EMG Analysis of Latissimus Dorsi, Erector Spinae and Middle Trapezius Muscle Activity During Spinal Rotation: a Pilot Study Jamie Flint University of North Dakota
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
The Structure and Function of Breathing
CHAPTERCONTENTS The structure-function continuum 1 Multiple Influences: biomechanical, biochemical and psychological 1 The structure and Homeostasis and heterostasis 2 OBJECTIVE AND METHODS 4 function of breathing NORMAL BREATHING 5 Respiratory benefits 5 Leon Chaitow The upper airway 5 Dinah Bradley Thenose 5 The oropharynx 13 The larynx 13 Pathological states affecting the airways 13 Normal posture and other structural THE STRUCTURE-FUNCTION considerations 14 Further structural considerations 15 CONTINUUM Kapandji's model 16 Nowhere in the body is the axiom of structure Structural features of breathing 16 governing function more apparent than in its Lung volumes and capacities 19 relation to respiration. This is also a region in Fascla and resplrstory function 20 which prolonged modifications of function - Thoracic spine and ribs 21 Discs 22 such as the inappropriate breathing pattern dis- Structural features of the ribs 22 played during hyperventilation - inevitably intercostal musculature 23 induce structural changes, for example involving Structural features of the sternum 23 Posterior thorax 23 accessory breathing muscles as well as the tho- Palpation landmarks 23 racic articulations. Ultimately, the self-perpetuat- NEURAL REGULATION OF BREATHING 24 ing cycle of functional change creating structural Chemical control of breathing 25 modification leading to reinforced dysfunctional Voluntary control of breathing 25 tendencies can become complete, from The autonomic nervous system 26 whichever direction dysfunction arrives, for Sympathetic division 27 Parasympathetic division 27 example: structural adaptations can prevent NANC system 28 normal breathing function, and abnormal breath- THE MUSCLES OF RESPIRATION 30 ing function ensures continued structural adap- Additional soft tissue influences and tational stresses leading to decompensation. -

Thoracic and Lumbar Spine Anatomy
ThoracicThoracic andand LumbarLumbar SpineSpine AnatomyAnatomy www.fisiokinesiterapia.biz ThoracicThoracic VertebraeVertebrae Bodies Pedicles Laminae Spinous Processes Transverse Processes Inferior & Superior Facets Distinguishing Feature – Costal Fovea T1 T2-T8 T9-12 ThoracicThoracic VertebraeVertebrae andand RibRib JunctionJunction FunctionsFunctions ofof ThoracicThoracic SpineSpine – Costovertebral Joint – Costotransverse Joint MotionsMotions – All available – Flexion and extension limited – T7-T12 LumbarLumbar SpineSpine BodiesBodies PediclesPedicles LaminaeLaminae TransverseTransverse ProcessProcess SpinousSpinous ProcessProcess ArticularArticular FacetsFacets LumbarLumbar SpineSpine ThoracolumbarThoracolumbar FasciaFascia LumbarLumbar SpineSpine IliolumbarIliolumbar LigamentsLigaments FunctionsFunctions ofof LumbarLumbar SpineSpine – Resistance of anterior translation – Resisting Rotation – Weight Support – Motion IntervertebralIntervertebral DisksDisks RatioRatio betweenbetween diskdisk thicknessthickness andand vertebralvertebral bodybody heightheight DiskDisk CompositionComposition – Nucleus pulposis – Annulus Fibrosis SpinalSpinal LigamentsLigaments AnteriorAnterior LongitudinalLongitudinal PosteriorPosterior LongitudinalLongitudinal LigamentumLigamentum FlavumFlavum InterspinousInterspinous LigamentsLigaments SupraspinousSupraspinous LigamentsLigaments IntertransverseIntertransverse LigamentsLigaments SpinalSpinal CurvesCurves PosteriorPosterior ViewView SagittalSagittal ViewView – Primary – Secondary -

