The Curse of the Scholarly Selective
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Vaccinia Belongs to a Family of Viruses That Is Closely Related to the Smallpox Virus
VACCINIA INFECTION What is it? Vaccinia belongs to a family of viruses that is closely related to the smallpox virus. Because of the similarities between the smallpox and vaccinia viruses, the vaccinia virus is used in the smallpox vaccine. When this virus is used as a vaccine, it allows our immune systems to develop immunity against smallpox. The smallpox vaccine does not actually contain smallpox virus and cannot cause smallpox. Vaccination usually prevents smallpox infection for at least ten years. The vaccinia vaccine against smallpox was used to successfully eradicate smallpox from the human population. More recently, this virus has also become of interest due to concerns about smallpox being used as an agent of bioterrorism. How is the virus spread? Vaccinia can be spread by touching the vaccination site before it has fully healed or by touching clothing or bandages that have been contaminated with the live virus during vaccination. In this manner, vaccinia can spread to other parts of the body and to other individuals. It cannot be spread through the air. What are the symptoms of vaccinia? Vaccinia virus symptoms are similar to smallpox, but milder. Vaccinia may cause rash, fever, headache and body aches. In certain individuals, such as those with weak immune systems, the symptoms can be more severe. What are the potential side effects of the vaccinia vaccine for smallpox? Normal reactions are mild and go away without any treatment.These include: Soreness and redness in the arm where the vaccine was given Slightly swollen, sore glands in the armpits Low grade fever One in approximately three people will feel badly enough to miss school, work or recreational activities Trouble sleeping Serious reactions are not very common but can occur in about 1,000 in every 1 million people who are vaccinated for the first time. -

Cidofovir Activity Against Poxvirus Infections
Viruses 2010 , 2, 2803-2830; doi:10.3390/v2122803 OPEN ACCESS viruses ISSN 1999-4915 www.mdpi.com/journal/viruses Review Cidofovir Activity against Poxvirus Infections Graciela Andrei * and Robert Snoeck Laboratory of Virology and Chemotherapy, Rega Institute for Medical Research, KULeuven, Minderboredersstraat 10, B-3000 Leuven, Belgium; E-Mail: [email protected] * Author to whom correspondence should be addressed; E-Mail: [email protected]; Tel.: +32-16-337372; Fax: +32-16-337340. Received: 10 November 2010; in revised form: 9 December 2010 / Accepted: 10 December 2010 / Published: 22 December 2010 Abstract: Cidofovir [(S)-1-(3-hydroxy-2-phosphonylmethoxypropyl)cytosine, HPMPC] is an acyclic nucleoside analog approved since 1996 for clinical use in the treatment of cytomegalovirus (CMV) retinitis in AIDS patients. Cidofovir (CDV) has broad-spectrum activity against DNA viruses, including herpes-, adeno-, polyoma-, papilloma- and poxviruses. Among poxviruses, cidofovir has shown in vitro activity against orthopox [vaccinia, variola (smallpox), cowpox, monkeypox, camelpox, ectromelia], molluscipox [molluscum contagiosum] and parapox [orf] viruses. The anti-poxvirus activity of cidofovir in vivo has been shown in different models of infection when the compound was administered either intraperitoneal, intranasal (aerosolized) or topically. In humans, cidofovir has been successfully used for the treatment of recalcitrant molluscum contagiosum virus and orf virus in immunocompromised patients. CDV remains a reference compound against poxviruses and holds potential for the therapy and short-term prophylaxis of not only orthopox- but also parapox- and molluscipoxvirus infections. Keywords: cidofovir; poxviruses; acyclic nucleoside analog 1. Introduction The antiviral activity of (S)-1-(3-hydroxy-2-phosphonylmethoxypropyl)cytosine (HPMPC, cidofovir, CDV) (Figure 1) against human cytomegalovirus (HCMV) and other DNA viruses was first Viruses 2010 , 2 2804 reported in 1986 [1]. -

(12) Patent Application Publication (10) Pub. No.: US 2012/0009150 A1 WEBER Et Al
