Distinct Effects of Orexin Receptor Antagonist and GABAA Agonist on Sleep and Physical/Cognitive Functions After Forced Awakening
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
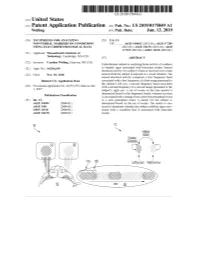
ANNNNNNNNNNNNNNNNNNNN 100A 006 Left Eye Input Right Eye Input
US 20190175049A1 ( 19) United States (12 ) Patent Application Publication (10 ) Pub. No. : US 2019 /0175049 A1 Welling ( 43 ) Pub . Date : Jun . 13 , 2019 ( 54 ) TECHNIQUES FOR ANALYZING (52 ) U . S . CI. NON -VERBAL MARKERS OF CONDITIONS CPC . .. A61B 5 /04842 (2013 . 01 ) ; A61B 5 / 7289 USING ELECTROPHYSIOLOGICAL DATA (2013 . 01) ; A61B 5 /0478 ( 2013 .01 ) ; A61B 5 /7225 ( 2013. 01 ) ; G06N 20 / 10 (2019 .01 ) (71 ) Applicant: Massachusetts Institute of Technology , Cambridge , MA (US ) ( 57 ) ABSTRACT (72 ) Inventor : Caroline Welling, Hanover, NH (US ) Embodiments related to analyzing brain activity of a subject to identify signs associated with binocular rivalry . Sensed ( 21 ) Appl. No. : 16 / 206, 639 electrical activity of a subject' s brain is received over a time period while the subject is exposed to a visual stimulus. The ( 22 ) Filed : Nov. 30 , 2018 sensed electrical activity comprises a first frequency band Related U . S . Application Data associated with a first frequency of a first image presented to the subject ' s left eye , a second frequency band associated (60 ) Provisional application No .62 / 593 , 535, filed on Dec . with a second frequency of a second image presented to the 1 , 2017 subject ' s right eye . A set of events in the time period is determined based on the frequency bands, wherein an event Publication Classification is associated with a change from a previous perceptual event (51 ) Int. Ci. to a new perceptual event. A metric for the subject is A61B 5 /0484 ( 2006 .01 ) determined based on the set of events . The metric is ana A61B 5 /00 ( 2006 .01 ) lyzed to determine whether the subject exhibits signs asso GO6N 20 / 10 (2006 .01 ) ciated with a condition that is associated with binocular A61B 5 /0478 ( 2006 .01 ) rivalry . -

Orexin Receptor Antagonists As Therapeutic Agents for Insomnia
REVIEW ARTICLE published: 25 December 2013 doi: 10.3389/fphar.2013.00163 Orexin receptor antagonists as therapeutic agents for insomnia Ana C. Equihua 1, Alberto K. De La Herrán-Arita 2 and Rene Drucker-Colin 1* 1 Neuropatología Molecular, Instituto de Fisiología Celular, Universidad Nacional Autónoma de México, Mexico City, México 2 Center for Sleep Sciences and Medicine, Stanford University, Palo Alto, CA, USA Edited by: Insomnia is a common clinical condition characterized by difficulty initiating or maintaining Christopher J. Winrow, Merck, USA sleep, or non-restorative sleep with impairment of daytime functioning. Currently, Reviewed by: treatment for insomnia involves a combination of cognitive behavioral therapy (CBTi) Matthew R. Ebben, Weill Medical and pharmacological therapy. Among pharmacological interventions, the most evidence College of Cornell University, USA Gabriella Gobbi, McGill University, exists for benzodiazepine (BZD) receptor agonist drugs (GABAA receptor), although Canada concerns persist regarding their safety and their limited efficacy. The use of these Matt Carter, University of hypnotic medications must be carefully monitored for adverse effects. Orexin (hypocretin) Washington, USA neuropeptides have been shown to regulate transitions between wakefulness and Michihiro Mieda, Kanazawa University, Japan sleep by promoting cholinergic/monoaminergic neural pathways. This has led to the *Correspondence: development of a new class of pharmacological agents that antagonize the physiological Rene Drucker-Colin, Departamento effects of orexin. The development of these agents may lead to novel therapies for de Neurociencias, Instituto de insomnia without the side effect profile of hypnotics (e.g., impaired cognition, disturbed Fisiología Celular, Universidad arousal, and motor balance difficulties). However, antagonizing a system that regulates Nacional Autónoma de México, Circuito exterior S/N, Apdo. -

