WHO Expert Committee on Drug Dependence Thirty-Eighth Report
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

International Collaborative Exercises (Ice)
INTERNATIONAL QUALITY ASSURANCE PROGRAMME (IQAP) INTERNATIONAL COLLABORATIVE EXERCISES (ICE) Summary Report BIOLOGICAL SPECIMENS 2013/2 INTERNATIONAL QUALITY ASSURANCE PROGRAMME (IQAP) INTERNATIONAL COLLABORATIVE EXERCISES (ICE) Table of contents Introduction Page 3 Comments from the International Panel of Forensic Experts Page 3 Codes and Abbreviations Page 4 Sample 1 Analysis Page 5 Identified substances Page 5 Statement of findings Page 6 Identification methods Page 10 Summary Page 12 Z-Scores Page 13 Sample 2 Analysis Page 15 Identified substances Page 15 Statement of findings Page 16 Identification methods Page 20 Summary Page 22 Z-Scores Page 23 Sample 3 Analysis Page 25 Identified substances Page 25 Statement of findings Page 27 Identification methods Page 31 Summary Page 33 Z-Scores Page 34 Sample 4 Analysis Page 36 Identified substances Page 36 Statement of findings Page 38 Identification methods Page 42 Summary Page 44 Test Samples Information Samples Comments on samples Sample 1 To prepare BS-1, urine was spiked with 4-Bromo-2,5-dimethoxyphenethylamine (2C-B) (1590 ng base/ml), as an ethanolic solution. The spiked urine was dispensed in 50ml aliquots and lyophilised Sample 2 To prepare BS-2, urine was spiked with Gammahydroxybutyrate (GHB) (14360 ng base/ml), as an aqueous solution. The spiked urine was dispensed in 50ml aliquots and lyophilised Sample 3 To prepare BS-3, urine was spiked with Amfetamine sulphate (1570ng/ml, 1150 ng base/ml) and Metamfetamine hydrochloride (4290 ng/ml, 3450 ng base/ml) as aqueous solutions. The spiked urine was dispensed in 50ml aliquots and lyophilised Sample 4 BS-4 was a blank test sample containing no substances in the ICE menu Samples Substances Concentrations Comments on substances Sample 1 4-Bromo-2,5-dimethoxyphenethylamine (2C- 1590 ng/ml B) Sample 2 gamma-Hydroxybutyric acid (GHB) 14360 ng/ml Sample 3 Metamfetamine 3450 ng/ml Amfetamine 1150 ng/ml Sample 4 [blank sample] This report contains the data received from laboratories participating in the current exercise. -

Structure-Cytotoxicity Relationship Profile of 13 Synthetic Cathinones In
Neurotoxicology 75 (2019) 158–173 Contents lists available at ScienceDirect Neurotoxicology journal homepage: www.elsevier.com/locate/neuro Structure-cytotoxicity relationship profile of 13 synthetic cathinones in differentiated human SH-SY5Y neuronal cells T ⁎ Jorge Soaresa, , Vera Marisa Costaa, Helena Gasparb,c, Susana Santosd,e, Maria de Lourdes Bastosa, ⁎ Félix Carvalhoa, João Paulo Capelaa,f, a UCIBIO, REQUIMTE (Rede de Química e Tecnologia), Laboratório de Toxicologia, Departamento de Ciências Biológicas, Faculdade de Farmácia, Universidade do Porto, Portugal b BioISI – Instituto de Biossistemas e Ciências Integrativas, Faculdade de Ciências, Universidade de Lisboa, Portugal c MARE - Centro de Ciências do Mar e do Ambiente, Escola Superior de Turismo e Tecnologia do Mar, Instituto Politécnico de Leiria, Portugal d Centro de Química e Bioquímica (CQB), Departamento de Química e Bioquímica, Faculdade de Ciências, Universidade de Lisboa, Portugal e Centro de Química Estrutural, Faculdade de Ciências, Universidade de Lisboa, Portugal f FP-ENAS (Unidade de Investigação UFP em Energia, Ambiente e Saúde), CEBIMED (Centro de Estudos em Biomedicina), Faculdade de Ciências da Saúde, Universidade Fernando Pessoa, Portugal ARTICLE INFO ABSTRACT Keywords: Synthetic cathinones also known as β-keto amphetamines are a new group of recreational designer drugs. We Synthetic cathinones aimed to evaluate the cytotoxic potential of thirteen cathinones lacking the methylenedioxy ring and establish a Classical amphetamines putative structure-toxicity profile using differentiated SH-SY5Y cells, as well as to compare their toxicity to that Cytotoxicity of amphetamine (AMPH) and methamphetamine (METH). Cytotoxicity assays [mitochondrial 3-(4,5-dimethyl-2- SH-SY5Y cells thiazolyl)-2,5-diphenyl-2H-tetrazolium bromide (MTT) reduction and lysosomal neutral red (NR) uptake] per- Structure-toxicity relationship formed after a 24-h or a 48-h exposure revealed for all tested drugs a concentration-dependent toxicity. -

