Hematuria As First Sign of Presentation in Urolithiasis
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Ideal Conditions for Urine Sample Handling, and Potential in Vitro Artifacts Associated with Urine Storage
Urinalysis Made Easy: The Complete Urinalysis with Images from a Fully Automated Analyzer A. Rick Alleman, DVM, PhD, DABVP, DACVP Lighthouse Veterinary Consultants, LLC Gainesville, FL Ideal conditions for urine sample handling, and potential in vitro artifacts associated with urine storage 1) Potential artifacts associated with refrigeration: a) In vitro crystal formation (especially, calcium oxalate dihydrate) that increases with the duration of storage i) When clinically significant crystalluria is suspected, it is best to confirm the finding with a freshly collected urine sample that has not been refrigerated and which is analyzed within 60 minutes of collection b) A cold urine sample may inhibit enzymatic reactions in the dipstick (e.g. glucose), leading to falsely decreased results. c) The specific gravity of cold urine may be falsely increased, because cold urine is denser than room temperature urine. 2) Potential artifacts associated with prolonged storage at room temperature, and their effects: a) Bacterial overgrowth can cause: i) Increased urine turbidity ii) Altered pH (1) Increased pH, if urease-producing bacteria are present (2) Decreased pH, if bacteria use glucose to form acidic metabolites iii) Decreased concentration of chemicals that may be metabolized by bacteria (e.g. glucose, ketones) iv) Increased number of bacteria in urine sediment v) Altered urine culture results b) Increased urine pH, which may occur due to loss of carbon dioxide or bacterial overgrowth, can cause: i) False positive dipstick protein reaction ii) Degeneration of cells and casts iii) Alter the type and amount of crystals present 3) Other potential artifacts: a) Evaporative loss of volatile substances (e.g. -

Interpretation of Canine and Feline Urinalysis
$50. 00 Interpretation of Canine and Feline Urinalysis Dennis J. Chew, DVM Stephen P. DiBartola, DVM Clinical Handbook Series Interpretation of Canine and Feline Urinalysis Dennis J. Chew, DVM Stephen P. DiBartola, DVM Clinical Handbook Series Preface Urine is that golden body fluid that has the potential to reveal the answers to many of the body’s mysteries. As Thomas McCrae (1870-1935) said, “More is missed by not looking than not knowing.” And so, the authors would like to dedicate this handbook to three pioneers of veterinary nephrology and urology who emphasized the importance of “looking,” that is, the importance of conducting routine urinalysis in the diagnosis and treatment of diseases of dogs and cats. To Dr. Carl A. Osborne , for his tireless campaign to convince veterinarians of the importance of routine urinalysis; to Dr. Richard C. Scott , for his emphasis on evaluation of fresh urine sediments; and to Dr. Gerald V. Ling for his advancement of the technique of cystocentesis. Published by The Gloyd Group, Inc. Wilmington, Delaware © 2004 by Nestlé Purina PetCare Company. All rights reserved. Printed in the United States of America. Nestlé Purina PetCare Company: Checkerboard Square, Saint Louis, Missouri, 63188 First printing, 1998. Laboratory slides reproduced by permission of Dennis J. Chew, DVM and Stephen P. DiBartola, DVM. This book is protected by copyright. ISBN 0-9678005-2-8 Table of Contents Introduction ............................................1 Part I Chapter 1 Sample Collection ...............................................5 -

Complete Urinalysis Panel
COMPLETE URINALYSIS PANEL INTERPRETATION GUIDE Scroll down or click on the following parameters to quickly access content A Complete Urinalysis is threefold: Physical exam Color Clarity - Turbidity Urine specific gravity Chemical exam pH PRO (protein) GLU (glucose) KET (ketones) UBG (urobilinogen) BIL (bilirubin) Blood LEU Sediment exam (see urine sediment guide) Cells, bacteria, casts, crystals and miscellaneous elements Urine Clarity Description In most animals, normal urine is clear to slightly cloudy. In horses, normal urine is cloudy due to the presence of calcium carbonate crystals and mucus. Values Below Reference Range Common Causes In an animal that typically shows cloudy urine, a