Hair's the Question*
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Hairdressing: Fashion Updo
Hairdressing: Fashion Updo Learning outcomes Maintain effective and safe methods of working when creating an up-do hairstyle with suitable products, tools, equipment and accessories. Create a balanced, fashion up-do suitable for an individual client and demonstrate professional, creative skills. Introduction Tools required for this treatment Wedding Fashion Gown Put up/ back brushing brush The Look: Pin tail comb This look is a modern fashion look currently popular with Slim traditional cutting comb brides or bridesmaids who are looking for a romantic 4/5 long, slim sectioning clips without catches to prevent ’boho’ feel for an outdoor/ country garden / natural marking the hair theme. The look includes a lace braid. An assortment of Kirby grips to suit Adapt this style for prom looks by using different client’s hair colour accessories. Approx. 20 straight long, fine grips to fix and separate Accessories: Hair spray- firm hold/ Shine Spray Works well with flowers, ivy or comb pins accessories. Smoothing crème Oil / or serum Alternatively, use no accessories for casual day wear. Heat protector Tongs or styling irons/ straighteners If required, wadding or added hair depending on hair thickness Accessories (flowers, veil) Step 1 Part the hair diagonally as a small zig-zag approx. 9cm from the front hair line. Take into account a preferred parting (ideally side to soften the look) and the client’s head shape. Use mirror to pull down tendrils around the face, avoiding symmetry. Then create a circular section from the top of the head point to the ears. Clip out of the way. Tip: 1. -

(In)Determinable: Race in Brazil and the United States
Michigan Journal of Race and Law Volume 14 2009 Determining the (In)Determinable: Race in Brazil and the United States D. Wendy Greene Cumberland School fo Law at Samford University Follow this and additional works at: https://repository.law.umich.edu/mjrl Part of the Comparative and Foreign Law Commons, Education Law Commons, Law and Race Commons, and the Law and Society Commons Recommended Citation D. W. Greene, Determining the (In)Determinable: Race in Brazil and the United States, 14 MICH. J. RACE & L. 143 (2009). Available at: https://repository.law.umich.edu/mjrl/vol14/iss2/1 This Article is brought to you for free and open access by the Journals at University of Michigan Law School Scholarship Repository. It has been accepted for inclusion in Michigan Journal of Race and Law by an authorized editor of University of Michigan Law School Scholarship Repository. For more information, please contact [email protected]. DETERMINING THE (IN)DETERMINABLE: RACE IN BRAZIL AND THE UNITED STATES D. Wendy Greene* In recent years, the Brazilian states of Rio de Janeiro, So Paulo, and Mato Grasso du Sol have implemented race-conscious affirmative action programs in higher education. These states established admissions quotas in public universities '' for Afro-Brazilians or afrodescendentes. As a result, determining who is "Black has become a complex yet important undertaking in Brazil. Scholars and the general public alike have claimed that the determination of Blackness in Brazil is different than in the United States; determining Blackness in the United States is allegedly a simpler task than in Brazil. In Brazil it is widely acknowledged that most Brazilians are descendants of Aficans in light of the pervasive miscegenation that occurred during and after the Portuguese and Brazilian enslavement of * Assistant Professor of Law, Cumberland School of Law at Samford University. -

Hair Removal & Skin Rejuvenation Machine
Hair Removal & Skin Rejuvenation Machine IPL Hair Removal IPL laser hair removal is a very popular method of hair removal. An IPL laser uses “intense pulsed light” to gently and safely removes hair on the face, legs, back, and bikini/pubic areas. The pulses of light focus their heat on the hair follicles, destroying them without burning or damaging the skin. IPL laser hair removal is quick and veritably painless. Side effects are few, but may include redness or swelling of the treated area; this should disappear rapidly. Good candidates for IPL laser hair removal will have lighter skin and darker hair, since IPL targets pigment in the hair follicles. Many people have experienced permanent hair removal with this method; if hair does grow back, it is often sparse and finer in texture. Laser Hair removal. Laser hair removal is a gentle and effective way to permanently reduce unwanted hair from virtually any area of the body. Locate a laser hair removal clinic in your area and acquire information on the latest laser hair removal options for men and women by reading the sections below. Laser Hair Removal Procedure Laser hair removal is most effective when hair is in the growth stage. Because hair grows in cycles, laser hair removal patients typically require a series of four to six sessions spaced approximately one month apart for maximum results. www.globalclinic.co During Laser Hair Removal Treatment Typically, the areas to be treated are shaved a few days prior to the laser hair removal treatment. On the day of the procedure, an anesthetic cream may be applied, although this step is not necessary. -

