Hiding Within the Cracks: Case Report of Rare Sutural Bone Found at the Nasion
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

The Occipitomastoid Suture As a Novel Landmark to Identify The
The Occipitomastoid Suture as a Novel Landmark to Identify the Occipital Groove and Proximal Segment of the Occipital Artery Halima Tabani MD; Sirin Gandhi MD; Roberto Rodriguez Rubio MD; Michael T. Lawton MD; Arnau Benet M.D. University of California, San Francisco Introduction Results Conclusions The occipital artery (OA) is commonly used as a In 71.5% of the specimens the OA ran in a groove, The OMS is a key landmark for localizing the donor for posterior circulation bypass procedures. while it carved an impression in the rest of the proximal OA. The OMS can be followed inferiorly Localization of OA during harvesting is important to cases (28.5%). In none of the specimens the OA prevent inadvertent damage to the donor. The was found to run in a bony canal. In 68.6% of the from the asterion to the OA groove, thereby proximal portion of the OA is found in the occipital cases, the OMS was found to be medial to the OA localizing the proximal OA. Inadvertent damage to groove. The occipitomastoid suture (OMS) is located groove or impression while in 31.4%, it ran the proximal OA may be avoided by identifying the between the occipital bone and the mastoid portion centrally through the OA groove or impression OMS and dissecting medial to it, since in majority of the temporal bone. This study aimed to assess (Figure 1). The OMS was never found lateral to the of cases, the proximal OA will be located lateral to the relationship between the OMS and the occipital OA it groove, in order to facilitate localization of the proximal portion of OA while harvesting it for bypass Learning Objectives 1.To understand the relationship between the Figure 1 occipital groove and the occiptomastoid suture 2.To understand the potential use of occipitomastoid suture as a landmark to identify the proximal Methods segment of OA in the occipital groove Thirty-five dry skulls were assessed bilaterally (n=70) to study the bony landmarks that can be used to identify and locate the proximal segment of OA. -

Anatomical Classification of Sutural Bones
MOJ Anatomy & Physiology Mini Review Open Access Anatomical classification of sutural bones Abstract Volume 3 Issue 4 - 2017 Sutural bones are accessory bones which occur within the skull. They get a different name, Rafael Romero Reverón1,2 derivative from the suture or sutures they are in contact with or with the centre of ossification 1Department of Human Anatomy, Universidad Central de or fontanel where they originate. They are classified into true Sutural bones and false Sutural Venezuela, Venezuela bones. True Sutural bones derived from one or many points of ossification. False Sutural 2Medical doctor Specialist in Orthopedic Trauma Surgery at bones are ossification centers not connected to independent bones. Although Sutural bones Centro Médico Docente La Trinidad, Venezuela they are poorly reported while they are quiet frequent. Sutural bones are being of interest to human anatomy, neurosurgery, physical anthropology, forensic medicine, craniofacial Correspondence: Rafael Romero Reverón, Department of surgery, radiology among others. Human Anatomy, Universidad Central de Venezuela, Medical doctor Specialist in Orthopedic Trauma Surgery at Centro Keywords: sutural bones, true sutural bones, false sutural bones, wormian bones, Médico Docente La Trinidad, Venezuela, anatomical classification Email [email protected] Received: February 23, 2017 | Published: April 10, 2017 Introduction both sexes as well as in both sides of the skull. Approximately half of Sutural bones are located in the lambdoid suture and fontanel and the The human skull is composed of several bones that fuse together masto-occipital suture. The second most common site of incidence after birth additionally to the regular centre of ossification of the skull. (about 25%) is in the coronal suture.7,8 The rest occur in any remaining Sutural bones are sporadically found in the course of cranial sutures sutures and fontanels.9 Knowledge of this variation is very important and fontanels or isolated. -