Booklet 4 Stimulants Preface
4 STIMULANTS 4 STIMULANTS 2019 2019 © United Nations, June 2019. All rights reserved worldwide. ISBN: 978-92-1-148314-7 eISBN: 978-92-1-004174-4 United Nations publication, Sales No. E.19.XI.8 This publication may be reproduced in whole or in part and in any form for educational or non-profit purposes without special permission from the copyright holder, provided acknowledgement of the source is made. The United Nations Office on Drugs and Crime (UNODC) would appreciate receiving a copy of any publication that uses this publication as a source. Suggested citation: World Drug Report 2019 (United Nations publication, Sales No. E.19.XI.8). No use of this publication may be made for resale or any other commercial purpose whatsoever without prior permission in writing from UNODC. Applications for such permission, with a statement of purpose and intent of the reproduction, should be addressed to the Research and Trend Analysis Branch of UNODC. DISCLAIMER The content of this publication does not necessarily reflect the views or policies of UNODC or contributory organizations, nor does it imply any endorsement. Comments on the report are welcome and can be sent to: Division for Policy Analysis and Public Affairs United Nations Office on Drugs and Crime PO Box 500 1400 Vienna Austria Tel: (+43) 1 26060 0 Fax: (+43) 1 26060 5827 E-mail: [email protected] Website: www.unodc.org/wdr2019 PREFACE The findings of this year’s World Drug Report fill in same time clamping down on organized crime and and further complicate the global picture of drug trafficking. -

Toxicology Report Division of Toxicology Daniel D
Franklin County Forensic Science Center Office of the Coroner Anahi M. Ortiz, M.D. 2090 Frank Road Columbus, Ohio 43223 Toxicology Report Division of Toxicology Daniel D. Baker, Chief Toxicologist Casey Goodson Case # LAB-20-5315 Date report completed: January 28, 2021 A systematic toxicological analysis has been performed and the following agents were detected. Postmortem Blood: Gray Top Thoracic ELISA Screen Acetaminophen Not Detected ELISA Screen Barbiturates Not Detected ELISA Screen Benzodiazepines Not Detected ELISA Screen Benzoylecgonine Not Detected ELISA Screen Buprenorphine Not Detected ELISA Screen Cannabinoids See Confirmation ELISA Screen Fentanyl Not Detected ELISA Screen Methamphetamine Not Detected ELISA Screen Naltrexone/Naloxone Not Detected ELISA Screen Opiates Not Detected ELISA Screen Oxycodone/Oxymorphone Not Detected ELISA Screen Salicylates Not Detected ELISA Screen Tricyclics Not Detected Page 1 of 4 Casey Goodson Case # LAB-20-5315 GC/FID Ethanol Not Detected GC/MS Acidic/Neutral Drugs None Detected GC/MS Nicotine Positive GC/MS Cotinine Positive Reference Lab Delta-9-THC 13 ng/mL Reference Lab 11-Hydroxy-Delta-9-THC 1.2 ng/mL Reference Lab 11-Nor-9-Carboxy-Delta-9-THC 15 ng/mL Postmortem Urine: Gray Top Urine GC/MS Cotinine Positive This report has been verified as accurate and complete by ______________________________________ Daniel D. Baker, M.S., F-ABFT Cannabinoid quantitations in blood were performed by NMS Labs, Horsham, PA. Page 2 of 4 Casey Goodson Case # LAB-20-5315 Postmortem Toxicology Scope of Analysis Franklin County Coroner’s Office Division of Toxicology Enzyme Linked Immunosorbant Assay (ELISA) Blood Screen: Qualitative Presumptive Compounds/Classes: Acetaminophen (cut-off 10 µg/mL), Benzodiazepines (cut-off 20 ng/mL), Benzoylecgonine (cut-off 50 ng/mL), Cannabinoids (cut-off 40 ng/mL), Fentanyl (cut-off 1 ng/mL), Methamphetamine/MDMA (cut-off 50 ng/mL), Opiates (cut-off 40 ng/mL), Oxycodone/Oxymorphone (cut-off 40 ng/mL), Salicylates (50 µg/mL). -