Frequently Asked Questions
Frequently Asked Questions What are the requirements for license renewal? Licenses Expire CE Hours Required 16 Biennial renewals are due on October 31. (All hours are allowed through home-study) How do I complete this course and receive my certificate of completion? Online Fax Phone Mail (386) 673-3563 - Be sure (855) 769-9888 - Please have your test Use the envelope provided Go to Cosmetology. to include your credit answers, license number and credit or mail to Elite, PO Box 37, EliteCME.com and follow card information. Your card ready. There will be an additional Ormond Beach, FL 32175. the prompts. Print your certificate will be e-mailed $4.95 convenience fee added for tests Your certificate will be certificate immediately. to you. received by phone. e-mailed to you. How much will it cost? Cost of Courses Course Title CE Hours Price 16 CE Hour Update for Florida Cosmetologists 16 $21.95 Are you a Florida board approved provider? Elite is approved by the Florida Department of Business and Professional Regulation (DBPR). Our provider number is 0001553. Are my credit hours reported to the Florida board? Yes, we report your hours electronically to the Florida Department of Business and Professional Regulation (DBPR) within one business day after completion. Is my information secure? Yes! Our website is secured by Thawte, we use SSL encryption, and we never share your information with third-parties. We are also rated A+ by the National Better Business Bureau. What if I still have questions? What are your business hours? No problem, we have several options for you to choose from! Online at Cosmetology.EliteCME.com you will see our robust FAQ section that answers many of your questions, simply click FAQ in the upper right hand corner or Email us at [email protected] or call us toll free at 1-855-769-9888, Monday - Friday 9:00 am - 6:00 pm, EST. -

The Art of Dressing Hair
The art of dressing hair UV10345 Y/502/3979 Learner name: VRQ Learner number: VTCT is the specialist awarding body for the Hairdressing, Beauty Therapy, Complementary Therapy and Sport and Active Leisure sectors, with over 45 years of experience. VTCT is an awarding body regulated by national organisations including Ofqual, SQA, DCELLS and CCEA. VTCT is a registered charity investing in education and skills but also giving to good causes in the area of facial disfigurement. Statement of unit achievement By signing this statement of unit achievement you are confirming that all learning outcomes, assessment criteria and range statements have been achieved under specified conditions and that the evidence gathered is authentic. This statement of unit achievement table must be completed prior to claiming certification. Assessor IV signature Unit code Date achieved Learner signature initials (if sampled) Assessor tracking table All assessors using this Record of Assessment book must complete this table. This is required for verification purposes. Assessors Assessor number Assessor name Assessor signature initials (optional) UV10345 The art of dressing hair The aim of this unit is to develop the creative skill of styling, dressing and finishing hair. You will learn how to identify the capability of your client’s hair which will allow you to choose from a range of products, tools and equipment to complete the look. You will need to demonstrate the ability to blow dry, set, put up hair and finish your client’s hair using heated styling equipment. Part of this service is to provide your client with good aftercare advice. UV10345_v7 Level 2 Credit value 5 GLH 30 Observation(s) 4 External paper(s) 1 Photo courtesy of Wahl UK Ltd. -

