating the Carpal coalition is uncommon, and the reported prevalence 2,5,6,9 patient’s symptoms. is close to 0.1%. There is, however, an increase of up to 1.5% in patients of African descent, and 9.5% in the West Af- rican -

Trapezius Origin: Occipital Bone, Ligamentum Nuchae & Spinous Processes of Thoracic Vertebrae Insertion: Clavicle and Scapul
Origin: occipital bone, ligamentum nuchae & spinous processes of thoracic vertebrae Insertion: clavicle and scapula (acromion Trapezius and scapular spine) Action: elevate, retract, depress, or rotate scapula upward and/or elevate clavicle; extend neck Origin: spinous process of vertebrae C7-T1 Rhomboideus Insertion: vertebral border of scapula Minor Action: adducts & performs downward rotation of scapula Origin: spinous process of superior thoracic vertebrae Rhomboideus Insertion: vertebral border of scapula from Major spine to inferior angle Action: adducts and downward rotation of scapula Origin: transverse precesses of C1-C4 vertebrae Levator Scapulae Insertion: vertebral border of scapula near superior angle Action: elevates scapula Origin: anterior and superior margins of ribs 1-8 or 1-9 Insertion: anterior surface of vertebral Serratus Anterior border of scapula Action: protracts shoulder: rotates scapula so glenoid cavity moves upward rotation Origin: anterior surfaces and superior margins of ribs 3-5 Insertion: coracoid process of scapula Pectoralis Minor Action: depresses & protracts shoulder, rotates scapula (glenoid cavity rotates downward), elevates ribs Origin: supraspinous fossa of scapula Supraspinatus Insertion: greater tuberacle of humerus Action: abduction at the shoulder Origin: infraspinous fossa of scapula Infraspinatus Insertion: greater tubercle of humerus Action: lateral rotation at shoulder Origin: clavicle and scapula (acromion and adjacent scapular spine) Insertion: deltoid tuberosity of humerus Deltoid Action: -

Meat Quality Workshop: Know Your Muscle, Know Your Meat BEEF
2/6/2017 Meat Quality Workshop: Know Your Muscle, Know Your Meat Principles of Muscle Profiling, Aging, and Nutrition Dale R. Woerner, Ph.D., Colorado State University BEEF- Determining Value 1 2/6/2017 Slight00 Small00 Modest00 Moderate00 SLAB00 MAB00 ACE ABC Maturity Group Approximate Age A 9‐30 months B 30‐42 months C 42‐72 months D E 72‐96 months 96 months or older Augmentation of USDA Grade Application 2 2/6/2017 Effect of Marbling Degree on Probability of a Positive Sensory Experience Probability of a Positive Sensory Experience 0.99a 0.98a 1 0.88b 0.9 0.82b 0.8 0.7 0.62c 0.6 0.5 0.4 0.29d 0.3 0.2 0.15e 0.1 0 TR SL SM MT MD SA MA Colorado State University M.S. Thesis: M. R. Emerson (2011) 3 2/6/2017 Carcass Weight Trend 900 All Fed Cattle CAB® 875 850 +55 lbs. in 5 years 825 +11 lbs. / year 800 775 750 +117 lbs. in 20 years Hot Carcass (lbs.) Weight +5.8 lbs. / year 725 Year 4 2/6/2017 Further Problems • Food service portion cutting problems = 8 oz. • Steak preparation problems = 8 oz. A 1,300‐pound, Yield Grade 3 steer yields 639 pounds of retail cuts from an 806‐pound carcass. Of the retail cuts, 62% are roasts and steaks (396 pounds) and 38% are ground beef and stew meat (243 pounds). 5 2/6/2017 Objective of Innovative Fabrication • Use quality-based break points during fabrication • Add value to beef by optimizing use of high-quality cuts • Add value to beef cuts by improving leanness and portion size $2.25 $7.56 $2.75 $4.66 $2.50 $12.73 $2.31 $2.85 $3.57 $1.99 Aging Response Premium USDA Choice USDA Select Muscle Aging response -

Effect of Latissimus Dorsi Muscle Strengthening in Mechanical Low Back Pain
International Journal of Science and Research (IJSR) ISSN: 2319-7064 ResearchGate Impact Factor (2018): 0.28 | SJIF (2019): 7.583 Effect of Latissimus Dorsi Muscle Strengthening in Mechanical Low Back Pain 1 2 Vishakha Vishwakarma , Dr. P. R. Suresh 1, 2PCPS & RC, People’s University, Bhopal (M.P.), India Abstract: Mechanical low back pain (MLBP) is one of the most common musculoskeletal pain syndromes, affecting up to 80% of people at some point during their lifetime. Sources of back pain are numerous, usually sought in as lesion of disc or facet joints at L4- L5 and L5-S1 levels. Studies have shown that 40% of all back pain is of thoracolumbar origin. The term meachnical low back pain also gives reassurance that there is no damage to the nerves or spinal pathology. The clinical presentation of mechanical low back pain usually the ages 18-55 years is in the lumbo sacral region. A study was conducted to evaluate the designed to check the effectiveness of Conventional Exercises alone in Mechanical low back pain and along with the latissimus dorsi muscle strengthening, data was collected from People’s hospital, Bhopal (age group-30-45 yr both male and female randomly) Keywords: Visual analog scale, Assessment chart, Treatment table, Data collection sheets, Essential stationery materials, Computer, SPSS Software etc. 1. Introduction Back pain is a primary to seek medical advice considering 80% of people suffering from back pain. Mechanical low back pain is defined as a result of minor intervertebral dysfunction and referred pain in the low back The latissimus dorsi is a large, flat muscle on the back that and hip region, and can often be confused with the other stretches to the sides, behind the arm, and is partly covered pathologies that may cause these symptoms.18 by the trapezius on the back near the midline, the word latissimus dorsi comes from Latin and its means, broadest muscle of the back dorsum means back.