B1000084 US Rev 1 T2 Recon.Indd
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

An Early Turning Point in the History of the Crusades
Jonathan Phillips. The Second Crusade: Extending the Frontiers of Christendom. New Haven: Yale University Press, 2007. xxix + 364 pp. $40.00, cloth, ISBN 978-0-300-11274-0. Reviewed by Jonathan R. Lyon Published on H-German (March, 2008) As the author makes clear in the excellent in‐ cepts could be employed against a variety of Latin troduction to this work, the Second Crusade Christendom's enemies. (1145-49) has typically not attracted as much in‐ Phillips divides his work into fourteen terest from modern historians as the more fa‐ chronologically-arranged chapters, although sepa‐ mous First Crusade (1095-99) and Third Crusade rate chapters treat the Iberian and Baltic compo‐ (1188-92). A key explanation for this trend is the nents of the crusade. The frst two chapters dis‐ Second Crusade's failure to make any significant cuss the period between the First and the Second gains for the Christians of the Holy Land in the Crusade; chapter 1 focuses on the various pilgrim‐ wake of the Muslim conquest of Edessa in 1144. ages and crusading efforts of the early twelfth Nevertheless, as Phillips convincingly argues, this century, and chapter 2 provides a rich, fascinating crusade--despite its lack of success--demands discussion of the powerful legacy the First Cru‐ more attention than it has received for several sade left to Latin Christian culture in the decades reasons. It was the frst crusade to the Holy Land after 1099. Phillips persuasively argues that this to involve western European kings and thus legacy had a significant impact on recruiting for forced rulers to consider the consequences of the Second Crusade, because the generation of leaving their kingdoms for months (if not years) young nobles alive in the 1140s had grown up at a time. -

Personal Names and Denomination of Livonians in Early Written Sources
ESUKA – JEFUL 2014, 5–1: 13–26 PERSONAL NAMES AND DENOMINATION OF LIVONIANS IN EARLY WRITTEN SOURCES Enn Ernits Estonian University of Life Sciences Abstract. This paper presents the timeline of ethnonyms denoting Livonians; specifies their chronology; and analyses the names used for this ethnos and possible personal names. If we consider the dating of the event, the earliest sources mentioning Livonians are Gesta Danorum and the Tale of Bygone Years (both 10th century), but both sources present rather dubious information: in the first the battle of Bråvalla itself or the date are dubious (6th, 8th or 10th century); in the latter we cannot be sure that the member of the Rus delegation was really a Livonian. If we consider the time of recording, the earliest sources are two rune inscriptions from Sweden (11th century), and the next is the list of neighbouring peoples of the Russians from the Tale of Bygone Years (12th century). The personal names Bicco and Ger referred in Gesta Danorum, and Либи Аръфастовъ in Tale of Bygone Years are very problematic. The first certain personal name of a Livonian is *Mustakka, *Mustukka or *Mustoikka (from Finnic *musta ‘black’) written in 1040–1050s on a strip of birch bark in Novgorod. Keywords: Livs, Finnic peoples, ethnonyms, anthroponyms, onomastics DOI: http://dx.doi.org/10.12697/jeful.2014.5.1.01 1. Introduction This paper (1) seeks to present the timeline of ethnonyms denoting Livonians; (2) to specify their chronology; (3) and to analyse the names used for this ethnos and possible personal names. It is supple- mental to the paper by Mauno Koski on words denoting Livonians (Koski 2011). -
Charters: What Survives?
Banner 4-final.qxp_Layout 1 01/11/2016 09:29 Page 1 Charters: what survives? Charters are our main source for twelh- and thirteenth-century Scotland. Most surviving charters were written for monasteries, which had many properties and privileges and gained considerable expertise in preserving their charters. However, many collections were lost when monasteries declined aer the Reformation (1560) and their lands passed to lay lords. Only 27% of Scottish charters from 1100–1250 survive as original single sheets of parchment; even fewer still have their seal attached. e remaining 73% exist only as later copies. Survival of charter collectionS (relating to 1100–1250) GEOGRAPHICAL SPREAD from inStitutionS founded by 1250 Our picture of documents in this period is geographically distorted. Some regions have no institutions with surviving charter collections, even as copies (like Galloway). Others had few if any monasteries, and so lacked large charter collections in the first place (like Caithness). Others are relatively well represented (like Fife). Survives Lost or unknown number of Surviving charterS CHRONOLOGICAL SPREAD (by earliest possible decade of creation) 400 Despite losses, the surviving documents point to a gradual increase Copies Originals in their use in the twelh century. 300 200 100 0 109 0s 110 0s 111 0s 112 0s 113 0s 114 0s 115 0s 116 0s 1170s 118 0s 119 0s 120 0s 121 0s 122 0s 123 0s 124 0s TYPES OF DONOR typeS of donor – Example of Melrose Abbey’s Charters It was common for monasteries to seek charters from those in Lay Lords Kings positions of authority in the kingdom: lay lords, kings and bishops. -