Analytical Methods for Determination of Benzodiazepines. a Short Review
Cent. Eur. J. Chem. • 12(10) • 2014 • 994-1007 DOI: 10.2478/s11532-014-0551-1 Central European Journal of Chemistry Analytical methods for determination of benzodiazepines. A short review Review Article Paulina Szatkowska1, Marcin Koba1*, Piotr Kośliński1, Jacek Wandas1, Tomasz Bączek2,3 1Department of Toxicology, Faculty of Pharmacy, Collegium Medicum of Nicolaus Copernicus University, 85-089 Bydgoszcz, Poland 2Department of Pharmaceutical Chemistry, Faculty of Pharmacy, Medical University of Gdańsk, 80-416 Gdańsk, Poland 3Institute of Health Sciences, Division of Human Anatomy and Physiology, Pomeranian University of Słupsk, 76-200 Słupsk, Poland Received 16 July 2013; Accepted 6 February 2014 Abstract: Benzodiazepines (BDZs) are generally commonly used as anxiolytic and/or hypnotic drugs as a ligand of the GABAA-benzodiazepine receptor. Moreover, some of benzodiazepines are widely used as an anti-depressive and sedative drugs, and also as anti-epileptic drugs and in some cases can be useful as an adjunct treatment in refractory epilepsies or anti-alcoholic therapy. High-performance liquid chromatography (HPLC) methods, thin-layer chromatography (TLC) methods, gas chromatography (GC) methods, capillary electrophoresis (CE) methods and some of spectrophotometric and spectrofluorometric methods were developed and have been extensively applied to the analysis of number of benzodiazepine derivative drugs (BDZs) providing reliable and accurate results. The available chemical methods for the determination of BDZs in biological materials and pharmaceutical formulations are reviewed in this work. Keywords: Analytical methods • Benzodiazepines • Drugs analysis • Pharmaceutical formulations © Versita Sp. z o.o. 1. Introduction and long). For this reason, an application of these drugs became broader allowing their utility to a larger extent, Benzodiazepines have been first introduced into medical and at the same time, problems related to drug abuse practice in the 60s of the last century. -

OREXIN ANTAGONISTS BELSOMRA (Suvorexant), DAYVIGO (Lemborexant)
OREXIN ANTAGONISTS BELSOMRA (suvorexant), DAYVIGO (lemborexant) RATIONALE FOR INCLUSION IN PA PROGRAM Background Belsomra (suvorexant) and Dayvigo (lemborexant) are orexin receptor antagonists used to treat difficulty in falling and staying asleep (insomnia). Orexins are chemicals that are involved in regulating the sleep-wake cycle and play a role in keeping people awake (1-2). Regulatory Status FDA-approved indication: Orexin receptor antagonists are indicated for the treatment of insomnia, characterized by difficulties with sleep onset and/or sleep maintenance (1-2). Orexin Antagonists are contraindicated in patients with narcolepsy (1-2). Orexin Antagonists are central nervous system (CNS) depressants that can impair daytime wakefulness even when used as prescribed. Medications that treat insomnia can cause next-day drowsiness and impair driving and other activities that require alertness. Orexin Antagonists can impair driving skills and may increase the risk of falling asleep while driving. People can be impaired even when they feel fully awake. Patients should also be made aware of the potential for next-day driving impairment, because there is individual variation in sensitivity to the drug (1-2). The failure of insomnia to remit after 7 to 10 days of treatment may indicate the presence of a primary psychiatric and/or mental illness that should be evaluated (1-2). Warnings and precautions that should be discussed with the patient on Orexin Antagonist therapy include adverse reactions on abnormal thinking and behavioral changes (such as amnesia, anxiety, hallucinations and other neuropsychiatric symptoms), complex behaviors (such as sleep- driving, preparing and eating food, or making phone calls), dose-dependent increase in suicidal ideation, and sleep paralysis which is the inability to move or speak for up to several minutes during sleep-wake transitions (1-2). -