clear urine would suggest absence of crystalluria. Values Above Reference Range Common Causes Excessively cloudy urine can be the result of high numbers of crystals, leukocytes, erythrocytes, bacteria, mucus, casts, lipids, or possibly sperm. Other Laboratory Tests Microscopic examination of the urine sediment is advised. References Barsanti JA, Lees GE, Willard MD, Green RA. Urinary disorders. In Small Animal Clinical Diagnosis by Laboratory Methods. Willard MD, Tvedten H, Turnwald GH, eds. Philadelphia, Pa: WB Saunders Company; 1999. DiBartola SP. Clinical approach and laboratory evaluation of renal disease. In Textbook of Veterinary Internal Medicine. Ettinger SJ, Feldman EC, eds. Philadelphia, Pa: WB Saunders Company; 1995. Duncan JR, Prasse KW, Mahaffey EA. Veterinary Laboratory Medicine. Ames, Iowa: Iowa State University Press; 1994. Urine Specific Gravity Description Specific gravity is a reflection of solute concentration. It should be determined by refractometry as dipsticks are inaccurate. Assuming normal hydration status and no treatments that alter water resorption by the kidneys, expected specific gravity results are: o Dogs: 1.015–1.045 o Cats: 1.035–1.060 o Horses: 1.020–1.050 The amount of other substances in urine should be interpreted in consideration of the specific gravity. -
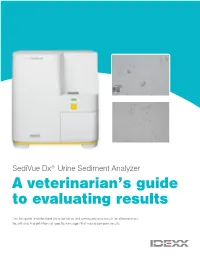
A Veterinarian's Guide to Evaluating Results
SediVue Dx® Urine Sediment Analyzer A veterinarian’s guide to evaluating results Use this guide to understand the quantitative and semiquantitative results for all parameters. You will also find definitions of specific messages that may accompany results. Element type: Blood cells Parameter Image tag Results Red blood cells None detected <1/HPF RBC (RBCs) The element has not Some rare features have Quantitative been detected or been found in the sample; numerical >50/HPF there are not enough however, the quantity result/HPF White blood cells recognizable features is below the clinical WBC (WBCs) to classify. reporting threshold. Red blood cells White blood cells Element type: Bacteria Parameter Image tag Results None detected Suspect presence Present Rods The element has not been Some recognizable features There is high confidence detected or there are not of an element (cocci, rods, that bacteria are present in N/A* enough recognizable casts) are present; however, the the sample. features to classify. quantity and detail is insufficient to report as “present.” Cocci *To avoid blocking your visual interpretation, the analyzer classifies and counts all bacteria without tagging them. NOTE: Bacteria results may be confounded by other debris and artifacts in the sample (e.g., sperm, crystalline debris). Rods Cocci Element type: Epithelial cells Parameter Image tag Results <1/HPF None detected Squamous sqEPI Some rare features The element has not have been found in been detected or the sample; however, 1–2/HPF 3–5/HPF 6–10/HPF >10/HPF there are not enough the quantity is below Nonsquamous nsEPI recognizable features the clinical reporting to classify. -

Exercise-Induced Acute Renal Failure Associated with Ibuprofen, Hydrochiorothiazide, and Triamterene1’2
EDITORIAL COMMITTEE Tomas Berl, Editor William Henrich Mark Paller Fred Silva Denver, CO Toledo, OH Minneapolis, MN Oklahoma City, OK THE NEPHROLOGY TRAINING PROGRAM AT BROOKE ARMY MEDICAL CENTER The Army Medical Department established the Nephrology Training Program at Brooke Army Medical Center, Fort Sam Houston, TX, in 1972. The program is affiliated with the Nephrology, Pathology. and Diabetes Divisions at the University of Texas Health Science Center at San Antonio and the Nephrology. Pediatric Nephrology. and Organ Transplantation Divisions at the Wilford Hall Air Force Medical Center, Lackland Air Force Base. TX. Rotations at the three institutions give fellows a broad exposure to basic and clinical nephrology. This includes an array of clinical and research conferences. patient activities, basic and clinical research, and renal biopsy interpretation. The program, designed to train Army nephrologists. emphasizes readiness for forward deployment with the REDY hemodialysis machine. The first-year fellows train in clinical nephrology. They are closely guided by senior faculty and participate