Nasal Morphology and Its Correlation to Craniofacial Morphology in Lateral Cephalometric Analysis
International Journal of Environmental Research and Public Health Article Nasal Morphology and Its Correlation to Craniofacial Morphology in Lateral Cephalometric Analysis Agnieszka Jankowska 1 , Joanna Janiszewska-Olszowska 2,* and Katarzyna Grocholewicz 2 1 Private Practice “Dental Clinic Jankowscy”, 68-200 Zary,˙ Poland; [email protected] 2 Department of Interdisciplinary Dentistry, Pomeranian Medical University in Szczecin, 70-111 Szczecin, Poland; [email protected] * Correspondence: [email protected]; Tel.: +48-91-466-1690 Abstract: Nose shape, size, and inclination influence facial appearance, but few studies concern the relationship between the nasal profile and craniofacial structures. The objective of this study was to analyze association of nasal cephalometric variables with skeletal structures, age, and sex. Cephalometric and nasal analysis was performed in 386 Polish orthodontic patients (aged 9–25 years). Student t-test and Mann–Whitney test were used to compare quantitative variables and Pearson’s or Spearman’s correlation coefficients—to find correlations. Soft tissue facial convexity angle corre- lates to Holdaway ratio, ANB (A-Nasion-B), and Wits appraisal. Nasal dorsum axis, nose length, nose depth (1) and nose depth (2), nose hump, lower dorsum convexity, and columella convexity increase with age. Nasal base angle, nasolabial angle, nasomental angle, soft tissue facial convex- ity and nasal bone angle decrease with age. Nasal base angle and nasomental angle are smaller in females. Thus, a relationship exists between nasal morphology and sagittal jaw configuration. Nasal parameters significantly change with age. Sexual dimorphism characterizes nasal bone angle Citation: Jankowska, A.; and nasomental angle. Janiszewska-Olszowska, J.; Grocholewicz, K. Nasal Morphology Keywords: nose; nose profile; cephalometry; orthodontics and Its Correlation to Craniofacial Morphology in Lateral Cephalometric Analysis. -

Cleidocranial Dysplasia- a Case Report
Case Report Cleidocranial Dysplasia- A Case Report Akhilanand Chaurasia Department of Oral Medicine & Radiology, Faculty of Dental Sciences, King George Medical University, Lucknow E-mail: [email protected] ABSTRACT Cleidocranial dysplasia is a rare congenital disease. It is characterized by autosomal dominant inheritance pattern which is caused due to mutations in the Cbfa1 gene (Runx2) located on chromosome 6p21. It primarily affects bones which are formedby intra-membranous ossification and have equal sex distribution. It is also known as Marie and Sainton disease, Mutational dysostosis and cleidocranialdysostosis. The skeletal deformities of cleidocranial dysplasia are characterized by partial or complete absence of clavicles, late closure of the fontanels, presence of open skull sutures and multiple wormian bones. This rare syndrome is of utmost importance in dentistry due to presence of multiple supernumerary teeth, facial bones deformities and deranged eruption patterns. We are reporting a classical case of cleidocranial dysplasia in 20 year old patient. Keywords: Cleidocranial dysplasia, Marie and Sainton disease, Mutational dysostosis, Cleidocranialdysostosis, Autosomal dominant Access this article online mandibular symphysis are less common findings of Quick Response cleidocranial dysostosis1,10,11. Code: Website: Dental findings in cleidocranialdysostosis are www.innovativepublication.com characterized by a decreased eruptive force of both primary and permanent dentition, prolonged retention of primary teeth12 and an increase in odontogenesis DOI: 10.5958/2395-6194.2015.00009.0 leading to an excessive number of supernumerary teeth13. The clinical findings of cleidocranialdysostosis although present at birth are often either missed or INTRODUCTION diagnosed at a much later time. Cleidocranialdysostosis Cleidocranialdysostosis is a rare congenital defect may be identified by family history, excessive mobility primarily affecting bones which undergo intra- of shoulders and radiographic pathognomonic findings membranous ossification i.e. -

Study of Wormian Bones on Dry Human Skull and Its Sexual Dimorphism in the Region of Andhra Pradesh
Original Research Article Study of Wormian Bones on Dry human skull and its sexual dimorphism in the region of Andhra Pradesh Shone Vasudeo Durge Assistant Professor, Dept. of Anatomy, Fathima Institute of Medical Sciences, Ramarajupalli, Andhra Pradesh Corresponding Author: E-mail: [email protected] Abstract This study was aimed at identifying the wormian bone and their overall incidence in respect to their number and location in the region of Andhra Pradesh. Overall incidence of wormian bones was more in female (47.72%) than in male skulls (41.66%). They occurred more frequently at lambdoid suture (38%). Wormian bones along the coronal suture, Bregma and Asterion were seen only in male skulls, while intra-orbital wormian bones and wormian bones at Pterion were seen only in female skulls. This study concludes by stating that, there exists a moderate degree of sexual dimorphism among the wormian bones with respect to overall incidence, number and location. Keywords- Skull, Sexual dimorphism, Wormian bones, Lambda, Asterion. Background knowledge of WBs is important in the diagnosis of Wormian bones, also known as intra-sutural bones, these disorders (Cremin, Goodman, Spranger et al., are extra bone pieces that occur within a suture in the 1982). It was reported that their incidence is well suited cranium. These are irregular isolated bones that appear for comparative studies as an anthropological marker or in addition to the usual centers of ossification of the an indicator of population distance (Gumusburun, cranium and, although unusual, are not rare. They occur Sevim, Katkici et al., 1997). Their knowledge is of most frequently in the course of the lambdoid suture, interest to the human anatomy, physical anthropology which is more tortuous than other sutures. -