The Erector Spinae Plane Block a Novel Analgesic Technique in Thoracic Neuropathic Pain
CHRONIC AND INTERVENTIONAL PAIN BRIEF TECHNICAL REPORT The Erector Spinae Plane Block A Novel Analgesic Technique in Thoracic Neuropathic Pain Mauricio Forero, MD, FIPP,*Sanjib D. Adhikary, MD,† Hector Lopez, MD,‡ Calvin Tsui, BMSc,§ and Ki Jinn Chin, MBBS (Hons), MMed, FRCPC|| Case 1 Abstract: Thoracic neuropathic pain is a debilitating condition that is often poorly responsive to oral and topical pharmacotherapy. The benefit A 67-year-old man, weight 116 kg and height 188 cm [body of interventional nerve block procedures is unclear due to a paucity of ev- mass index (BMI), 32.8 kg/m2] with a history of heavy smoking idence and the invasiveness of the described techniques. In this report, we and paroxysmal supraventricular tachycardia controlled on ateno- describe a novel interfascial plane block, the erector spinae plane (ESP) lol, was referred to the chronic pain clinic with a 4-month history block, and its successful application in 2 cases of severe neuropathic pain of severe left-sided chest pain. A magnetic resonance imaging (the first resulting from metastatic disease of the ribs, and the second from scan of his thorax at initial presentation had been reported as nor- malunion of multiple rib fractures). In both cases, the ESP block also pro- mal, and the working diagnosis at the time of referral was post- duced an extensive multidermatomal sensory block. Anatomical and radio- herpetic neuralgia. He reported constant burning and stabbing logical investigation in fresh cadavers indicates that its likely site of action neuropathic pain of 10/10 severity on the numerical rating score is at the dorsal and ventral rami of the thoracic spinal nerves. -

Active Release Techniques Spine Level 2
Active Release Techniques Spine Level 2 Dates of program- Montvale, NJ February 18-21, 2021 Colorado Springs, CO March 4-7, 2021 Orlando, FL June 10-13, 2021 Chicago, IL September 30 – October 3, 2021 Total Hours: 24 Summary: Active Release Techniques® Spine Level 2 offers intense training in 75 manual treatment protocols of the cervical, thoracic, and lumbar spine. ART® treatment utilizes manual techniques to move tissues and joints while under tension. The system allows for relative motion between the tissues and articulations. This seminar emphasizes the manipulation of the neuromusculoskeletal system to diagnose and correct alterations in tissue texture, tension, movement, and function between tissues. Evaluation and treatment occur simultaneously. Learning Outcomes: 1. By the end of the seminar, learners will be able to correctly identify (palpate) 75 facial seams of soft-tissue structures within the spine. 2. By the end of the seminars, learners will be able to correctly state the muscle actions of two adjacent spinal muscles. 3. By the end of the seminar, learners will be able to effectively recognize common symptom patterns of spinal neuromuscular injuries and disorders. 4. By the end of the seminar, learners will correctly identify the structure treated and associated concentric and eccentric muscle actions via video presentations. 5. By the end of the seminar, the learner will correctly move the muscle from its shortened position to elongated position using two-hand placement techniques. 6. By the end of the seminar, the learner can successfully differentiate between healthy and unhealthy tissue utilizing hands-on palpation techniques. 7. By the end of the seminar, the learner will proficiently palpate 75 anatomical soft-tissue structures within the spine, using an appropriate tension, depth, and motion to properly perform the treatment protocol. -

Familial Absenceof the Pectoralis Major, Serratus Anterior, And
J Med Genet: first published as 10.1136/jmg.22.5.390 on 1 October 1985. Downloaded from Journal of Medical Genetics, 1985, 22, 390-392 Familial absence of the pectoralis major, serratus anterior, and latissimus dorsi muscles T J DAVID* AND R M WINTERt From *the Department of Child Health, University ofManchester; and tthe Kennedy-Galton Centrefor Clinical Genetics, Harperbury Hospital, Hertfordshire. SUMMARY Congenital absence of shoulder girdle muscles is described in three generations of a family. The proband, a 3 year old boy, had absence of the sternocostal head of the right pectoralis major. His father had absence of the left serratus anterior and part of the left latissimus dorsi and his paternal grandfather had absence of the lower two-thirds of the left pectoralis major, with absence of the left serratus anterior and latissimus dorsi muscles. The condition is probably the result of a dominant gene. These observations show that absence of the pectoralis major is part of a wider spectrum of shoulder girdle defects. Where genetic advice is sought by persons with apparently sporadic absence of the pectoralis major, examination of the relatives is necessary. The Poland anomaly comprises unilateral absence of of the Poland anomaly or isolated absence of the the pectoralis major combined with an ipsilateral pectoralis. The pedigree is shown in fig 1. malformation of the hand which usually includes syndactyly. It is currently unclear whether isolated Case reports absence of the pectoralis major muscle and the CASE 1 Poland anomaly are part of the same spectrum of IV.3 was a male infant, the product of the first defects or are separate entities.1 Both are consis- 30 year old http://jmg.bmj.com/ tently unilateral and both are usually sporadic pregnancy of a 29 year old mother and 2 father, who had been married for seven years. -