actively in hemodialysis, peritoneal dialysis, continuous arteriovenous therapies. renal biopsy, and surgical and medical nephrology consultation services. They conduct outpatient nephrology clinics for the 2 yr of training. giving them broad exposure to hypertension and general nephrologic disorders. Fellows participate actively in the renal transplant program supported by the South Texas Organ Bank. During the second year. they rotate on the pediatric nephrology and organ transplantation services. They spend half of the second year conducting basic or clinical research at the University of Texas Health Science Center at San Antonio. The University of Texas research divisions have strong interests in diabetic nephropathy. -

THE URINE SEDIMENT: an Historical Perspective
The particles of the urinary sediment and their clinical meaning Cecilia Bellincioni and Giovanni B. Fogazzi Clinical and Research Laboratory on Urinary Sediment U.O. di Nefrologia Fondazione IRCCS Ca’ Granda Ospedale Maggiore Policlinico Milano, Italy THE PARTICLES OF THE URINARY SEDIMENT • Cells • Lipids • Casts • Crystals • Microorganisms • Contaminants Cells TYPE SUBTYPE 1. ERYTHROCYTES Isomorphic Dysmorphic 2. LEUKOCYTES Neutrophil Eosinophil a. FROM BLOOD Lymphocyte 3. MACROPHAGES Granular Vacuolar Homogeneous Phagocytic 1. RENAL TUBULAR CELLS Proximal Distal b. EPITHELIAL 2. TRANSITIONAL CELLS Superficial Deep 3. SQUAMOUS CELLS Superficial Deep a. CELLS FROM BLOOD 1. Erithrocytes 2. Leukocytes 3. Macrophages Erythrocytes Appearance • Small cells, with a diameter ranging from 4 to 10 µm • From perfectly round cells to very modified shapes Clinical meaning • Bleeding from the kidney • Bleeding from the excretory urinary tract • Genital contamination, especially in women Isomorphic red blood cells Dysmorphic red blood cells Erythrocyte morphology (isomorphic and dysmorphic) See presentation by Dr A. Skoberne: “Estimating erythroctye shape-dysmorphism” a. CELLS FROM BLOOD 1. Erithrocytes 2. Leukocytes 3. Macrophages Leukocytes 3 types: 1.Polymorphonuclear 2.Lymphocytes 3.Eosinophils 1.Polymorphonuclear Source Any segment of the urinary tract (without forgetting genital contamination) Appearance Round granular cells Diameter 7.0 -15.0 μm Lobulated nucleus Clinical meaning Inflammation of whatever cause including immunological disorders (eg, glomerular diseases) POLYMORPHONUCLEAR LEUKOCYTES 2.Lymphocytes Stains and cythological techniques needed Appearance small round cell, with big round nucleus and a thin cytoplasm Clinical meaning - they were considered an early marker of acute cellular rejection of renal allograft. Today, very rarely used in clinical practice - typical finding in chyluria 3.Eosinophils See presentation by Dr G.B. -

Reticulocytes
Reticulocytes Differentials Description: Reticulocytes are immature red blood cells that do not have a nucleus. Their presence in circulation is used to differentiate regenerative from nonregenerative anaemia. Reticulocytosis in the absence of anaemia can be an indication of significant underlying disease accompanied by RBC loss or destruction with an adequate regenerative response (compensated anaemia). Reticulocytes should be evaluated along with the reticulocyte haemoglobin (RETIC-HGB) for early detection of blood loss and inflammatory conditions prior to the development of anaemia. Increased Reticulocytes Regenerative anaemia Blood loss Haemorrhage Parasitism Immune-mediated haemolysis Primary (idiopathic) immune-mediated hemolytic anaemia (IMHA) Secondary IMHA Infection Neoplasia Systemic immune-mediated disease Drugs/vaccines Increased red blood cell destruction (non-immune) Heinz body anaemia Toxins Drugs Dietary Mechanical fragmentation (microangiopathic) Vasculitis Intravascular coagulation, both disseminated and local Haemangiosarcoma Heartworm infection Metabolic Hereditary Envenomation Reticulocytosis in the absence of anaemia Physiologic reticulocytosis - splenic contraction Excitement Exercise Drugs: epinephrine Compensated anaemia Blood loss Haemolysis Absolute erythrocytosis Endocrine Secondary polycythaemia Polycythaemia vera Next Steps and Related Findings for Increased Reticulocytes Regenerative Anaemia: Blood loss CBC: Decreased RBC, haematocrit, MCHC, MCH Increased MCV and RDW Generated by VetConnect® PLUS Reticulocytes -