Makeup-Hairstyling-2019-V1-Ballot.Pdf
2019 Primetime Emmy® Awards Ballot Outstanding Hairstyling For A Single-Camera Series A.P. Bio Melvin April 11, 2019 Synopsis Jack's war with his neighbor reaches a turning point when it threatens to ruin a date with Lynette. And when the school photographer ups his rate, Durbin takes school pictures into his own hands. Technical Description Lynette’s hair was flat-ironed straight and styled. Glenn’s hair was blow-dried and styled with pomade. Lyric’s wigs are flat-ironed straight or curled with a marcel iron; a Marie Antoinette wig was created using a ¾” marcel iron and white-color spray. Jean and Paula’s (Paula = set in pin curls) curls were created with a ¾” marcel iron and Redken Hot Sets. Aparna’s hair is blow-dried straight and ends flipped up with a metal round brush. Nancy Martinez, Department Head Hairstylist Kristine Tack, Key Hairstylist American Gods Donar The Great April 14, 2019 Synopsis Shadow and Mr. Wednesday seek out Dvalin to repair the Gungnir spear. But before the dwarf is able to etch the runes of war, he requires a powerful artifact in exchange. On the journey, Wednesday tells Shadow the story of Donar the Great, set in a 1930’s Burlesque Cabaret flashback. Technical Description Mr. Weds slicked for Cabaret and two 1930-40’s inspired styles. Mr. Nancy was finger-waved. Donar wore long and medium lace wigs and a short haircut for time cuts. Columbia wore a lace wig ironed and pin curled for movement. TechBoy wore short lace wig. Showgirls wore wigs and wig caps backstage audience men in feminine styles women in masculine styles. -

Puberty Changes in Boys
PUBERTY CHANGES IN BOYS The changes of puberty in boys include growth of testes, growth of the penis, growth of pubic hair, voice change, and height spurt. An individual boy may begin his changes at a time different from his peers. TESTES DEVELOPMENT Growth of testes is usually the first change for boys. The scrotum lengthens and becomes a darker color. These changes begin between 9 ½ and 13 ½ years of age. PENIS DEVELOPMENT Growth of the penis occurs between ages 10 and 14. PUBIC HAIR Pubic hair and underarm hair appear between the ages of 10 and 14. At first the hair is fine and thin but becomes curly and coarse over time. GROWTH SPURT Increased height and change in body shape with broadening shoulders begin between the ages of 11 and 16. The voice also deepens. During this time, a boy may notice some temporary breast enlargement. This is completely normal, very common, and is no cause for concern. It will disappear with time. FACIAL AND CHEST HAIR Facial and chest hair appear at around age 17. The thickness of the beard is quite variable and depends on genes. Some men have little or no chest hair and very light beards, while others have dense growth. The amount of hair is unrelated to masculinity. ERECTIONS / EJACULATIONS Erections occur more often during puberty; sometimes a boy will have an erection for no apparent reason – this is common and normal. Ejaculation, the release of semen from the penis, begins during puberty. Like erections, ejaculation can occur for no obvious reason, especially during sleep. -
Milady-Textbook-Chapter-19-Wigs
Wigs and 19Chapter Hair Additions Chapter Outline Why Study Wigs and Hair Additions? Human versus Synthetic Hair Wigs Hairpieces Hair Extensions Photo courtesy of East Carolina Hair Clinic. Stylist Donna Wilson. Copyright 2011 Cengage Learning. All Rights Reserved. May not be copied, scanned, or duplicated, in whole or in part. Due to electronic rights, some third party content may be suppressed from the eBook and/or eChapter(s). Editorial review has deemed that any suppressed content does not materially affect the overall learning experience. Cengage Learning reserves the right to remove additional content at any time if subsequent rights restrictions require it. Learning Objectives After completing this chapter, you will be able to: LO1 Explain the differences between human hair and synthetic hair. LO2 Describe the two basic categories of wigs. LO3 Describe several types of hairpieces and their uses. LO4 Explain several different methods of attaching hair extensions. Key terms Page number indicates where in the chapter the term is used. block fallen hair integration turned hair pg. 546 pg. 544 hairpiece (Remi hair) pg. 551 pg. 543 bonding fusion bonding pg. 556 pg. 557 machine-made wigs wefts pg. 545 pg. 544 braid-and-sew hair extensions method pg. 553 semi-hand-tied wigs wig pg. 554 pg. 545 pg. 544 hairpiece cap wigs pg. 544 toupee pg. 544 pg. 551 hand-tied wigs capless wigs (caps) (hand-knotted wigs) pg. 544 pg. 545 19 Copyright 2011 Cengage Learning. All Rights Reserved. May not be copied, scanned, or duplicated, in whole or in part. Due to electronic rights, some third party content may be suppressed from the eBook and/or eChapter(s). -