Meta-Analysis of Benzodiazepine Use in the Treatment of Insomnia
Meta-analysis of benzodiazepine use in the treatment of insomnia Review Anne M. Holbrook, Renée Crowther, Ann Lotter, Chiachen Cheng, Derek King Synthèse Abstract From the Centre for Evaluation of Medicines, Objective: To systematically review the benefits and risks associated with the use St. Joseph’s Hospital of benzodiazepines to treat insomnia in adults. and McMaster University, Data sources: MEDLINE and the Cochrane Controlled Trials Registry were Hamilton, Ont. searched for English-language articles published from 1966 to December 1998 that described randomized controlled trials of benzodiazepines for the treatment This article has been peer reviewed. of insomnia. Key words included “benzodiazepines” (exploded), “randomized controlled trial” and “insomnia.” Bibliographies of relevant articles were re- CMAJ 2000;162(2):225-33 viewed for additional studies and manufacturers of benzodiazepines were asked to submit additional randomized controlled trial reports not in the literature. ß An overview of the diagnosis and management of insomnia in clinical Study selection: Articles were considered for the meta-analysis if they were ran- practice appears on page 216. domized controlled trials involving patients with insomnia and compared a ben- zodiazepine with placebo or another active agent. Of the 89 trials originally identified, 45 met our criteria, representing a total of 2672 patients. January 25, 2000 Data extraction: Data were extracted regarding the participants, the setting, details Table of Contents of the intervention, the outcomes (including adverse effects) and the method- ologic quality of the studies. Data synthesis: The meta-analyses of sleep records indicated that, when compared with placebo, benzodiazepines decreased sleep latency by 4.2 minutes (non- significant; 95% confidence interval [CI] –0.7 to 9.2) and significantly increased total sleep duration by 61.8 minutes (95% CI 37.4 to 86.2). -

Comparative Efficacy and Acceptability of Pharmacological Treatments for Insomnia in Adults: a Systematic Review and Network Meta-Analysis (Protocol)
Cochrane Database of Systematic Reviews Comparative efficacy and acceptability of pharmacological treatments for insomnia in adults: a systematic review and network meta-analysis (Protocol) De Crescenzo F, Foti F, Ciabattini M, Del Giovane C, Watanabe N, Sañé Schepisi M, Quested DJ, Cipriani A, Barbui C, Amato L De Crescenzo F, Foti F, Ciabattini M, Del Giovane C, Watanabe N, Sañé Schepisi M, Quested DJ, Cipriani A, Barbui C, Amato L. Comparative efficacy and acceptability of pharmacological treatments for insomnia in adults: a systematic review and network meta-anal- ysis. Cochrane Database of Systematic Reviews 2016, Issue 9. Art. No.: CD012364. DOI: 10.1002/14651858.CD012364. www.cochranelibrary.com Comparative efficacy and acceptability of pharmacological treatments for insomnia in adults: a systematic review and network meta- analysis (Protocol) Copyright © 2016 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd. TABLE OF CONTENTS HEADER....................................... 1 ABSTRACT ...................................... 1 BACKGROUND .................................... 1 OBJECTIVES ..................................... 4 METHODS ...................................... 4 Figure1. ..................................... 5 ACKNOWLEDGEMENTS . 9 REFERENCES ..................................... 10 APPENDICES ..................................... 14 WHAT’SNEW..................................... 18 CONTRIBUTIONSOFAUTHORS . 18 DECLARATIONSOFINTEREST . 18 Comparative efficacy and acceptability of pharmacological treatments for -