Appendix I: Reference Intervals
Appendix I: Reference Intervals AMIN Y. BARAKAT The following reference intervals are guidelines usually needed in the diagnosis and management of renal disease. Values may vary according to the methodology used. Laboratory values are given in conventional and international units. A few references have been used in the formu lation of this table (1-5); values from other sources have been referenced separately. The prefixes for units are the standard ones approved by the Conference Generale des Poids et Mesures, 1964, the International Union of Pure and Applied Chemistry and the International Federation of Clin ical Chemistry. Few other abbreviations are used: B, blood; Ca, calcium; d, day; EDT A, ethylenediaminetetraacetate, edetic acid; f, female; hr, hour; m, male; min, minute; mo, month; RBC, red blood cell; P, plasma; S, serum; U, urine; wk, week; yr, year. Conventional International Test Specimen units units g/dl giL Albumin S Premature 3.0-4.2 30-42 NB 3.6-5.4 36-54 Infant 4.0-5.0 40-50 Thereafter 3.5-5.0 35-50 U Look under urine protein ng/dl nmoljL Aldosterone P (heparin, EDT A) Newborn: 5-60 0.14-1.7 S I wk-I yr: 1-160 0.03-4.4 1-3 yr: 5-60 0.14-1.7 3-5 yr: <5-80 <0.14-2.2 5-7 yr: <5-50 <0.14-1.4 7-11 yr: 5-70 0.14-1.9 II-IS yr: <5-50 <0.14-1.4 414 Amin Y. Barakat Conventional International Test Specimen units units ngJdl nmol/L Adult: Average sodium diet Supine: 3-10 0.08-0.3 Upright F: 5-30 0.14-0.8 M: 6-22 0.17-0.61 2-3 X higher during pregnancy Adrenal vein: 200-800 ngJdl 5.5-22 Low sodium diet: increases 2-5 fold Florinef -

A Contribution to the Study of Crystalluria: Significance in The
Journal of Advances in VetBio Science and Techniques J AdvVetBioSci Tech, 2020, 5(2), 81-89 A contribution to the study of crystalluria: significance in ReviewArticle the diagnosis of metabolic and renal diseases Muhamed KATICA1a Nasreldin Hassan AHMED2b Nedžad GRADAŠČEVIĆ3c Alen SALKIĆ4d ABSTRACT 5e The study of crystalluria is of great importance for the detection of substances of Emina DERVIŠEVIĆ endogenous or exogenous origin that are present inthe urine, to a greater or lesser 1 extent. Urinary sediment crystals can provide valuable answers for the assessment of Department of pathological physiology, Veterinary faculty, therapeutic efficacy, as well as congenital and/or acquired pathophysiological University of Sarajevo, Bosnia conditions. The nature of the observed crystals informs the clinician of the and Herzegovina, biochemical irregularity of the urine. 2Emergency medicine clinic, Crystalluria is of clinical significance only if it has been studied under good test University Clinical center conditions (sample selection, time and storage conditions). Crystalluria interpretations Sarajevo, University of Sarajevo, are performed on the basis of the urinary pH determined with statistically significant Bosnia and Herzegovina, reliability. When studying crystalluria by light microscopy, it is necessary to provide 3Department of Radiobiology light polarization or bidirectional illuminationin order to reduce the risk of diagnostic with Radiation Hygiene, error. Biophysics & Environmental Protection, Veterinary Faculty, Keywords:Urine -

Urinary Tract Disorders in Cattle
Urinary Tract Disorders in Cattle Thomas J. Divers, D. V.M New Bolton Center Kennett Square, PA Acute Renal Failure in Cattle a dehydrated animal (less than 1.022), and microscopic hematuria is usually present. Acute Tubular Necrosis Acute tubular necrosis is the most common patho Epidemiology: Acorn or oak bud poisoning is the most logic cause of acute renal failure (ARF) in cattle. This frequent in the autumn and spring. It often occurs in the results from renal ischemia or nephrotoxins. Renal autumn in association with sprouted acorns and the ischemia occurs most frequently in cattle with acute severe weaning of calves in a cow/calf operation onto a pasture of mastitis, septic metritis, abomasal torsion, salmonella, or sprouting acorns. Oak bud poisoning occurs in the spring other severe septic processes. The most common toxins and may be associated with late winter snows covering causing acute tubular necrosis in cattle are: other available grazing material. Aminoglycoside nephrotoxicity