4F-Pentedrone
NMS Labs 2300 Stratford Ave Willow Grove, PA 19090 4F-Pentedrone Sample Type: Seized Material Latest Revision: December 3, 2019 Date Received: August 16, 2019 Date of Report: December 3, 2019 1. GENERAL INFORMATION IUPAC Name: 1-(4-fluorophenyl)-2-(methylamino)pentan-1-one InChI String: InChI=1S/C12H16FNO/c1-3-4-11(14-2)12(15)9-5-7-10(13)8-6- 9/h5-8,11,14H,3-4H2,1-2H3 CFR: Not Scheduled (12/2019) CAS# Not Available Synonyms: 4-Fluoro Pentedrone, 4-Fluoro-α-Methylamino-Valerophenone, 4-FPD Source: Department of Homeland Security Appearance: Tan Solid Material Important Note: All identifications were made based on evaluation of analytical data (GC-MS and LC- QTOF-MS) in comparison to analysis of acquired reference material. Prepared By: Alex J. Krotulski, PhD; Melissa F. Fogarty, MSFS, D-ABFT-FT; and Barry K. Logan, PhD, F-ABFT 2. CHEMICAL AND PHYSICAL DATA 2.1 CHEMICAL DATA Chemical Molecular Molecular Ion Exact Mass Form Formula Weight [M+] [M+H]+ Base C12H16FNO 209.3 209 210.1289 3. BRIEF DESCRIPTION 4F-Pentedrone is classified as a novel stimulant and substituted cathinone. Substituted cathinones are modified based on the structure of cathinone, an alkaloid found in the Khat plant. Novel stimulants have been reported to cause stimulant-like effects, similar to amphetamines. Novel stimulants have also caused adverse events, including deaths, as described in the literature. Structurally similar compounds include pentedrone, hexedrone, and N-ethyl hexedrone. Pentedrone is a Schedule I substance in the United States while 4F-pentedrone is not explicitly scheduled. -

AGENDA Friday, September 9, 2016 7:00 A.M
Needham Board of Health AGENDA Friday, September 9, 2016 7:00 a.m. – 9:00 a.m. Charles River Room – Public Services Administration Building 500 Dedham Avenue, Needham MA 02492 • 7:00 to 7:05 - Welcome & Review of Minutes (July 29 & August 29) • 7:05 to 7:30 - Director and Staff Reports (July & August) • 7:30 to 7:45 - Discussion about Proposed Plastic Bag Ban Christopher Thomas, Needham Resident • 7:45 to 7:50 - Off-Street Drainage Bond Discussion & Vote • 7:50 to 8:00 - Update on Wingate Pool Variance Application * * * * * * * * * * * * * Board of Health Public Hearing • 8:00 to 8:40 - Hearing for Proposed New or Amended BOH Regulations o Body Art o Synthetic Marijuana o Drug Paraphernalia • 8:40 to 8:50 - Board Discussion of Policy Positions • Other Items (Healthy Aging, Water Quality) • Next Meeting Scheduled for Friday October 14, 2016 • Adjournment (Please note that all times are approximate) 1471 Highland Avenue, Needham, MA 02492 781-455-7500 ext 511 (tel); 781-455-0892 (fax) E-mail: [email protected] Web: www.needhamma.gov/health NEEDHAM BOARD OF HEALTH July 29, 2016 MEETING MINUTES PRESENT: Edward V. Cosgrove, PhD, Chair, Jane Fogg, Vice-Chair, M.D., and Stephen Epstein, M.D STAFF: Timothy McDonald, Director, Donna Carmichael, Catherine Delano, Maryanne Dinell, Tara Gurge GUEST: Kevin Mulkern, Aquaknot Pools, Inc., Keith Mulkern, Aquaknot Pools, Inc., David Friedman, Wingate, Paul Humphreys, Michael Tomasello, Callahan, Inc. CONVENE: 7:00 a.m. – Public Services Administration Building (PSAB), 500 Dedham Avenue, Needham MA 02492 DISCUSSION: Call To Order – 7:06 a.m. – Dr. Cosgrove, Chairman APPROVE MINUTES: Upon motion duly made and seconded, the minutes of the BOH meeting of June 17, 2016 were approved as submitted. -

