Vaccinating Against Monkeypox in the Democratic Republic of the Congo
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Vaccinia Belongs to a Family of Viruses That Is Closely Related to the Smallpox Virus
VACCINIA INFECTION What is it? Vaccinia belongs to a family of viruses that is closely related to the smallpox virus. Because of the similarities between the smallpox and vaccinia viruses, the vaccinia virus is used in the smallpox vaccine. When this virus is used as a vaccine, it allows our immune systems to develop immunity against smallpox. The smallpox vaccine does not actually contain smallpox virus and cannot cause smallpox. Vaccination usually prevents smallpox infection for at least ten years. The vaccinia vaccine against smallpox was used to successfully eradicate smallpox from the human population. More recently, this virus has also become of interest due to concerns about smallpox being used as an agent of bioterrorism. How is the virus spread? Vaccinia can be spread by touching the vaccination site before it has fully healed or by touching clothing or bandages that have been contaminated with the live virus during vaccination. In this manner, vaccinia can spread to other parts of the body and to other individuals. It cannot be spread through the air. What are the symptoms of vaccinia? Vaccinia virus symptoms are similar to smallpox, but milder. Vaccinia may cause rash, fever, headache and body aches. In certain individuals, such as those with weak immune systems, the symptoms can be more severe. What are the potential side effects of the vaccinia vaccine for smallpox? Normal reactions are mild and go away without any treatment.These include: Soreness and redness in the arm where the vaccine was given Slightly swollen, sore glands in the armpits Low grade fever One in approximately three people will feel badly enough to miss school, work or recreational activities Trouble sleeping Serious reactions are not very common but can occur in about 1,000 in every 1 million people who are vaccinated for the first time. -

Cidofovir Activity Against Poxvirus Infections
Viruses 2010 , 2, 2803-2830; doi:10.3390/v2122803 OPEN ACCESS viruses ISSN 1999-4915 www.mdpi.com/journal/viruses Review Cidofovir Activity against Poxvirus Infections Graciela Andrei * and Robert Snoeck Laboratory of Virology and Chemotherapy, Rega Institute for Medical Research, KULeuven, Minderboredersstraat 10, B-3000 Leuven, Belgium; E-Mail: [email protected] * Author to whom correspondence should be addressed; E-Mail: [email protected]; Tel.: +32-16-337372; Fax: +32-16-337340. Received: 10 November 2010; in revised form: 9 December 2010 / Accepted: 10 December 2010 / Published: 22 December 2010 Abstract: Cidofovir [(S)-1-(3-hydroxy-2-phosphonylmethoxypropyl)cytosine, HPMPC] is an acyclic nucleoside analog approved since 1996 for clinical use in the treatment of cytomegalovirus (CMV) retinitis in AIDS patients. Cidofovir (CDV) has broad-spectrum activity against DNA viruses, including herpes-, adeno-, polyoma-, papilloma- and poxviruses. Among poxviruses, cidofovir has shown in vitro activity against orthopox [vaccinia, variola (smallpox), cowpox, monkeypox, camelpox, ectromelia], molluscipox [molluscum contagiosum] and parapox [orf] viruses. The anti-poxvirus activity of cidofovir in vivo has been shown in different models of infection when the compound was administered either intraperitoneal, intranasal (aerosolized) or topically. In humans, cidofovir has been successfully used for the treatment of recalcitrant molluscum contagiosum virus and orf virus in immunocompromised patients. CDV remains a reference compound against poxviruses and holds potential for the therapy and short-term prophylaxis of not only orthopox- but also parapox- and molluscipoxvirus infections. Keywords: cidofovir; poxviruses; acyclic nucleoside analog 1. Introduction The antiviral activity of (S)-1-(3-hydroxy-2-phosphonylmethoxypropyl)cytosine (HPMPC, cidofovir, CDV) (Figure 1) against human cytomegalovirus (HCMV) and other DNA viruses was first Viruses 2010 , 2 2804 reported in 1986 [1]. -

(12) Patent Application Publication (10) Pub. No.: US 2012/0009150 A1 WEBER Et Al