is most frequent in Quercus spp. (oak) dehydrated patients. Oxytetracycline nephrotoxicity is Halogeton glomerultos usually associated with overdosing of the drug, although it Sarcobatus vermiculatus (greasewood) may occur at normal doses in septic cattle. Oxalis spp. (soursob) Anaranthus spp. (pigwood) Treatment: Treatment is aimed at restoring intravascular Kochia spp. fluid volume by the administration of intravenous fluids Rumex (sorrel, dock) containing sodium chloride and calcium and potassium Chenopodium album (lambs quarter) when needed. The animal should be removed from the Rheum Rhaporticum (rhubarb) source of the toxin. Most cattle with acute tubular Salsola pestfiter (Russian thistle) nephrosis are polyuric, and if the disease process has not Lantana camara be present for several days, the prognosis is usually good if Isotropis the predisposing cause can be corrected. -
“All Things Are Poison,” So What Should We Test For? Evaluation of Poisoning and Drug Overdose
“All things are poison,” so what should we test for? Evaluation of Poisoning and Drug Overdose Kara Lynch, PhD, DABCC [email protected] University of California San Francisco San Francisco, CA Learning Objectives • Understand the laboratories role in the diagnosis and treatment of the overdosed patient • Review the pathophysiology of toxic exposures • Identify the common toxidromes and causative agents • Calculate the osmolar gap and anion gap • Be able to recognize drug overdoses Paraclesus – “father of toxicology” • “All things are poison, and nothing is without poison; only the dose permits something not to be poisonous.” • “The dose makes the poison.” • substances considered toxic are harmless in small doses, and an ordinarily harmless substance can be deadly if over-consumed Paraclesus, 1490 - 1541 Definition of “Poisoning” • A poisoning occurs when a person’s exposure to a natural or manmade substance has an undesirable effect - CDC • Poisonings can be classified as: – Self-harm or suicide – Assault or homicide – Unintentional or accidental, when no harm was intended – includes overdoses resulting from drug misuse, drug abuse or taking too much of a drug for medical reasons Monitoring Poisonings • AAPCC – American Association of Poison Control Centers – – National poison data system (NPDS) annual report • DAWN – Drug Abuse Warning Network • SAMHSA World Drug Report – Substance Abuse and Mental Health Services Administration • CDC – Center for Disease Control – National Vital Statistics System (NVSS) Poisoning / Overdose Trends -

Influence of Diet on Urinary Ph, Urine and Serum Biochemical Variables, and Blood-Ionized Calcium Concentrations in Healthy Dogs*
H. K. Gleaton, J. W. Bartges, and D. P. Laflamme Influence of Diet on Urinary pH, Urine and Serum Biochemical Variables, and Blood-Ionized Calcium Concentrations in Healthy Dogs* Heather K. Gleaton, DVMa Joseph W. Bartges, DVM, PhDb Dottie P. Laflamme, DVM, MS, PhDc aHolly Tree Animal Hospital 1332 South Highway 14 Simpsonville, SC 29681 bDepartment of Small Animal Clinical Sciences College of Veterinary Medicine The University of Tennessee Box 1071 Knoxville, TN 37901-1071 cThe Ralston Purina Company Checkerboard Square St. Louis, MO 63164 I ABSTRACT to aid in management of fiber-responsive dis- Urolithiasis is a common cause of lower uri- eases (Diet B; CNM Canine DCO [dry], Ral- nary tract disease in dogs. Diet influences urine ston Purina Co, St. Louis, MO); a diet formu- composition, and dietary change is often in- lated to aid in management of chronic renal corporated into medical management of failure (Diet C; CNM Canine NF [dry], Ral- uroliths. The purpose of this study was to de- ston Purina Co, St. Louis, MO); and a diet de- termine the influence of four diets on urine pH signed to aid in prevention of struvite urolithi- in healthy dogs. Sixteen adult dogs of various asis (Diet D; Prescription Diet Canine c/d breeds, ages, and weights were fed four diets in [dry], Hill’s Pet Nutrition Inc, Topeka, KS). Latin Square design: a diet formulated for Diets were fed for 21 days. On day 21, blood adult dogs at maintenance (Diet A; ProPlan and urine samples were collected before feed- Canine Chicken and Rice Adult [dry], Ralston ing one-half of daily caloric requirements, and Purina Co, St.