Quantification of the Elastic Moduli of Lumbar Erector Spinae And
applied sciences Article Quantification of the Elastic Moduli of Lumbar Erector Spinae and Multifidus Muscles Using Shear-Wave Ultrasound Elastography Tae Hyun Lim 1, Deukhee Lee 2,3 , Olga Kim 1,3 and Song Joo Lee 1,3,* 1 Center for Bionics, Biomedical Research Institute, Korea Institute of Science and Technology, Seoul 02792, Korea; [email protected] (T.H.L.); [email protected] (O.K.) 2 Center for Healthcare Robotics, AI and Robot Institute, Korea Institute of Science and Technology, Seoul 02792, Korea; [email protected] 3 Division of Bio-Medical Science and Technology, KIST School, Korea University of Science and Technology, Seoul 02792, Korea * Correspondence: [email protected]; Tel.: +82-2-958-5645 Featured Application: The findings and approach can potentially be used to guide surgical train- ing and planning for developing a minimal-incision surgical procedure by considering surgical position-dependent muscle material properties. Abstract: Although spinal surgeries with minimal incisions and a minimal amount of X-ray exposure (MIMA) mostly occur in a prone posture on a Wilson table, the prone posture’s effects on spinal muscles have not been investigated. Thus, this study used ultrasound shear-wave elastography (SWE) to compare the material properties of the erector spinae and multifidus muscles when subjects lay on the Wilson table used for spinal surgery and the flat table as a control condition. Thirteen male subjects participated in the study. Using ultrasound SWE, the shear elastic moduli (SEM) of the Citation: Lim, T.H.; Lee, D.; Kim, O.; Lee, S.J. Quantification of the Elastic erector spinae and multifidus muscles were investigated. -
Measurements of the Trapezius and Erector Spinae Muscles Using Virtual Touch Imaging Quantification Ultrasound-Elastography
Heizelmann et al. BMC Musculoskeletal Disorders (2017) 18:370 DOI 10.1186/s12891-017-1733-8 RESEARCHARTICLE Open Access Measurements of the trapezius and erector spinae muscles using virtual touch imaging quantification ultrasound-Elastography: a cross section study Anne Heizelmann1, Sümeyra Tasdemir1, Julian Schmidberger1, Tilmann Gräter2, Wolfgang Kratzer1* and Beate Grüner3 Abstract Background: This study uses virtual touch imaging quantification (VTIQ) technology for the first time to conduct measurements of the trapezius and erector spinae muscles in a large study population. The significance of various influencing factors, such as age and sex, are also examined. Method: The study population comprised 278 subjects. The Siemens Acuson S3000 and VTIQ technology were used for measurements of the trapezius and erector spinae muscles (Siemens Healthcare, Erlangen, Germany). Results: The following mean values ± standard deviation were calculated: left trapezius: males 2.89 ± 0.38 m/s, females 2.71 ± 0.37 m/s; right trapezius: males 2.84 ± 0.41 m/s, females 2.70 ± 0.38 m/s; left erector spinae: males 2. 97 ± 0.50 m/s, females 2.81 ± 0.57 m/s; right erector spinae: males 3.00 ± 0.52 m/s, females 2.77 ± 0.59 m/s. A significant difference between male and female subjects was demonstrated both for the shear wave velocities of the trapezius and erector spinae as well as for the thickness of the trapezius muscle (p < 0.05). There was also a significant difference in muscle elasticity between subjects over 60 years of age and those under 60 (p < 0.05). Furthermore, the results indicate that regular physical activity has an effect on muscle elasticity. -