Merck & Co., Inc
As filed with the Securities and Exchange Commission on February 25, 2021 UNITED STATES SECURITIES AND EXCHANGE COMMISSION WASHINGTON, D. C. 20549 _________________________________ FORM 10-K (MARK ONE) ☒ Annual Report Pursuant to Section 13 or 15(d) of the Securities Exchange Act of 1934 For the Fiscal Year Ended December 31, 2020 OR ☐ Transition Report Pursuant to Section 13 or 15(d) of the Securities Exchange Act of 1934 For the transition period from to Commission File No. 1-6571 _________________________________ Merck & Co., Inc. 2000 Galloping Hill Road Kenilworth New Jersey 07033 (908) 740-4000 New Jersey 22-1918501 (State or other jurisdiction of incorporation) (I.R.S Employer Identification No.) Securities Registered pursuant to Section 12(b) of the Act: Title of Each Class Trading Symbol(s) Name of Each Exchange on which Registered Common Stock ($0.50 par value) MRK New York Stock Exchange 1.125% Notes due 2021 MRK/21 New York Stock Exchange 0.500% Notes due 2024 MRK 24 New York Stock Exchange 1.875% Notes due 2026 MRK/26 New York Stock Exchange 2.500% Notes due 2034 MRK/34 New York Stock Exchange 1.375% Notes due 2036 MRK 36A New York Stock Exchange Number of shares of Common Stock ($0.50 par value) outstanding as of January 31, 2021: 2,530,315,668. Aggregate market value of Common Stock ($0.50 par value) held by non-affiliates on June 30, 2020 based on closing price on June 30, 2020: $195,461,000,000. Indicate by check mark if the registrant is a well-known seasoned issuer, as defined in Rule 405 of the Securities Act. -

Effects of Brotizolam, a New Thieno-Triazolo-Diazepine Derivative, on the Central Nervous System
In the present study, its actions on the central nervous system were investigated. Effects of Brotizolam, a New Thieno-Triazolo-Diazepine Derivative, on the Central Nervous System Kenjiro KIMISHIMA, Kyoko TANABE, Yukako KINOSHITA, Kooji TOKUYOSHI, Daisuke HOURI and Tatsuo KOBAYASHI Department of Pharmacology, Tottori University School of Medicine, Yonago 683, Japan Accepted August 24, 1984 Abstract-The effects of brotizolam, a new thieno-triazolo-diazepine derivative, on the central nervous system were analyzed in mice, rats and rabbits. Diazepam, estazolam and triazolam were used as control drugs. Brotizolam inhibited spon taneous motor activities; performances in the rotarod test, staircase test, and maximal electroshock seizure test; and pentetrazol or bemegride-induced convulsion. Moreover, catalepsy inducing action and potentiating effect on sleep elicited by pentobarbital or ethanol were observed. Following intraperitoneal or oral admin istration of brotizolam to rabbits with chronically implanted electrodes , the electro encephalographic profile in spontaneous EEG was characterized by slow waves with high amplitudes in the neocortex. The arousal responses by stimulation of the midbrain reticular formation and posterior hypothalamus were slightly inhibited, but the recruiting responses induced by stimulation of the diffuse thalamic projecting system were not inhibited, and seizure discharges induced by stimulation of the dorsal hippocampus were inhibited markedly. When motor activities and pente trazol-induced convulsions were observed as indices of tolerance for brotizolam, tolerance was not developed by repeated administration of brotizolam up to 14 days. These results suggested that brotizolam, a new thieno-triazolo-diazepine derivative, is judged to be a safer and stronger sleep inducer than diazepam and estazolam . Since the pioneering paper by Randall et et al. -