Does Materialism Predict Body Hair Removal Among Undergraduate Males and Females? Brianna Ballew Grand Valley State University, [email protected]
Grand Valley State University ScholarWorks@GVSU Honors Projects Undergraduate Research and Creative Practice 4-2016 Does Materialism Predict Body Hair Removal Among Undergraduate Males and Females? Brianna Ballew Grand Valley State University, [email protected] Follow this and additional works at: http://scholarworks.gvsu.edu/honorsprojects Part of the Arts and Humanities Commons Recommended Citation Ballew, Brianna, "Does Materialism Predict Body Hair Removal Among Undergraduate Males and Females?" (2016). Honors Projects. 576. http://scholarworks.gvsu.edu/honorsprojects/576 This Open Access is brought to you for free and open access by the Undergraduate Research and Creative Practice at ScholarWorks@GVSU. It has been accepted for inclusion in Honors Projects by an authorized administrator of ScholarWorks@GVSU. For more information, please contact [email protected]. Materialist Values and Body Hair Removal 1 Running head: Materialist Values and Body Hair Removal Does Materialism Predict Body Hair Removal Among Undergraduate Males and Females? Brianna Ballew Grand Valley State University Faculty Advisor: Donna Henderson-King Ph.D. – Psychology Department 499 Honors Senior Project April, 2016 Materialist Values and Body Hair Removal 2 Abstract Previous research indicates that materialistic women are more likely to want to alter their bodies (Henderson-King & Brooks, 2009). This study focuses specifically on the relationship between materialism and body hair removal. We collected information about the frequency of body hair removal, reasons for hair removal, and materialism (Richins & Dawson, 1992). Findings indicate that males and females do not significantly differ on materialist values. Correlational analyses reveal that for women, materialism is related to frequency of hair removal for several body sites; for men, however, materialism was related to body hair removal for only a single site. -
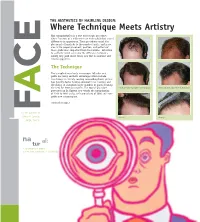
Where Technique Meets Artistry Hair Transplantation Is a True Microscopic Procedure, Where Fractions of a Millimeter Can Make Subtle but Critical
THE AESTHETICS OF HAIRLINE DESIGN: Where Technique Meets Artistry Hair transplantation is a true microscopic procedure, where fractions of a millimeter can make subtle but critical E differences in appearance. These procedures entail the placement of hundreds to thousands of grafts, and in no area is the proper placement, position, and pattern of these grafts more important than the hairline. Attention to aesthetic detail can make the difference between a merely very good result versus one that is excellent and natural appearing. C The Technique The transplanting of only microscopic follicular unit grafts has many aesthetic advantages which include: less damage to already existing surrounding hairs; greater hair density; faster healing; minimal to no scarring; and the ability to transplant larger numbers of grafts meaning the need for fewer procedures. The typical procedure Before and after a procedure of 2400 grafts Before and after a procedure of 2500 grafts performed by Dr. Epstein now entails the transplanting A of 2200 to 2400 grafts, with procedures of 3000 and more grafts now commonplace. continued on page 2 F For the patients of Jeffrey S. Epstein, Close-up Close-up M. D., F.A .C.S. na al: tur 1. As existing in nature 2. Free from pretension or artificiality WORDS FROM THE DOCTOR THE AESTHETICS OF HAIRLINE DESIGN (cont.) Since 1993, I have been fortunate to participate in the evolution The Aesthetics of the specialties of surgical hair The transplanted hairlines on this page all restoration and facial plastic demonstrate different aesthetic aspects of a natural a surgery. Few other surgical appearing hairline. -