Morphological and Topographical Study of Wormian Bones in Cadaver Dry Skulls
Original article Morphological and topographical study of Wormian bones in cadaver dry skulls Murlimanju, BV.*, Prabhu, LV., Ashraf, CM., Kumar, CG., Rai, R. and Maheshwari, C. Department of Anatomy, Manipal University, Centre for Basic Sciences, Kasturba Medical College, Mangalore, India *E-mail: [email protected] Abstract Introduction: The Wormian bones are formations associated with insufficient rate of suture closure and regarded as epigenetic and hypostotic traits. It was reported that there exists racial variability among the incidence of these bones. In the present study, the aims were to find the incidence of Wormian bones in Indian skulls and to analyze them topographically. Material and methods: The study included 78 human adult dry skulls of Indian population which were obtained from the neuroanatomy laboratory of our institution. They were macroscopically observed for the incidence and topographical distribution of the Wormian bones. Results: The Wormian bones were observed in 57 skulls (73.1%) of our series. Remaining 21 skulls (26.9%) didn’t show these variant bones. They were observed at the lambdoid suture in 56.4% cases (44 skulls; 14-bilateral; 18-right side; 12-left side), at the asterion in 17.9% (14 skulls; 3-bilateral; 2-right side; 9-left side), at the pterion in 11.5% (9 skulls; 4-right side; 5-left side), at the coronal suture in 1.3% (only one skull) and at the sagittal suture in 1.3% cases (only one skull). Conclusion: The current study observed Wormian bones in 73.1% of the cases from Indian population. This incidence rate is slightly higher compared to other reports and may be due to racial variations. -

Chapter 22 TEMPORAL BONE FRACTURES
Temporal Bone Fractures Chapter 22 TEMPORAL BONE FRACTURES † CARLOS R. ESQUIVEL, MD,* AND NICHOLAS J. SCALZITTI, MD INTRODUCTION INITIAL EVALUATION FRACTURE CLASSIFICATION RADIOGRAPHIC EVALUATION MANAGEMENT OF INJURIES Facial Nerve Injury Hearing Loss Cerebrospinal Fluid Leak and Use of Antibiotic Therapy SPECIAL CONSIDERATIONS FOR WARTIME INJURIES Acute Management CASE PRESENTATIONS Case Study 22-1 Case Study 22-2 *Lieutenant Colonel (Retired), Medical Corps, US Air Force; Clinical Director, Department of Defense, Hearing Center of Excellence, Wilford Hall Ambulatory Surgical Center, 59th Medical Wing, Lackland Air Force Base, Texas 78236 †Captain, Medical Corps, US Air Force; Resident Otolaryngologist, San Antonio Military Medical Center, 3551 Roger Brooke Drive, Joint Base San Antonio, Fort Sam Houston, Texas 78234 267 Otolaryngology/Head and Neck Combat Casualty Care INTRODUCTION The conflicts in Iraq and Afghanistan have resulted age to the deeper structures of the middle and inner in large numbers of head and neck injuries to NATO ear, as well as the brain. Special arrangement of the (North Atlantic Treaty Organization) and Afghan ser- outer and middle ear is essential for efficient capture vice members. Improvised explosive devices, mortars, and transduction of sound energy to the inner ear in and suicide bombs are the weapons of choice during order for hearing to take place. This efficiency relies this conflict. The resultant injuries are high-velocity on a functional anatomical relationship of a taut tym- projectile injuries. Relatively little is known about the panic membrane connected to a mobile, intact ossicular precise incidence and prevalence of isolated closed chain. Traumatic forces that disrupt this relationship temporal bone fractures in theater. -