Role of the Orexin Receptor System in Stress, Sleep and Cocaine Use
Role of the orexin receptor system in stress, sleep and cocaine use NCT02785406 Version Date: 04/25/2017 IRB NUMBER: HSC-MS-16-0120 IRB APPROVAL DATE: 04/25/2017 Title: Role of the orexin receptor system in stress, sleep and cocaine use Principal Investigator: Scott D. Lane Co-Investigators: Joy M. Schmitz, Charles E. Green, Jin H. Yoon, Michael F. Weaver ABSTRACT Preclinical research has established important functions for the orexin system in mediating arousal/sleep, stress, and cue-induced reinstatement of drug taking (e.g., relapse). The role of stress/anxiety and drug cue reactivity in human drug relapse is well established, but to date, the role of the orexin system in modulating these phenomena has not been examined in humans with substance use disorders (e.g., cocaine). The goal of the present first-in-human study will be to examine the effects of an orexin antagonist (suvorexant) on interactions among stress/anxiety, sleep, and drug-cue reactivity. We will utilize a battery of highly sensitive, drug-specific, laboratory measures of drug cue reactivity (a relapse risk model), and well-established metrics of stress/anxiety and sleep. We hypothesize that antagonism of the orexin system will attenuate the link between (1) stress/anxiety and drug cue reactivity, and (2) sleep and drug cue reactivity. These results will elucidate a unique biochemical mechanism for understanding relapse, and provide a potential medication target for relapse prevention SCIENTIFIC IMPACT Given the promising preclinical data on the orexin system in modulating sleep, anxiety, and drug cue reactivity, this research project has high translational scientific value. -

S1 Table. List of Medications Analyzed in Present Study Drug
S1 Table. List of medications analyzed in present study Drug class Drugs Propofol, ketamine, etomidate, Barbiturate (1) (thiopental) Benzodiazepines (28) (midazolam, lorazepam, clonazepam, diazepam, chlordiazepoxide, oxazepam, potassium Sedatives clorazepate, bromazepam, clobazam, alprazolam, pinazepam, (32 drugs) nordazepam, fludiazepam, ethyl loflazepate, etizolam, clotiazepam, tofisopam, flurazepam, flunitrazepam, estazolam, triazolam, lormetazepam, temazepam, brotizolam, quazepam, loprazolam, zopiclone, zolpidem) Fentanyl, alfentanil, sufentanil, remifentanil, morphine, Opioid analgesics hydromorphone, nicomorphine, oxycodone, tramadol, (10 drugs) pethidine Acetaminophen, Non-steroidal anti-inflammatory drugs (36) (celecoxib, polmacoxib, etoricoxib, nimesulide, aceclofenac, acemetacin, amfenac, cinnoxicam, dexibuprofen, diclofenac, emorfazone, Non-opioid analgesics etodolac, fenoprofen, flufenamic acid, flurbiprofen, ibuprofen, (44 drugs) ketoprofen, ketorolac, lornoxicam, loxoprofen, mefenamiate, meloxicam, nabumetone, naproxen, oxaprozin, piroxicam, pranoprofen, proglumetacin, sulindac, talniflumate, tenoxicam, tiaprofenic acid, zaltoprofen, morniflumate, pelubiprofen, indomethacin), Anticonvulsants (7) (gabapentin, pregabalin, lamotrigine, levetiracetam, carbamazepine, valproic acid, lacosamide) Vecuronium, rocuronium bromide, cisatracurium, atracurium, Neuromuscular hexafluronium, pipecuronium bromide, doxacurium chloride, blocking agents fazadinium bromide, mivacurium chloride, (12 drugs) pancuronium, gallamine, succinylcholine -