US 2012O009 150A1 (19) United States (12) Patent Application Publication (10) Pub. No.: US 2012/0009150 A1 WEBER et al. (43) Pub. Date: Jan. 12, 2012 (54) DIARYLUREAS FORTREATINGVIRUS Publication Classification INFECTIONS (51) Int. Cl. (76) Inventors: Olaf WEBER, Wulfrath (DE); st 2. CR Bernd Riedl, Wuppertal (DE) ( .01) A63/675 (2006.01) (21) Appl. No.: 13/236,865 A6II 3/522 (2006.01) A6IP 29/00 (2006.01) (22) Filed: Sep. 20, 2011 A6II 3/662 (2006.01) A638/14 (2006.01) Related U.S. Application Data A63L/7056 (2006.01) A6IP3L/2 (2006.01) (63) Continuation of application No. 12/097.350. filed on A6II 3/44 (2006.01) Nov. 3, 2008, filed as application No. PCTAEPO6/ A6II 3/52 (2006.01) 11693 on Dec. 6, 2006. O O (52) U.S. Cl. .......... 424/85.6; 514/350; 514/171; 514/81; (30) Foreign Application Priority Data 514/263.38: 514/263.4: 514/120: 514/4.3: Dec. 15, 2005 (EP) .................................. 05O274513 424/85.7; 514/43 Dec. 15, 2005 (EP). ... O5O27452.1 Dec. 15, 2005 (EP). ... O5O27456.2 Dec. 15, 2005 (EP). ... O5O27458.8 The present invention relates to pharmaceutical compositions Dec. 15, 2005 (EP) O5O27.460.4 for treating virus infections and/or diseases caused by virus Dec. 15, 2005 (EP) O5O27462.O infections comprising at least a diary1 urea compound option Dec. 15, 2005 (EP). ... O5O27465.3 ally combined with at least one additional therapeutic agent. Dec. 15, 2005 (EP). ... O5O274.67.9 Useful combinations include e.g. BAY 43-9006 as a diaryl Dec. -

Draft Recommendations for Use of Smallpox Vaccine in a Pre-Event
Draft Recommendations for Use of Smallpox Vaccine in a Pre-Event Smallpox Vaccination Program: Supplemental Recommendations of the Advisory Committee on Immunization Practices (ACIP) and the Healthcare Infection Control Practices Advisory Committee (HICPAC) In June 2001, the Advisory Committee on Immunization Practices (ACIP) made recommendations for the use of smallpox (vaccinia) vaccine to protect persons working with orthopoxviruses, and to prepare for a possible bioterrorism attack and for response to an attack involving smallpox.[1] Because of the terrorist attacks in the fall of 2001, the Centers for Disease Control and Prevention (CDC) asked the ACIP to review their previous recommendations for smallpox vaccination. These supplemental recommendations update the 2001 recommendations for vaccination of persons designated to respond or care for a suspected or confirmed case of smallpox. In addition, they clarify and expand the primary strategy for control and containment of smallpox in the event of an outbreak. Recommendations for vaccination of laboratory workers who directly handle recombinant vaccinia viruses derived from non-highly attenuated vaccinia strains, or other orthopoxviruses that infect humans (e.g., monkeypox, cowpox, vaccinia, and variola) remain unchanged.[1] The following recommendations were developed after formation of a joint Working Group of the ACIP and the National Vaccine Advisory Committee (NVAC) in April 2002, joined in September 2002 by the Healthcare Infection Control Practices Advisory Committee (HICPAC), and a series of public meetings and forums to review available data on smallpox, smallpox vaccine, smallpox control strategies, and other issues related to smallpox vaccination. Smallpox Transmission and Control Smallpox is transmitted from an infected person. Patients are most infectious during the first 7 to 10 days following rash onset; transmission can occur during the prodromal period just prior to rash onset, when lesions in the mouth ulcerate, releasing virus into oral secretions. -

Painful Bubbles
Osteopathic Family Physician (2018) 29 - 31 29 CLINICAL IMAGES Painful Bubbles Craig Bober, DO & Amy Schultz, DO Lankenau Hospital Family Medicine Residency A 25 year-old female with a past medical history of well controlled eczema presented to her primary care physician with a one week his- tory of a painful “bubbles” localized to her right antecubital fossa as seen in Figure 1. She noted that the new rash appeared to form over- night, was extremely painful, and would occasionally drain a clear liquid after scratching. It did not respond to her usual over-the-counter regimen of moisturizers prompting her to be evaluated. She had subjective fevers and malaise but denied oral or genital ulcers, vaginal discharge, dysuria, ocular irritation, visual disturbances, and upper respiratory or gastrointestinal symptoms. Review of systems was oth- erwise unremarkable. She had no other known medical problems, allergies, and denied drug and alcohol use. She denied any recent travel, sick contacts, pets, or OTC medications/creams. She was sexually active in a monogamous relationship for over a year. QUESTIONS 1. What is the most likely diagnosis? A. Cellulitis B. Eczema herpeticum C. Impetigo D. Primary varicella infection 2. Which test should be performed initally? A. Blood culture B. Direct fuorescent antibody staining FIGURE 1: C. Tzanck smear D. Wound culture 3. What is the best treatment? A. Acyclovir B. Augmentin C. Doxycycline D. Varicella Zoster Immune Globulin CORRESPONDENCE: Amy Schultz, DO | [email protected] 1877-5773X/$ - see front matter. © 2018 ACOFP. All rights reserved. 30 Osteopathic Family Physician | Volume 10, No. 3 | May/June, 2018 ANSWERS 1. -