The Relationship of Psychological Trauma with Trichotillomania and Skin Picking
Journal name: Neuropsychiatric Disease and Treatment Article Designation: Original Research Year: 2015 Volume: 11 Neuropsychiatric Disease and Treatment Dovepress Running head verso: Özten et al Running head recto: Psychological trauma with trichotillomania and skin picking open access to scientific and medical research DOI: http://dx.doi.org/10.2147/NDT.S79554 Open Access Full Text Article ORIGINAL RESEARCH The relationship of psychological trauma with trichotillomania and skin picking Eylem Özten1 Objective: Interactions between psychological, biological and environmental factors are Gökben Hızlı Sayar1 important in development of trichotillomania and skin picking. The aim of this study is to Gül Eryılmaz1 determine the relationship of traumatic life events, symptoms of post-traumatic stress disorder Gaye Kag˘an2 and dissociation in patients with diagnoses of trichotillomania and skin picking disorder. Sibel Işık3 Methods: The study included patients who was diagnosed with trichotillomania (n=23) or skin Og˘uz Karamustafalıog˘lu4 picking disorder (n=44), and healthy controls (n=37). Beck Depression Inventory, Traumatic Stress Symptoms Scale and Dissociative Experiences Scale were administered. All groups 1 Neuropsychiatry Health, Practice, checked a list of traumatic life events to determine the exposed traumatic events. and Research Center, Üsküdar University, 2Istanbul Neuropsychiatry Results: There was no statistical significance between three groups in terms of Dissociative Hospital, Üsküdar University, 3Turkish Experiences Scale -

Body Depilation Among Women and Men: the Association of Body Hair Reduction Or Removal with Body Satisfaction, Appearance Compar
University of South Florida Scholar Commons Graduate Theses and Dissertations Graduate School January 2012 Body Depilation among Women and Men: The Association of Body Hair Reduction or Removal with Body Satisfaction, Appearance Comparison, Body Image Disturbance, and Body Dysmorphic Disorder Symptomatology Michael Scott Boroughs University of South Florida, [email protected] Follow this and additional works at: http://scholarcommons.usf.edu/etd Part of the American Studies Commons, Clinical Psychology Commons, and the Sociology Commons Scholar Commons Citation Boroughs, Michael Scott, "Body Depilation among Women and Men: The Association of Body Hair Reduction or Removal with Body Satisfaction, Appearance Comparison, Body Image Disturbance, and Body Dysmorphic Disorder Symptomatology" (2012). Graduate Theses and Dissertations. http://scholarcommons.usf.edu/etd/3985 This Dissertation is brought to you for free and open access by the Graduate School at Scholar Commons. It has been accepted for inclusion in Graduate Theses and Dissertations by an authorized administrator of Scholar Commons. For more information, please contact [email protected]. Body Depilation among Women and Men: The Association of Body Hair Reduction or Removal with Body Satisfaction, Appearance Comparison, Body Image Disturbance, and Body Dysmorphic Disorder Symptomatology by Michael S. Boroughs A dissertation submitted in partial fulfillment of the requirements for the degree of Doctor of Philosophy Department of Psychology College of Arts and Sciences University of South Florida Major Professor: J. Kevin Thompson, Ph.D. Vicky Phares, Ph.D. Cynthia R. Cimino, Ph.D. Joseph A. Vandello, Ph.D. Brent J. Small, Ph.D. Date of Approval: October 12, 2010 Keywords: body image, body hair, human appearance, attractiveness, Social Comparison Theory, muscularity, masculinity, femininity Copyright © 2012, Michael S.