Morfofunctional Structure of the Skull
N.L. Svintsytska V.H. Hryn Morfofunctional structure of the skull Study guide Poltava 2016 Ministry of Public Health of Ukraine Public Institution «Central Methodological Office for Higher Medical Education of MPH of Ukraine» Higher State Educational Establishment of Ukraine «Ukranian Medical Stomatological Academy» N.L. Svintsytska, V.H. Hryn Morfofunctional structure of the skull Study guide Poltava 2016 2 LBC 28.706 UDC 611.714/716 S 24 «Recommended by the Ministry of Health of Ukraine as textbook for English- speaking students of higher educational institutions of the MPH of Ukraine» (minutes of the meeting of the Commission for the organization of training and methodical literature for the persons enrolled in higher medical (pharmaceutical) educational establishments of postgraduate education MPH of Ukraine, from 02.06.2016 №2). Letter of the MPH of Ukraine of 11.07.2016 № 08.01-30/17321 Composed by: N.L. Svintsytska, Associate Professor at the Department of Human Anatomy of Higher State Educational Establishment of Ukraine «Ukrainian Medical Stomatological Academy», PhD in Medicine, Associate Professor V.H. Hryn, Associate Professor at the Department of Human Anatomy of Higher State Educational Establishment of Ukraine «Ukrainian Medical Stomatological Academy», PhD in Medicine, Associate Professor This textbook is intended for undergraduate, postgraduate students and continuing education of health care professionals in a variety of clinical disciplines (medicine, pediatrics, dentistry) as it includes the basic concepts of human anatomy of the skull in adults and newborns. Rewiewed by: O.M. Slobodian, Head of the Department of Anatomy, Topographic Anatomy and Operative Surgery of Higher State Educational Establishment of Ukraine «Bukovinian State Medical University», Doctor of Medical Sciences, Professor M.V. -

Morphology of the Pterion in Serbian Population
Int. J. Morphol., 38(4):820-824, 2020. Morphology of the Pterion in Serbian Population Morfología del Pterion en Población Serbia Knezi Nikola1; Stojsic Dzunja Ljubica1; Adjic Ivan2; Maric Dusica1 & Pupovac Nikolina4 KNEZI, N.; STOJSIC, D. L.; ADJIC, I.; MARIC, D. & PUPOVAC, N. Morphology of the pterion in Serbian population. Int. J. Morphol., 38(4):820-824, 2020. SUMMARY: The pterion is a topographic point on the lateral aspect of the skull where frontal, sphenoid, parietal and temporal bones form the H or K shaped suture. This is an important surgical point for the lesions in anterior and middle cranial fossa. This study was performed on 50 dry skulls from Serbian adult individuals from Department of Anatomy, Faculty of Medicine in Novi Sad. The type of the pterion on both sides of each skull was determined and they are calcified in four types (sphenoparietal, frontotemporal, stellate and epipteric). The distance between the center of the pterion and defined anthropological landmarks were measured using the ImageJ software. Sphenoparietal type is predominant with 86 % in right side and 88 % in left side. In male skulls, the distance from the right pterion to the frontozygomatic suture is 39.89±3.85 mm and 39.67±4.61 mm from the left pterion to the frontozygomatic suture. In female skulls the distance is 37.38±6.38 mm on the right and 35.94±6.46 mm on the left. The shape and the localization of the pterion are important because it is an anatomical landmark and should be used in neurosurgery, traumatology and ophthalmology. -