US 2012O009 150A1 (19) United States (12) Patent Application Publication (10) Pub. No.: US 2012/0009150 A1 WEBER et al. (43) Pub. Date: Jan. 12, 2012 (54) DIARYLUREAS FORTREATINGVIRUS Publication Classification INFECTIONS (51) Int. Cl. (76) Inventors: Olaf WEBER, Wulfrath (DE); st 2. CR Bernd Riedl, Wuppertal (DE) ( .01) A63/675 (2006.01) (21) Appl. No.: 13/236,865 A6II 3/522 (2006.01) A6IP 29/00 (2006.01) (22) Filed: Sep. 20, 2011 A6II 3/662 (2006.01) A638/14 (2006.01) Related U.S. Application Data A63L/7056 (2006.01) A6IP3L/2 (2006.01) (63) Continuation of application No. 12/097.350. filed on A6II 3/44 (2006.01) Nov. 3, 2008, filed as application No. PCTAEPO6/ A6II 3/52 (2006.01) 11693 on Dec. 6, 2006. O O (52) U.S. Cl. .......... 424/85.6; 514/350; 514/171; 514/81; (30) Foreign Application Priority Data 514/263.38: 514/263.4: 514/120: 514/4.3: Dec. 15, 2005 (EP) .................................. 05O274513 424/85.7; 514/43 Dec. 15, 2005 (EP). ... O5O27452.1 Dec. 15, 2005 (EP). ... O5O27456.2 Dec. 15, 2005 (EP). ... O5O27458.8 The present invention relates to pharmaceutical compositions Dec. 15, 2005 (EP) O5O27.460.4 for treating virus infections and/or diseases caused by virus Dec. 15, 2005 (EP) O5O27462.O infections comprising at least a diary1 urea compound option Dec. 15, 2005 (EP). ... O5O27465.3 ally combined with at least one additional therapeutic agent. Dec. 15, 2005 (EP). ... O5O274.67.9 Useful combinations include e.g. BAY 43-9006 as a diaryl Dec. -
Here, There, and Everywhere: the Wide Host Range and Geographic Distribution of Zoonotic Orthopoxviruses
viruses Review Here, There, and Everywhere: The Wide Host Range and Geographic Distribution of Zoonotic Orthopoxviruses Natalia Ingrid Oliveira Silva, Jaqueline Silva de Oliveira, Erna Geessien Kroon , Giliane de Souza Trindade and Betânia Paiva Drumond * Laboratório de Vírus, Departamento de Microbiologia, Instituto de Ciências Biológicas, Universidade Federal de Minas Gerais: Belo Horizonte, Minas Gerais 31270-901, Brazil; [email protected] (N.I.O.S.); [email protected] (J.S.d.O.); [email protected] (E.G.K.); [email protected] (G.d.S.T.) * Correspondence: [email protected] Abstract: The global emergence of zoonotic viruses, including poxviruses, poses one of the greatest threats to human and animal health. Forty years after the eradication of smallpox, emerging zoonotic orthopoxviruses, such as monkeypox, cowpox, and vaccinia viruses continue to infect humans as well as wild and domestic animals. Currently, the geographical distribution of poxviruses in a broad range of hosts worldwide raises concerns regarding the possibility of outbreaks or viral dissemination to new geographical regions. Here, we review the global host ranges and current epidemiological understanding of zoonotic orthopoxviruses while focusing on orthopoxviruses with epidemic potential, including monkeypox, cowpox, and vaccinia viruses. Keywords: Orthopoxvirus; Poxviridae; zoonosis; Monkeypox virus; Cowpox virus; Vaccinia virus; host range; wild and domestic animals; emergent viruses; outbreak Citation: Silva, N.I.O.; de Oliveira, J.S.; Kroon, E.G.; Trindade, G.d.S.; Drumond, B.P. Here, There, and Everywhere: The Wide Host Range 1. Poxvirus and Emerging Diseases and Geographic Distribution of Zoonotic diseases, defined as diseases or infections that are naturally transmissible Zoonotic Orthopoxviruses. Viruses from vertebrate animals to humans, represent a significant threat to global health [1]. -
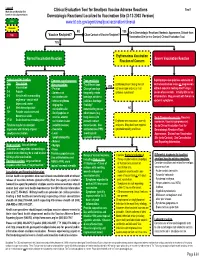
Localized to Vaccination Site (3-12-2003 Version) Low
Legend Tool 1 Morbidity and Mortality Risk Clinical Evaluation Tool for Smallpox Vaccine Adverse Reactions based on clinical presentation. Dermatologic Reactions/ Localized to Vaccination Site (3-12-2003 Version) Low www.bt.cdc.gov/agent/smallpox/vaccination/clineval Moderate NO YES Go to Dermatologic Reactions/ Nontoxic Appearance, Distant from High Close Contact of Vaccine Recipient? Vaccine Recipient? Vaccination Site (or in a Contact) Clinical Evaluation Tool. YES Erythematous Vaccination Normal Vaccination Reaction Severe Vaccination Reaction Reaction of Concern Typical reaction timeline Common signs/symptoms Tape sensitivity Rapid progressive painless extension of Day Description after vaccination Try different tape. Erythema present along lines of central vaccination lesion or progression YES 0 Vaccination - Pruritus Change bandage adhesive tape