Eczema Vaccinatum in Indiana’S Public Health Nurses Play a Vital Role in Protecting, Aiding, Child Resulting from and Educating Hoosiers
Volume 10, Issue 6 June 2007 Public Health Nurse Conference Article Page 2007 No. Public Health Nurse Tom Duszynski, BS Conference 2007 1 Eczema Vaccinatum in Indiana’s public health nurses play a vital role in protecting, aiding, Child Resulting from and educating Hoosiers. The Indiana State Department of Health Transmission of (ISDH) recognizes the contribution these nurses make to public health Vaccinia from in Indiana and assists their efforts by offering continuing education Smallpox Vaccinee opportunities, such as the annual Public Health Nurse Conference. with Tertiary Spread to the Mother 3 On June 8, more than 150 public A Decade of Indiana health nurses and Sentinel Influenza Data nursing students Surveillance 8 attended the 2007 ISDH Public Training Room 13 Health Nurse Conference. This Data Reports 14 year’s conference was the most well HIV Summary 14 attended in conference history. Disease Reports 15 Several years ago, the conference began as a “training day” to provide newly hired public health nurses with general education about public health responsibilities within local health departments. The conference has consistently grown over the past several years, and new ideas and different topics have emerged based on suggestions from those who have attended. Conference planners have used participants’ input to restructure the program to meet the needs of public health nurses. This year’s conference was no exception. Deputy State Health Commissioner Mary Hill, an attorney and registered nurse, opened the conference by reminding public health nurses and nursing students of the important work they do every day for Hoosiers and how, since September 11, 2001, their roles and knowledge have changed and expanded to include the world of preparedness, again demonstrating the flexibility of public health nursing. -
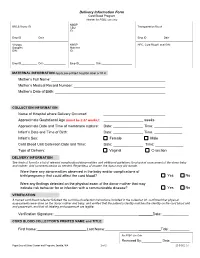
Delivery Information Form Cord Blood Program Header for PSBC Use Only NMDP BBCS Donor ID______CBU Transportation Box #______ID
Delivery Information Form Cord Blood Program Header for PSBC use only NMDP BBCS Donor ID________________________ CBU Transportation Box #____________________ ID: Emp ID___________ Date_______________ Emp ID___________ Date_______________ Virology NMDP HPC, Cord Blood Local DIN: Samples Maternal DIN: ID: Emp ID___________ Date_______________ Emp ID___________ Date_____________________ MATERNAL INFORMATION Apply pre-printed hospital label or fill in Mother’s Full Name: Mother’s Medical Record Number: Mother’s Date of Birth: COLLECTION INFORMATION Name of Hospital where Delivery Occurred: Approximate Gestational Age (must be ≥ 37 weeks): _ weeks Approximate Date and Time of membrane rupture: Date: _______________ Time: ______________ Infant’s Date and Time of Birth: Date: _______________ Time: ______________ Infant’s Sex: Female Male Cord Blood Unit Collection Date and Time: Date: _______________ Time: ______________ Type of Delivery: Vaginal C-section DELIVERY INFORMATION See back of form for a list of relevant complications/abnormalities and additional guidelines for physical assessment of the donor baby and mother. Add comments below as needed. Regardless of answer, the donor may still donate. Were there any abnormalities observed in the baby and/or complications of birth/pregnancy that could affect the cord blood? Yes No Were any findings detected on the physical exam of the donor mother that may indicate risk behavior for or infection with a communicable disease? Yes No VERIFICATION A trained cord blood collector followed the cord blood collection instructions included in the collection kit, confirmed that physical assessments were done on the donor mother and baby, and verified that the patient’s identity matches the identity on the cord blood unit and paperwork, and that all labeling and paperwork are legible. -
Here, There, and Everywhere: the Wide Host Range and Geographic Distribution of Zoonotic Orthopoxviruses