VWR Circulators and Chillers
VWR Circulators and Chillers Superior Temperature Control Equipment Clockwise from top left: 13721-200, 13721-172, 13721-138, 13721-082 Controllers Table of Contents. Page Product Features. 2-3 Precise Controllers Controllers . 4-5 Choice of four controllers. From state-of-the-art program- VWR Signature` mable designs that provide Refrigerated/Heating ultimate control, to the analog Circulating Baths. 6-10 design that is perfect for less demanding applications. How To Choose A Chiller . 11 VWR Signature Recirculating Chillers . 12-13 VWR Signature Heating Immersion Circulator. 14 Durable Design VWR` Open Bath Systems . 15 Immersed parts and reservoirs are made of corrosion-fighting VWR Signature stainless steel. The exterior Heating Circulating Baths . 16-17 surface is a tough powder coating for easy clean-up. VWR Refrigerated/Heating Circulating Baths. 18-21 VWR Immersion & Flow-Through Coolers . 22 VWR Ambient Bath Cooler. 22 Double Safety VWR Heating Recirculator . 22 Your equipment and work are protected with redundant over VWR Heating Immersion Circulators . 23 temperature and low liquid cutoff standard on all circula- VWR Heating Circulating Baths . 24-25 tors. 60Hz models are CSA approved, 50Hz models carry Accessories . 26 the CE mark. At-a-Glance Chart . 27 Environmentally Responsible VWR Refrigerated Circulators and Chillers use R-134a refrigerant, and no ozone- depleting CFC’s are used in the manufacturing process. All instruments are manufactured in an ISO 9001 accredited facility. 2 To order, call 1-800-932-5000 or visit vwr.com Controllers Time Savers Advanced refrigeration sys- tems and high wattage heaters respond quickly to temperature changes. You'll have minimum waiting time for your circulator to stabilize. -
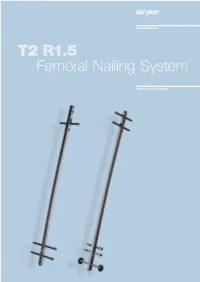
T2 R1.5 Femoral Nailing System
T2 R1.5 Femoral Nailing System Operative Technique Femoral Nailing System Contributing Surgeons Prof. Dr. med. Volker Bühren Chief of Surgical Services Medical Director of Murnau Trauma Center Murnau Germany Joseph D. DiCicco III, D. O. Director Orthopaedic Trauma Service Good Samaritan Hospital Dayton, Ohio Associate Clinical Professor of Orthopeadic Surgery Ohio University and Wright State University USA Thomas G. DiPasquale, D. O. Medical Director, Orthopedic Trauma Services Director, Orthopedic Trauma Fellowship and This publication sets forth detailed Orthopedic Residency Programs recommended procedures for using York Hospital Stryker Osteosynthesis devices and York instruments. USA It offers guidance that you should heed, but, as with any such technical guide, each surgeon must consider the particular needs of each patient and make appropriate adjustments when and as required. A workshop training is required prior to first surgery. All non-sterile devices must be cleaned and sterilized before use. Follow the instructions provided in our reprocessing guide (L24002000). Multi-component instruments must be disassembled for cleaning. Please refer to the corresponding assembly/ disassembly instructions. See package insert (L22000007) for a complete list of potential adverse effects, contraindications, warnings and precautions. The surgeon must discuss all relevant risks, including the finite lifetime of the device, with the patient, when necessary. Warning: Fixation Screws: Stryker Ostreosynthesis bone screws are not approved or intended for screw attachment or fixation to the posterior elements (pedicles) of the cervical, thoracic or lumbar spine. 2 Contents Page 1. Introduction 4 Implant Features 4 Instrument Features 6 References 6 2. Indications, Precautions and Contraindications 7 Indications 7 Precautions 7 Relative Contraindications 7 3. -