and no or mild without apparent healing after 15 days. 3-4 Papule - Soreness at frequently, rotate systemic symptoms? Lesion often necrotic. Initially little or no 5-6 Vesicle with surrounding vaccination site bandage, or take a inflammation. May present with few or no erythema - vesicle with - Intense erythema judicious bandage systemic symptoms. depressed center ringing the “holiday” 8-9 Well-formed pustule vaccination site remembering to use NO 12+ Pustule crusts over and - Small papules or other means (e.g. becomes a scab vesicles around long sleeves) to Early Progressive vaccinia (Vaccinia 17-21 Scab detaches revealing scar vaccination lesion prevent contact Erythema with induration, warmth, necrosum, Vaccinia gangrenosum) Timeline may be accelerated (satellite lesions) transmission. Use and pain. May also have regional Go to Clinical Evaluation Tool for in persons with history of prior - Headache antihistamines PRN; lymphadenopathy and fever. Dermatologic Reactions/Toxic smallpox vaccination. -
Abstract Book (PDF)
Abstract Book and Program 7th European Seminar in Virology (EuSeV) “Vaccines and antibodies against viral infections” June 14-16, 2019 Botanical Garden University of Padova 1 7th European Seminar in Virology (EuSeV) “Vaccines and antibodies against viral infections” June 14-16, 2019 Organizers: Gabriella Campadelli-Fiume, University of Bologna Dana Wolf, Hebrew University Jerusalem Michael Kann University of Gothenburg Thomas Mertens, Ulm University Medical Centre Giorgio Palù University of Padova Organizing Secretariat: Arianna Calistri, Ilaria Frasson, Michela Nandi, Marta Trevisan 2 7th. European Seminars in Virology (EuSeV) 2019 Program FRIDAY 14.06.2019 13:45-14:00 Welcome Dana Wolf, Gabriella Campadelli-Fiume, Thomas Mertens, Michael Kann Giorgio Palù Session on Ethical and technological issues about antiviral vaccine and antibodies development Chair: Giorgio Palù 14:00-14:40 Andrea Grignolio, Cognitive bases for vaccine hesitancy Medical Humanities & Bioethics, Vita-Salute San Raffaele University, Milan, Italy [email protected] 14:40-15:20 Rino Rappuoli, Reverse vaccinology 2.0 GSK, Siena, Italy [email protected] 15:20-16:00 Melvin Kohn, MSD’s Investigational Ebola Vaccine Regional Director of Medical Affairs Lead for Vaccines, MSD. [email protected] 16:00-16:30 Discussion 16:30-17:30 Selected oral presentations Francesco Santoro, Human transcriptomic response to vaccination with recombinant VSV expressing Ebola virus Glycoprotein Laboratory of Molecular Microbiology and Biotechnology (LAMMB), Dept. of Medical Biotechnologies, -

New Smallpox Vaccine Found Safer Than Existing Vaccines
APRIL 2009 • WWW.SKINANDALLERGYNEWS.COM INFECTIOUS DISEASES 37 Gardasil Prevents Warts, HPV Misunderstood, Feared HPV Infection in Males In One Border Community BY PATRICE WENDLING diagnosis of HPV as a diagnosis of BY MIRIAM E. TUCKER ACIP from the American Academy of Fam- cancer. They expressed their fears of ily Physicians. ispanic men and women liv- cancer and their belief that, once di- ATLANTA — The human papillomavirus In the randomized, double-blind, placebo- Hing on the United States–Mex- agnosed, it is “essentially a death vaccine was efficacious in preventing persis- controlled trial, three doses of Gardasil or ico border have little understanding sentence.” The women said they tent infections and genital warts caused by placebo were given at 0, 2, and 6 months. about the human papillomavirus would be reluctant to disclose their HPV strains 6, 11, 16, and 18 in a Merck-spon- Mean follow-up for this analysis was 30 and its role in the etiology of cer- HPV status to their partners be- sored study of 4,065 males aged 16-26 years. months of a planned total of 36. The study vical cancer, according to a small cause they believed they would be The findings were presented by Dr. Richard population, which came from 18 different prospective study. accused of infidelity. Men initially M. Haupt at a meeting of the Centers for Dis- countries, included 3,463 heterosexual males Not only were there very low lev- expressed anger at the possibility of ease Control and Prevention’s Advisory Com- aged 16-23 years and 602 males aged 16-26 who els of knowledge among these res- an HPV diagnosis, attributing it to mittee on Immunization Practices. -