viruses Review Here, There, and Everywhere: The Wide Host Range and Geographic Distribution of Zoonotic Orthopoxviruses Natalia Ingrid Oliveira Silva, Jaqueline Silva de Oliveira, Erna Geessien Kroon , Giliane de Souza Trindade and Betânia Paiva Drumond * Laboratório de Vírus, Departamento de Microbiologia, Instituto de Ciências Biológicas, Universidade Federal de Minas Gerais: Belo Horizonte, Minas Gerais 31270-901, Brazil; [email protected] (N.I.O.S.); [email protected] (J.S.d.O.); [email protected] (E.G.K.); [email protected] (G.d.S.T.) * Correspondence: [email protected] Abstract: The global emergence of zoonotic viruses, including poxviruses, poses one of the greatest threats to human and animal health. Forty years after the eradication of smallpox, emerging zoonotic orthopoxviruses, such as monkeypox, cowpox, and vaccinia viruses continue to infect humans as well as wild and domestic animals. Currently, the geographical distribution of poxviruses in a broad range of hosts worldwide raises concerns regarding the possibility of outbreaks or viral dissemination to new geographical regions. Here, we review the global host ranges and current epidemiological understanding of zoonotic orthopoxviruses while focusing on orthopoxviruses with epidemic potential, including monkeypox, cowpox, and vaccinia viruses. Keywords: Orthopoxvirus; Poxviridae; zoonosis; Monkeypox virus; Cowpox virus; Vaccinia virus; host range; wild and domestic animals; emergent viruses; outbreak Citation: Silva, N.I.O.; de Oliveira, J.S.; Kroon, E.G.; Trindade, G.d.S.; Drumond, B.P. Here, There, and Everywhere: The Wide Host Range 1. Poxvirus and Emerging Diseases and Geographic Distribution of Zoonotic diseases, defined as diseases or infections that are naturally transmissible Zoonotic Orthopoxviruses. Viruses from vertebrate animals to humans, represent a significant threat to global health [1]. -

Disseminated Varicella Zoster Virus Infection After Vaccination with a Live Attenuated Vaccine
PRACTICE | CASES SEPSIS CPD Disseminated varicella zoster virus infection after vaccination with a live attenuated vaccine Vinita Dubey MD, Derek MacFadden MD n Cite as: CMAJ 2019 September 16;191:E1025-7. doi: 10.1503/cmaj.190270 70-year-old man presented to the emergency depart- ment with a 2-week history of rash, which started as a KEY POINTS localized eruption on his forehead and progressed to a • Live attenuated vaccines are capable of causing symptomatic vesicularA rash involving his entire body (Figure 1). Over this same vaccine-derived infection, even weeks following vaccination. period, he noted increasing shortness of breath, tiredness, pain- • Immunocompromised hosts, including those taking low-dose ful swallowing and chills. He did not report recent travel. immunosuppressive medications, are at increased risk for The patient had a past history of hypertension, coronary artery infection with live vaccine strains. disease, congestive heart failure, chronic obstructive pulmonary • Caution is required before using live attenuated vaccines in immunocompromised people; expert consultation may be disease and atrial flutter. Successful cardiac ablation had been required. performed 2 weeks before the onset of the rash. He also had rheu- • Severe and unusual adverse events following vaccination matoid arthritis, treated with methotrexate, 2.5 mg/d (6 d per should be reported to local public health authorities for week) for 3 years, hydroxychloroquine, 200 mg/d and prednisone, surveillance and investigative purposes. 10 mg/d. In the previous month, his prednisone dosage had been tapered from 10 mg/d. He was not receiving any biologic agents. On examination, the patient’s blood pressure was 110/60 mm Hg, multiple vesicular and crusted lesions, disseminated varicella heart rate 86 beats/min and temperature 36.8°C. -
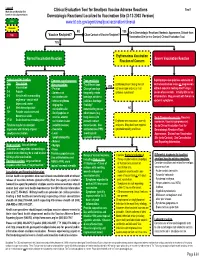
Localized to Vaccination Site (3-12-2003 Version) Low
Legend Tool 1 Morbidity and Mortality Risk Clinical Evaluation Tool for Smallpox Vaccine Adverse Reactions based on clinical presentation. Dermatologic Reactions/ Localized to Vaccination Site (3-12-2003 Version) Low www.bt.cdc.gov/agent/smallpox/vaccination/clineval Moderate NO YES Go to Dermatologic Reactions/ Nontoxic Appearance, Distant from High Close Contact of Vaccine Recipient? Vaccine Recipient? Vaccination Site (or in a Contact) Clinical Evaluation Tool. YES Erythematous Vaccination Normal Vaccination Reaction Severe Vaccination Reaction Reaction of Concern Typical reaction timeline Common signs/symptoms Tape sensitivity Rapid progressive painless extension of Day Description after vaccination Try different tape. Erythema present