Erector Spinae Plane Block Versus Retrolaminar Block a Magnetic Resonance Imaging and Anatomical Study
Regional Anesthesia & Pain Medicine: first published as 10.1097/AAP.0000000000000798 on 1 October 2018. Downloaded from REGIONAL ANESTHESIA AND ACUTE PAIN BRIEF TECHNICAL REPORT Erector Spinae Plane Block Versus Retrolaminar Block A Magnetic Resonance Imaging and Anatomical Study Sanjib Das Adhikary, MD,* Stephanie Bernard, MD,† Hector Lopez, MD,‡ and Ki Jinn Chin, FRCPC§ As with the ESP block, it has been postulated that the clinical ef- Background and Objectives: The erector spinae plane (ESP) and fects of the retrolaminar block may be explained by spread of lo- retrolaminar blocks are ultrasound-guided techniques for thoracoabdominal cal anesthetic into the paravertebral space,6 but this mechanism wall analgesia involving injection into the musculofascial plane between has never been systematically investigated. However, there are the paraspinal back muscles and underlying thoracic vertebrae. The ESP significant anatomical and technical differences between the 2 block targets the tips of the transverse processes, whereas the retrolaminar techniques: the retrolaminar block targets the lamina instead of block targets the laminae. We investigated if there were differences in the transverse process, and thus the injection point is more medial injectate spread between the 2 techniques that would have implications and deeper. The muscle layer over the lamina and adjacent to the for their clinical effect. spinous processes is thicker, being composed of the spinalis portion Methods: The blocks were performed in 3 fresh cadavers. The ESP and of the erector spinae muscle group as well as the transversospinalis retrolaminar blocks were performed on opposite sides of each cadaver at muscle group, which comprises the multifidus, rotatores, semis- the T5 vertebral level. -

Trapezius Origin: Occipital Bone, Ligamentum Nuchae & Spinous Processes of Thoracic Vertebrae Insertion: Clavicle and Scapul
Origin: occipital bone, ligamentum nuchae & spinous processes of thoracic vertebrae Insertion: clavicle and scapula (acromion Trapezius and scapular spine) Action: elevate, retract, depress, or rotate scapula upward and/or elevate clavicle; extend neck Origin: spinous process of vertebrae C7-T1 Rhomboideus Insertion: vertebral border of scapula Minor Action: adducts & performs downward rotation of scapula Origin: spinous process of superior thoracic vertebrae Rhomboideus Insertion: vertebral border of scapula from Major spine to inferior angle Action: adducts and downward rotation of scapula Origin: transverse precesses of C1-C4 vertebrae Levator Scapulae Insertion: vertebral border of scapula near superior angle Action: elevates scapula Origin: anterior and superior margins of ribs 1-8 or 1-9 Insertion: anterior surface of vertebral Serratus Anterior border of scapula Action: protracts shoulder: rotates scapula so glenoid cavity moves upward rotation Origin: anterior surfaces and superior margins of ribs 3-5 Insertion: coracoid process of scapula Pectoralis Minor Action: depresses & protracts shoulder, rotates scapula (glenoid cavity rotates downward), elevates ribs Origin: supraspinous fossa of scapula Supraspinatus Insertion: greater tuberacle of humerus Action: abduction at the shoulder Origin: infraspinous fossa of scapula Infraspinatus Insertion: greater tubercle of humerus Action: lateral rotation at shoulder Origin: clavicle and scapula (acromion and adjacent scapular spine) Insertion: deltoid tuberosity of humerus Deltoid Action: -

Towards Defining Muscular Regions of Interest from Axial Magnetic Resonance Imaging with Anatomical Cross-Reference: Part II - Cervical Spine Musculature James M
Elliott et al. BMC Musculoskeletal Disorders (2018) 19:171 https://doi.org/10.1186/s12891-018-2074-y TECHNICAL ADVANCE Open Access Towards defining muscular regions of interest from axial magnetic resonance imaging with anatomical cross-reference: part II - cervical spine musculature James M. Elliott1,2,3* , Jon Cornwall4, Ewan Kennedy5, Rebecca Abbott2 and Rebecca J. Crawford6 Abstract Background: It has been suggested that the quantification of paravertebral muscle composition and morphology (e.g. size/shape/structure) with magnetic resonance imaging (MRI) has diagnostic, prognostic, and therapeutic potential in contributing to overall musculoskeletal health. If this is to be realised, then consensus towards standardised MRI methods for measuring muscular size/shape/structure are crucial to allow the translation of such measurements towards management of, and hopefully improved health for, those with some musculoskeletal conditions. Following on from an original paper detailing methods for measuring muscles traversing the lumbar spine, we propose new methods based on anatomical cross-reference that strive towards standardising MRI-based quantification of anterior and posterior cervical spine muscle composition. Methods: In this descriptive technical advance paper we expand our methods from the lumbar spine by providing a detailed examination of regional cervical spine muscle morphology, followed by a comprehensive description of the proposed technique defining muscle ROI from axial MRI. Cross-referencing cervical musculature and vertebral -