Chapter 7. Developments in Vaccination and Control Between
CHAPTER 7 DEVELOPMENTS IN VACCINATION AND CONTROL BETWEEN 1900 AND 1966 Contents Page Introduction 277 Vaccine production and quality control before 1967 278 Production of vaccine lymph 279 Preparation of liquid vaccine 282 Preparation of dried vaccine 283 Quality control 289 Vaccination techniques before 1967 291 Vaccination site 291 Methods of vaccination 292 Age for primary vaccination 293 Interpretation of the results of vaccination 294 Complications of vaccination 296 Types of complication 299 Frequency of complications 302 Contraindications to vaccination 307 Prevention and treatment of complications 308 Reconsideration of vaccination policies in non-endemic countries 309 Complications : the overall picture 310 Programmes for vaccination and revaccination 311 Vaccination and revaccination of the general public 311 Simultaneous vaccination with several antigens 311 Vaccination of international travellers 312 INTRODUCTION The latter half of the 19th century saw the emergence of microbiology and immunology By the year 1900 vaccination was in as scientific disciplines . Because of their widespread use throughout the industrialized familiarity with vaccination, many of the countries as well as in some cities in what were pioneers in these new sciences used vaccinia then the colonies of various European virus for their studies (see Chapter 2) . In powers . Although variolation was no longer consequence, the empirical practices of Jenner practised in Europe and North America, it and his early followers were placed on a more was still widely employed in many parts of scientific basis . Vaccine production was no Africa and Asia . Smallpox persisted as an longer the province of the local physician, endemic disease in virtually every country of who had maintained the virus by arm-to-arm the world (see Chapter 8, Fig. -

(Vaccinia) Adverse Reactions
Morbidity and Mortality Weekly Report Recommendations and Reports February 3, 2006 / Vol. 55 / No. RR-1 Surveillance Guidelines for Smallpox Vaccine (vaccinia) Adverse Reactions INSIDE: Continuing Education Examination department of health and human services Centers for Disease Control and Prevention MMWR CONTENTS The MMWR series of publications is published by the Introduction......................................................................... 1 Coordinating Center for Health Information and Service, Centers for Disease Control and Prevention (CDC), U.S. Reporting Guidelines ........................................................... 2 Department of Health and Human Services, Atlanta, GA 30333. Case Definition and Classification ....................................... 2 Localized Reactions ........................................................... 3 SUGGESTED CITATION Unintentional Transfer of Vaccinia Virus ............................ 3 Centers for Disease Control and Prevention. Surveillance guidelines for smallpox vaccine (vaccinia) adverse reactions. Diffuse Dermatologic Complications ................................. 4 MMWR 2006;55(No. RR-1):[inclusive page numbers]. Progressive Vaccinia ......................................................... 6 Rare Reactions .................................................................. 6 Centers for Disease Control and Prevention Cardiac ............................................................................ 7 Julie L. Gerberding, MD, MPH Case Classification ........................................................... -

Vaccines Could Halt Third World Health Crisis Vaccines by Anita Manning 2 Human Beings Are Born with the Bare Minimum of Defenses Against Infectious Diseases