along lines of central vaccination lesion or progression YES 0 Vaccination - Pruritus Change bandage adhesive tape and no or mild without apparent healing after 15 days. 3-4 Papule - Soreness at frequently, rotate systemic symptoms? Lesion often necrotic. Initially little or no 5-6 Vesicle with surrounding vaccination site bandage, or take a inflammation. May present with few or no erythema - vesicle with - Intense erythema judicious bandage systemic symptoms. depressed center ringing the “holiday” 8-9 Well-formed pustule vaccination site remembering to use NO 12+ Pustule crusts over and - Small papules or other means (e.g. becomes a scab vesicles around long sleeves) to Early Progressive vaccinia (Vaccinia 17-21 Scab detaches revealing scar vaccination lesion prevent contact Erythema with induration, warmth, necrosum, Vaccinia gangrenosum) Timeline may be accelerated (satellite lesions) transmission. Use and pain. May also have regional Go to Clinical Evaluation Tool for in persons with history of prior - Headache antihistamines PRN; lymphadenopathy and fever. Dermatologic Reactions/Toxic smallpox vaccination. -
Abstract Book (PDF)
Abstract Book and Program 7th European Seminar in Virology (EuSeV) “Vaccines and antibodies against viral infections” June 14-16, 2019 Botanical Garden University of Padova 1 7th European Seminar in Virology (EuSeV) “Vaccines and antibodies against viral infections” June 14-16, 2019 Organizers: Gabriella Campadelli-Fiume, University of Bologna Dana Wolf, Hebrew University Jerusalem Michael Kann University of Gothenburg Thomas Mertens, Ulm University Medical Centre Giorgio Palù University of Padova Organizing Secretariat: Arianna Calistri, Ilaria Frasson, Michela Nandi, Marta Trevisan 2 7th. European Seminars in Virology (EuSeV) 2019 Program FRIDAY 14.06.2019 13:45-14:00 Welcome Dana Wolf, Gabriella Campadelli-Fiume, Thomas Mertens, Michael Kann Giorgio Palù Session on Ethical and technological issues about antiviral vaccine and antibodies development Chair: Giorgio Palù 14:00-14:40 Andrea Grignolio, Cognitive bases for vaccine hesitancy Medical Humanities & Bioethics, Vita-Salute San Raffaele University, Milan, Italy [email protected] 14:40-15:20 Rino Rappuoli, Reverse vaccinology 2.0 GSK, Siena, Italy [email protected] 15:20-16:00 Melvin Kohn, MSD’s Investigational Ebola Vaccine Regional Director of Medical Affairs Lead for Vaccines, MSD. [email protected] 16:00-16:30 Discussion 16:30-17:30 Selected oral presentations Francesco Santoro, Human transcriptomic response to vaccination with recombinant VSV expressing Ebola virus Glycoprotein Laboratory of Molecular Microbiology and Biotechnology (LAMMB), Dept. of Medical Biotechnologies, -

Skin Conditions That Mean You Should Not Get Smallpox Vaccine
SMALLPOX VACCINE INFORMATION STATEMENT (VIS) SUPPLEMENT C Skin Conditions That Mean You Should Not Get Smallpox Vaccine The smallpox vaccine is made from a live virus related to smallpox called vaccinia (not smallpox virus). The vaccine stimulates the immune system to react against the vaccinia virus, and develop immunity to it. Immunity to vaccinia also provides immunity to smallpox. For most people, live virus vaccines are safe and effective. However, people with certain skin conditions are more likely to have rare and serious reactions to the smallpox vaccine, including bad skin rashes (eczema vaccinatum).This results when virus from the vaccine site gets into broken skin and causes a rash in that area. While most people recover from this rash with treatment, it can be quite severe, sometimes leading to scarring or even death. SKIN CONDITIONS THAT MEAN YOU SHOULD NOT BE VACCINATED: • Individuals who have ever been diagnosed with eczema or atopic dermatitis, (conditions involving repeated episodes of red, itchy or inflamed skin) even if the condition is mild, not presently active, or if you had it only as a child, should not get the vaccine. • Individuals with Darier’s disease should not get the vaccine. • Individuals in close contact with someone who has ever been diagnosed with eczema or atopic dermatitis, even if the condition is mild, not presently active, or if they had it only as a child, should not get the vaccine because of the risk it poses to that close contact. (Close contacts include anyone living in your household and anyone you have close physical contact with such as a sexual partner.) SKIN CONDITIONS THAT MEAN YOU SHOULD WAIT BEFORE BEING VACCINATED: • Individuals with breaks in their skin should not be vaccinated until the skin is fully healed.