Effect of Latissimus Dorsi Muscle Strengthening in Mechanical Low Back Pain
International Journal of Science and Research (IJSR) ISSN: 2319-7064 ResearchGate Impact Factor (2018): 0.28 | SJIF (2019): 7.583 Effect of Latissimus Dorsi Muscle Strengthening in Mechanical Low Back Pain 1 2 Vishakha Vishwakarma , Dr. P. R. Suresh 1, 2PCPS & RC, People’s University, Bhopal (M.P.), India Abstract: Mechanical low back pain (MLBP) is one of the most common musculoskeletal pain syndromes, affecting up to 80% of people at some point during their lifetime. Sources of back pain are numerous, usually sought in as lesion of disc or facet joints at L4- L5 and L5-S1 levels. Studies have shown that 40% of all back pain is of thoracolumbar origin. The term meachnical low back pain also gives reassurance that there is no damage to the nerves or spinal pathology. The clinical presentation of mechanical low back pain usually the ages 18-55 years is in the lumbo sacral region. A study was conducted to evaluate the designed to check the effectiveness of Conventional Exercises alone in Mechanical low back pain and along with the latissimus dorsi muscle strengthening, data was collected from People’s hospital, Bhopal (age group-30-45 yr both male and female randomly) Keywords: Visual analog scale, Assessment chart, Treatment table, Data collection sheets, Essential stationery materials, Computer, SPSS Software etc. 1. Introduction Back pain is a primary to seek medical advice considering 80% of people suffering from back pain. Mechanical low back pain is defined as a result of minor intervertebral dysfunction and referred pain in the low back The latissimus dorsi is a large, flat muscle on the back that and hip region, and can often be confused with the other stretches to the sides, behind the arm, and is partly covered pathologies that may cause these symptoms.18 by the trapezius on the back near the midline, the word latissimus dorsi comes from Latin and its means, broadest muscle of the back dorsum means back. -
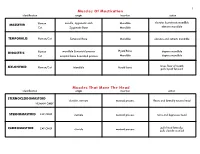
Muscles of Mastication Muscles That Move the Head
1 Muscles Of Mastication identification origin insertion action maxilla, zygomatic arch Mandible elevates & protracts mandible MASSETER Human Cat Zygomatic Bone Mandible elevates mandible TEMPORALIS Human/Cat Temporal Bone Mandible elevates and retracts mandible Hyoid Bone DIGASTRIC Human mandible & mastoid process depress mandible Cat occipital bone & mastoid process Mandible depress mandible raises floor of mouth; MYLOHYOID Human/Cat Mandible Hyoid bone pulls hyoid forward Muscles That Move The Head identification origin insertion action STERNOCLEIDOMAStoID clavicle, sternum mastoid process flexes and laterally rotates head HUMAN ONLY STERNOMAStoID CAT ONLY sternum mastoid process turns and depresses head pulls head laterally; CLEIDOMAStoID CAT ONLY clavicle mastoid process pulls clavicle craniad 2 Muscles Of The Hyoid, Larynx And Tongue identification origin insertion action Human Sternum Hyoid depresses hyoid bone STERNOHYOID Cat costal cartilage 1st rib Hyoid pulls hyoid caudally; raises ribs and sternum sternum Throid cartilage of larynx Human depresses thyroid cartilage STERNothYROID Cat costal cartilage 1st rib Throid cartilage of larynx pulls larynx caudad elevates thyroid cartilage and Human thyroid cartilage of larynx Hyoid THYROHYOID depresses hyoid bone Cat thyroid cartilage of larynx Hyoid raises larynx GENIOHYOID Human/Cat Mandible Hyoid pulls hyoid craniad 3 Muscles That Attach Pectoral Appendages To Vertebral Column identification origin insertion action Human Occipital bone; Thoracic and Cervical raises clavicle; adducts,