Application of High Resolution Mass Spectrometry for the Screening and Confirmation of Novel Psychoactive Substances Joshua Zolton Seither [email protected]
Florida International University FIU Digital Commons FIU Electronic Theses and Dissertations University Graduate School 4-25-2018 Application of High Resolution Mass Spectrometry for the Screening and Confirmation of Novel Psychoactive Substances Joshua Zolton Seither [email protected] DOI: 10.25148/etd.FIDC006565 Follow this and additional works at: https://digitalcommons.fiu.edu/etd Part of the Chemistry Commons Recommended Citation Seither, Joshua Zolton, "Application of High Resolution Mass Spectrometry for the Screening and Confirmation of Novel Psychoactive Substances" (2018). FIU Electronic Theses and Dissertations. 3823. https://digitalcommons.fiu.edu/etd/3823 This work is brought to you for free and open access by the University Graduate School at FIU Digital Commons. It has been accepted for inclusion in FIU Electronic Theses and Dissertations by an authorized administrator of FIU Digital Commons. For more information, please contact [email protected]. FLORIDA INTERNATIONAL UNIVERSITY Miami, Florida APPLICATION OF HIGH RESOLUTION MASS SPECTROMETRY FOR THE SCREENING AND CONFIRMATION OF NOVEL PSYCHOACTIVE SUBSTANCES A dissertation submitted in partial fulfillment of the requirements for the degree of DOCTOR OF PHILOSOPHY in CHEMISTRY by Joshua Zolton Seither 2018 To: Dean Michael R. Heithaus College of Arts, Sciences and Education This dissertation, written by Joshua Zolton Seither, and entitled Application of High- Resolution Mass Spectrometry for the Screening and Confirmation of Novel Psychoactive Substances, having been approved in respect to style and intellectual content, is referred to you for judgment. We have read this dissertation and recommend that it be approved. _______________________________________ Piero Gardinali _______________________________________ Bruce McCord _______________________________________ DeEtta Mills _______________________________________ Stanislaw Wnuk _______________________________________ Anthony DeCaprio, Major Professor Date of Defense: April 25, 2018 The dissertation of Joshua Zolton Seither is approved. -

Written Witness Statement for U.S. Sentencing Commission's Public
STATEMENT OF TERRENCE L. BOOS, PH.D. SECTION CHIEF DRUG AND CHEMICAL EVALUATION SECTION DIVERSION CONTROL DIVISION DRUG ENFORCEMENT ADMINISTRATION and CASSANDRA PRIOLEAU, PH.D. DRUG SCIENCE SPECIALIST DRUG AND CHEMICAL EVALUATION SECTION DIVERSION CONTROL DIVISION DRUG ENFORCEMENT ADMINISTRATION - - - BEFORE THE UNITED STATES SENTENCING COMMISSION - - - HEARING ON SENTENCING POLICY FOR SYNTHETIC DRUGS - - - OCTOBER 4, 2017 WASHINGTON, D.C. 1 Introduction New Psychoactive Substances (NPS) are substances trafficked as alternatives to well- studied controlled substances of abuse. NPS have demonstrated adverse health effects such as paranoia, psychosis, and seizures to name a few. Cathinones, cannabinoids, and fentanyl-related substances are the most common NPS drug classes encountered on the illicit drug market, all with negative consequences for the user to include serious injury and death. Our early experience saw substances being introduced from past research efforts in an attempt to evade controls. This has evolved to NPS manufacturers structurally altering substances at a rapid pace with unknown outcomes to targeting specific user populations. These substances represent an unprecedented level of diversity and consequences. Due to clandestine manufacture and unscrupulous trafficking, the user is at great risk. A misconception exists that these substances carry a lower risk of harm In reality, published reports from law enforcement, emergency room physicians and scientists, accompanied with autopsies from medical examiners, have clearly demonstrated the harmful and potentially deadly consequences of using synthetic cathinones. These substances are introduced in an attempt to circumvent drug controls and the recent flood of NPS remains a challenge for law enforcement and public health. The United Nations Office on Drugs and Crime reported over 700 NPS encountered.1 The manufacturers and traffickers make minor changes in the chemical structure of known substances of abuse and maintain the pharmacological effect. -