CASE REPORT Osteopathic Manipulative Treatment to Resolve
CASE REPORT Osteopathic Manipulative Treatment to Resolve Head and Neck Pain After Tooth Extraction Patricia M. Meyer, DO, MS Sharon M. Gustowski, DO, MPH Pain is a common occurrence after tooth extraction and fter dental extraction, the majority of patients have is usually localized to the extraction site. However, clinical Apain lasting less than 1 week that can be controlled experience shows that patients may also have pain in by analgesics. The length, type, and severity of pain vary the head or neck in the weeks after this procedure. The as a result of multiple factors, such as the difficulty of the authors present a case representative of these findings. extraction procedure, the patient’s health status and atti - In the case, cranial and cervical somatic dysfunction in tude, and the patient’s sex. 1 Other pain syndromes that a patient who had undergone tooth extraction was may occur weeks after the procedure—though rare— resolved through the use of osteopathic manipulative include neuropathic pain, temporomandibular disorder, 2,3 treatment. This case emphasizes the need to include a cluster headache, 4,5 and neck and head pain caused by dental history when evaluating head and neck pain as somatic dysfunction. 6,7 Prolonged and nonresolving pain part of comprehensive osteopathic medical care. The should be investigated for such conditions as rheumatologic case can also serve as a foundation for a detailed discus - diseases, tumors, migraine headache, or myofascial pain sion regarding how to effectively incorporate osteopathic syndrome. manipulative treatment into primary care practice for The etiologic characteristics of head and neck pain patients who present with head or neck pain after tooth after dental procedures are multifactorial, depending on extraction. -
The Effects of Somatic Dysfunction on the Spinal Accessory Nerve (CN XI) with Subsequent Distal Dysfunctions by Sherman Gorbis, DO, FAAO
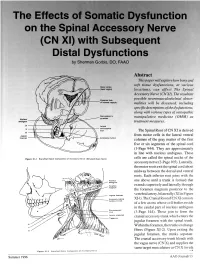
The Effects of Somatic Dysfunction on the Spinal Accessory Nerve (CN XI) with Subsequent Distal Dysfunctions by Sherman Gorbis, DO, FAAO Abstract This paper will explore how bony and soft tissue dysfunctions, at various Motor codes (head region) locations, can affect The Spinal Accessory Nerve (CN XI). The resultant possible neuromusculoskeletal abnor- Posterior limb of internal capsule malities will be discussed, including specific descriptions of the dysfunctions, along with various types of osteopathic DBOUSSFigon In pyramids manipulative medicine (OMM) as Nucleus amblguus treatment measures. IX Lateral X corticospinal tract The Spinal Root of CN XI is derived XI Jugular from motor cells in the lateral ventral foramen Accessory nucleus columns of the gray matter of the first five or six segments of the spinal cord (1-Page 944). They are approximately in line with nucleus ambiguus. These Flgure XI-I Branchtal Motot Component of Accessory Nerve (Elevated Brain Sterol cells are called the spinal nuclei of the accessory nerve (2-Page 105). Laterally, the motor roots exit the spinal cord about midway between the dorsal and ventral roots. Each inferior root joins with the one above until a trunk is formed that extends superiorly and laterally through the foramen magnum posterior to the Jugular lor•men vertebral artery, bilaterally (XI in Figure Accessory (spinal XI-1). The Cranial Root of CN XI consists nucleus CI-CS of a few axons whose cell bodies reside in the caudal part of nucleus ambiguus Sternomesiod (cull (3-Page 144). These join to form the Lent or scapulae cranial accessory trunk which enters the Trap-axles jugular foramen with the spinal trunk. -

Persistent Metopic Suture with Multiple Sutural Bones at Unusual Sites
CASE REPORT Persistent metopic suture with multiple sutural bones at unusual sites Ambade HV, Fulpatil MP, Kasote AP Ambade HV, Fulpatil MP, Kasote AP. Persistent metopic suture with multiple in a human skull at asterion, left pterion and right coronal suture apart from the sutural bones at unusual sites. Int J Anat Var. 2017;10(3):69-70. lambdoid suture. Moreover, there was a persistent metopic suture between bregma to nasion in the same skull. The metopic suture with multiple sutural bones SUMMARY spreading beyond lambdoid suture at unusual sites is not reported previously. The knowledge of such variation and combination is rare and very important Sutural bones are small irregular bones found in the sutures and fontanels of for forensic expert, radiologists, orthopedists, neurosurgeons and anthropologist the human skull. They are commonly found at lambda and lambdoid suture point of view. It is very important to know about such variation because they can followed by pterion; and rarely at other sites. They vary from person to person in mislead the diagnosis of fracture of skull bones. number and shape, hence not named. Usually, 1-3 sutural bones in one skull are present, but 8-10 sutural bones are also reported in the literature, all restricted in Key Words: Metopic suture; Sutural bones; Wormian bones; Skull; Unusual sites; the vicinity of lambdoid sutures. In the present case, 8 sutural bones were present Variations INTRODUCTION etopic suture is present in between two frontal bones during fetal Mlife and soon disappear after birth. The obliteration starts at the age of 2 years and completed at the age of 8 years from above downwards (1).