THE NATION’S NEWSPAPER PTK2003-04 Collegiate Case Study www.usatodaycollege.com Vaccines could halt Third World health crisis Vaccines By Anita Manning 2 Human beings are born with the bare minimum of defenses against infectious diseases. It is the job of a healthy immune system to strengthen itself over Vaccine use spreading time by recognizing and adapting to new threats. When a new, potentially harmful microbe enters the body, the immune system provides defense By Gary Mihoces 2 against it in the form of antibodies. More importantly, the body will remember the attacker and remember how to kill it. This secondary response provides immunity from future infection. Vaccines increase our protection by stimulating the immune system to generate antibodies against specific antigens. Large-scale vaccination of the population, called herd immunity, also provides an important defense against infectious disease. Herd immunity limits outbreaks because there are not enough susceptible people to support an epidemic. Well before the development of vaccines, humans knew that prior infection to a disease could protect a person from getting that disease again. Recorded history provides many examples of vaccination techniques being used without a full understanding of the mechanisms that allow them to work. As early as the 10th century, Chinese physicians had children inhale dried and powdered smallpox scabs. In 18th Century England, a similar procedure was used when Photo by Tim Dillon, USA TODAY small pox scabs were scratched into children's skin. Unfortunately, in some cases the procedure did backfire and kill the recipient. However, the 1% Cancer vaccine shows mortality rate was a vast improvement over the 50% mortality of smallpox. -

Boards Fodder Vaccines in Dermatology by Caroline A
boards fodder Vaccines in dermatology By Caroline A. Nelson, MD LIVE INACTIVATED/KILLED TOXOID SUBUNIT/ CONJUGATE Adenovirus Hepatitis A virus Diphtheria, tetanus, and Anthrax Cholera (oral) Influenza (injection) pertussis Haemophilus influenzae Influenza (intranasal) Japanese encephalitis Hepatitis B virus Measles, mumps, rubella Polio (injection) Human papillomavirus Polio (oral) Rabies Influenza (injection) Rotavirus Meningococcus Smallpox Pneumococcus Tuberculosis Typhoid (injection) Typhoid (oral) Zoster (Shingrix) Varicella zoster virus Yellow fever Zoster (Zostavax) VACCINE ROUTINE INDICATIONS SKIN REACTIONS/ COMPLICATIONS* NOTES† Viral Infections Hepatitis B Infants at 0-, 2-, and 6-months of Anetoderma, granuloma annulare, lichen Patients without evidence of disease or immunity virus (HBV) age and at-risk adults planus, lichen nitidus, lichen striatus, on serologic testing and with risk factors should papular acrodermatitis of childhood be offered vaccination prior to immunosuppression (Gianotti-Crosti syndrome), polyarteritis nodosa, and pseudolymphoma Human papil- Gardasil and Gardasil-9: Patients Localized lipoatrophy Vaccines contain L1 capsid protein of specific HPV lomavirus 9-26 years of age with a second types: Cervarix has 16 and 18; Gardasil has 6, 11, (HPV) dose after 6-12 months (patients 16, and 18; and Gardasil-9 has 6, 11, 16, 18, 31, 33, 15-26 years of age should receive 45, 52, and 58 a second dose after 1-2 months and a third dose after 6 months) Can be administered regardless of history of abnor- mal PAP smear -

Vaccinia (Smallpox) Vaccine
December 13, 1991 / Vol. 40 / No. RR-14 Recommendations and Reports '°0 : o r Vaccinia (Smallpox) Vaccine Recommendations of the Immunization Practices Advisory Committee (ACIP) REVERT/ALUMNI LIBRARY CREIGHTOH UNIVERSITY DEPOSITORY ITEM U.S. DEPARTMENT OF HEALTH AND HUMAN SERVICES Public Health Service , Centers for Disease Control f+ National Center for Prevention Services C Atlanta, Georgia 30333 CDCV« The MMWR series of publications is published by the Epidemiology Program Office, Centers for Disease Control, Public Health Service, U.S. Department of Health and Human Services, Atlanta, Georgia 30333. SUGGESTED CITATION Centers for Disease Control. Vaccinia (smallpox) vaccine. Recommendations of the Immunization Practices Advisory Committee (ACIP). MMWR 1991;40(RR-14) [inclusive page numbers]. Centers for Disease Control.... ..William L. Roper, M.D., M.P.H. Director The material in this report was prepared for publication by: National Center for Prevention Services .Alan R. Hinman, M.D., M.P.H. Director Division of Immunization Walter A. Orenstein, M.D. Director The production of this report as an MMWR serial publication was coordinated in: Epidemiology Program Office. Stephen B. Thacker, M.D., M.Sc. Director Richard A. Goodman, M.D., M.P.H. Editor, MMWR Series Scientific Communications Program Public Health Publications Branch. Suzanne M. Hewitt Chief Karen R. Bradfield Ava W. Navin, M.A. Project Editors Morie E. Miller Editorial Assistant Use of trade names is for identification only and does not imply endorsement by the Public Health