Drug Information Sheet("Kusuri-No-Shiori")
Drug Information Sheet("Kusuri-no-Shiori") Internal Published: 08/2015 The information on this sheet is based on approvals granted by the Japanese regulatory authority. Approval details may vary by country. Medicines have adverse reactions (risks) as well as efficacies (benefits). It is important to minimize adverse reactions and maximize efficacy. To obtain a better therapeutic response, patients should understand their medication and cooperate with the treatment. Brand name:BROTIZOLAM TABLETS 0.25mg 「OHARA」 Active ingredient:Brotizolam Dosage form:white tablet with split line on one side, diameter: 8.0 mm, thickness: 2.3 mm Print on wrapping:ブロチゾラム錠 0.25mg「オーハラ」, ブロチゾラム, 0.25mg, OH-54, Brotizolam 0.25mg「OHARA」 Effects of this medicine This medicine intensifies the effect of GABA (γ-aminobutyric acid), a typical inhibitory transmitter of central nervous system, and suppresses hypothalamic area and cerebral limbic system which control emotion. It consequently blocks unnecessary stimulation from the autonomic nervous system and shows central nervous system depressant effect including hypnotic/sedative/anti-anxiety effect. It is usually used to treat insomnia and for anesthetic premedication. Before using this medicine, be sure to tell your doctor and pharmacist ・If you have previously experienced any allergic reactions (itch, rash, etc.) to any medicines. If you have glaucoma, myasthenia gravis or respiratory disability. ・If you are pregnant or breastfeeding. ・If you are taking any other medicinal products. (Some medicines may interact to enhance or diminish medicinal effects. Beware of over-the-counter medicines and dietary supplements as well as other prescription medicines.) Dosing schedule (How to take this medicine) ・Your dosing schedule prescribed by your doctor is<< to be written by a healthcare professional>> ・For insomnia: In general, for adults, take 1 tablet (0.25 mg of the active ingredient) at a time right before bedtime. -

EFFECTS of CHRONIC and ACUTE Y-HYDROXYBUTYRATE ADMINISTRATION on MASS and the RELEASE of GROWTH HORMONE and CORTICOSTERONE
EFFECTS OF CHRONIC AND ACUTE y-HYDROXYBUTYRATE ADMINISTRATION ON MASS AND THE RELEASE OF GROWTH HORMONE AND CORTICOSTERONE A Thesis Presented to the Faculty of the College of Science and Technology Morehead State University In Partial Fulfillment of the Requirements for the Degree Master of Science in Biology by Eric C. Goshorn October, 1998 /-t?p-1\'/ I"\s 4 ,he-a ·1 ~ ~lC\ .9~ G ls> 1 lo .JL. Accepted by the faculty of the College of Science and Technology, Morehead State University, in partial fulfillment of the requirements for the Master of Science degree. Master's Committee: /2..-lo -</'?, Date ii EFFECTS OF CHRONIC AND ACUTE y-HYDROXYBUTYRATE ADMINISTRATION ON MASS AND THE RELEASE OF GROWTH HORMONE AND CORTICOSTERONE Eric Christopher Goshorn, M.S. Morehead State University, 1998 Director of Thesis· Gamma-hydroxybutyrate (GHB) is a naturally occurring compound found both in neural (Roth and Suhr 1970) and extraneural tissue (Nelson et al. 1981 ). While the endogenous function of peripheral GHB has yet to be elucidated, experimentation has found that this compound induces anesthesia, and the release of growth hormone and prolactin from the anterior pituitary (Oyama and Takiguchi 1970; Takahara et al. 1977). This study was undertaken to determine the effect of chronic GHB injections on the weight gain of rats during early postnatal development. Acute injections were also administered to rats not previously treated with exogenous GHB to iii ascertain the mechanism of growth hormone release and to determine GHB's effect on corticosterone release. At the age of 3 days, both male and female rats from the chronic group were injected intraperitoneally with 100 mg/kg, 500 mg/kg, or 0 mg/kg of GHB.