Federal Register/Vol. 82, No. 7/Wednesday, January 11, 2017
3326 Federal Register / Vol. 82, No. 7 / Wednesday, January 11, 2017 / Notices is responsible for oversight and DEPARTMENT OF HEALTH AND such as medical information, your or implementation of the MSP provisions HUMAN SERVICES anyone else’s Social Security number, or as part of its overall authority for the confidential business information, such Medicare program. The CMS Food and Drug Administration as a manufacturing process. Please note accomplishes this through a [Docket No. FDA–2016–N–4619] that if you include your name, contact combination of direct CMS action and information, or other information that work by CMS’ contractors. The CMS International Drug Scheduling; identifies you in the body of your efforts include policy and operational Convention on Psychotropic comments, that information will be guidelines, including regulations (as Substances; Single Convention on posted on https://www.regulations.gov. • If you want to submit a comment necessary), as well as oversight over Narcotic Drugs; World Health with confidential information that you contractor MSP responsibilities. As a Organization; Scheduling Recommendations; 4- do not wish to be made available to the result of litigation in the mid-1990’s, public, submit the comment as a certain GHP insurers were mandated to Methylethcathinone and Nine Other Substances; Request for Comments written/paper submission and in the report coverage information for a manner detailed (see ‘‘Written/Paper number of years. Subsequent to this AGENCY: Food and Drug Administration, Submissions’’ and ‘‘Instructions’’). litigation related mandatory reporting, HHS. Written/Paper Submissions CMS instituted a Voluntary Data ACTION: Notice. Sharing Agreement (VDSA) effort which Submit written/paper submissions as expanded the scope of the GHP SUMMARY: The Food and Drug follows: • participants and added some NGHP Administration (FDA) is providing Mail/Hand delivery/Courier (for participants. -
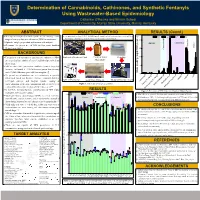
Determination of Cannabinoids, Cathinones, and Synthetic Fentanyls Using Wastewater-Based Epidemiology
Determination of Cannabinoids, Cathinones, and Synthetic Fentanyls Using Wastewater-Based Epidemiology Catherine O’Rourke and Bikram Subedi Department of Chemistry, Murray State University, Murray, Kentucky ABSTRACT ANALYTICAL METHOD RESULTS (Contd.) Develop an analytical method capable of determining a wide An analytical method (UPLC-MS/MS based) capable of determining trace levels of New C1 C2 C3 C4 Psychoactive Substances in wastewater was developed and validated. range of new psychoactive substances (NPS) in wastewater. 20 Optimize sample preparation and instrumental analysis. Opioids Cathinones Determine the prevalence of NPS in four rural Southern Piperizine Indole Illinois communities. 15 Cannabinoid BACKGROUND Unregulated new narcotics or psychoactive substances (NPS) Wastewater Treatment Plant Certified Amber Centrifuge 10 are created to have similar effects of established prescribed and Glass Bottle illicit drugs.1 5 NPS are often more potent than established abused drugs. For instance, carfentanil is ~100 folds more potent than fentanyl and ~10,000 folds more powerful than morphine.1 Mass Loading (mg/d/1000 people) 0 The prevalence of substance use in a community is typically 5IT determined based on forensic evidence, criminal statistics, mCPP Solvent Evaporator Solid Phase Extractor Vacuum Filtration (1 µm) MMMP self-report surveys, and hospital reports, causing an Carfentanil Figure 1. Schematic of sample preparation Methcathinone underestimation of the drug consumption and a delay between Furanyl Fentanyl MAB-CHMINACA a drug outbreak and intervention of law enforcement.2-4 4-Methyl Pentedrone Methoxyacetyl Fentanyl In the U.S., the total forensic identifications of NPS tripled RESULTS Figure 3. Prevalence of NPS in four rural Southern Illinois Counties 5 from 2016 (684) to 2019 (2023). -

Characterization of Hepatotoxicity Mechanisms Triggered by Designer Cathinone Drugs
ToxSci Advance Access published July 3, 2016 TOXICOLOGICAL SCIENCES, 2016, 1–14 doi: 10.1093/toxsci/kfw105 Advance Access Publication Date: June 2, 2016 Research article Characterization of Hepatotoxicity Mechanisms Triggered by Designer Cathinone Drugs (b-Keto Amphetamines) Maria Joao~ Valente,* Ana Margarida Araujo,* Maria de Lourdes Bastos,* † Eduarda Fernandes, Fe´lix Carvalho,* Paula Guedes de Pinho,* Downloaded from Marcia Carvalho*,‡,1 *UCIBIO, REQUIMTE, Laboratory of Toxicology, Faculty of Pharmacy, University of Porto, Porto, Portugal; †UCIBIO, REQUIMTE, Laboratory of Applied Chemistry, Faculty of Pharmacy, University of Porto, Porto, Portugal; and ‡FP-ENAS, CEBIMED, Fundac¸ao~ Ensino e Cultura Fernando Pessoa, Porto, Portugal http://toxsci.oxfordjournals.org/ 1To whom correspondence should be addressed at FP-ENAS, CEBIMED, Fundac¸ao~ Ensino e Cultura Fernando Pessoa, PrauˆI¨a 9 de Abril, 349, 4249-004 Porto, Portugal. Fax: +351 225074630. E-mail address: [email protected]. ABSTRACT The use of cathinone designer drugs in recreational settings has been associated with severe toxic effects, including liver damage. The precise mechanisms by which cathinones induce hepatotoxicity and whether they act by common pathways remain to be elucidated. Herein, we assessed the toxicity of the cathinones methylone, pentedrone, 3,4- by guest on July 4, 2016 methylenedioxypyrovalerone (MDPV) and 4-methylethcathinone (4-MEC) in primary rat hepatocytes (PRH) and HepaRG cells, and compared with that of 3,4-methylenedioxymethamphetamine (MDMA). MDPV and pentedrone were significantly more toxic than MDMA, while methylone was the least cytotoxic compound. Importantly, PRH revealed to be the most sensitive experimental model and was thus used to explore the mechanisms underlying the observed toxicity. -

LJMU Research Online
LJMU Research Online Brunt, TM, Atkinson, AM, Nefau, T, Martinez, M, Lahaie, E, Malzcewski, A, Pazitny, M, Belackova, V and Brandt, SD Online test purchased new psychoactive substances in 5 different European countries; a snapshot study of chemical composition and price http://researchonline.ljmu.ac.uk/id/eprint/6048/ Article Citation (please note it is advisable to refer to the publisher’s version if you intend to cite from this work) Brunt, TM, Atkinson, AM, Nefau, T, Martinez, M, Lahaie, E, Malzcewski, A, Pazitny, M, Belackova, V and Brandt, SD (2017) Online test purchased new psychoactive substances in 5 different European countries; a snapshot study of chemical composition and price. International Journal of Drug LJMU has developed LJMU Research Online for users to access the research output of the University more effectively. Copyright © and Moral Rights for the papers on this site are retained by the individual authors and/or other copyright owners. Users may download and/or print one copy of any article(s) in LJMU Research Online to facilitate their private study or for non-commercial research. You may not engage in further distribution of the material or use it for any profit-making activities or any commercial gain. The version presented here may differ from the published version or from the version of the record. Please see the repository URL above for details on accessing the published version and note that access may require a subscription. For more information please contact [email protected] http://researchonline.ljmu.ac.uk/ Elsevier Editorial System(tm) for International Journal of Drug Policy Manuscript Draft Manuscript Number: DRUGPO-D-16-359R2 Title: Online test purchased new psychoactive substances in 5 different European countries; a snapshot study of chemical composition and price Article Type: Research Paper Keywords: webshops; NPS; purity; price; chemical analysis; European Union Corresponding Author: Dr.