Hildegard Transfigured – Programme Copy 2021(1)
Hildegard Transfigured: a medieval trance for the 21st century Hildegard Transfigured is a collaborative piece of concert-theatre by vocal trio Voice, visual artist Innerstrings, and composer Laura Moody that celebrates St. Hildegard of Bingen through song, psychedelic lights, and live visuals. The performance at SJE includes the world premiere of Moody’s Hildegard Portraits. St Hildegard of Bingen (1098 - 1179) joined the monastery in Disibodenberg (in German Rhineland) when she was just eight years old and would stay there for nearly forty years, eventually becoming abbess in 1136. She founded her own abbey at Rupertsberg near Bingen in 1147 and a second monastery in nearby Eibingen in 1165. Throughout her life, Hildegard was a great spiritual leader, theologian, mystic, scientist, and composer. Revered as a saint for centuries, Pope Benedict XVI canonised Hildegard of Bingen on 10 May 2012. Hildegard experienced intense visions, recorded in her major work Scivias (Know the Way), (1141-51), and it is this aspect of her life that the collaboration with visual artist, Innerstrings, will bring to life in Hildegard Transfigured, transfiguring her beautiful music into a new sensory experience. Laura Moody’s research for the show brought her to The Personal Correspondence of Hildegard of Bingen, translated by Joseph L Baird and Radd K Ehrman (OUP 2006). She has set extracts and fragments of Hildegard’s letters in her composition Hildegard Portraits, written especially for this programme. You will hear Moody's music interspersed throughout in the form of miniatures, culminating in the finale The Living Light. “It is some kind of miracle to have the kind of access to a female creator of the twelfth century that we have with Hildegard, her output only having been permissible during her lifetime because of her sacred status. -
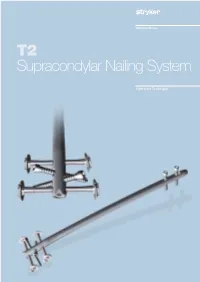
T2 Supracondylar Nailing System
T2 Supracondylar Nailing System Operative Technique Supracondylar Nailing System Contributing Surgeons Prof. Dr. med. Volker Bühren Chief of Surgical Services Medical Director of Murnau Trauma Center Murnau Germany Dean C. Maar, M.D. Methodist Hospital − Indianapolis Indianapolis Indiana USA James Maxey, M.D. Clinical Assistant Professor University of Illinois College of Medicine Peoria, IL USA This publication sets forth detailed recommended procedures for using Stryker Osteosynthesis devices and instruments. It offers guidance that you should heed, but, as with any such technical guide, each surgeon must consider the particular needs of each patient and make appropriate adjustments when and as required. A workshop training is required prior to first surgery. All non-sterile devices must be cleaned and sterilized before use. Follow the instructions provided in our reprocessing guide (L24002000). Multi-component instruments must be disassembled for cleaning. Please refer to the corresponding assembly/ disassembly instructions. See package insert (L22000007) for a complete list of potential adverse effects, contraindications, warnings and precautions. The surgeon must discuss all relevant risks, including the finite lifetime of the device, with the patient, when necessary. Warning: All bone screws referenced in this document here are not approved for screw attachment or fixation to the posterior elements (pedicles) of the cervical, thoracic or lumbar spine. 2 Contents Page 1. Introduction 4 Implant Features 4 Technical Details 5 Instrument -

Downloaded from Brill.Com09/24/2021 05:15:28PM Via Free Access 318 Faletra Empire
Chapter 11 Colonial Preoccupations in Geoffrey of Monmouth’s De gestis Britonum Michael Faletra Nearly three quarters of the way through the sweep of legendary history that constitutes Geoffrey of Monmouth’s De gestis Britonum, the narrative grinds almost to a halt. Whereas parts of the history had glossed over dozens of kings and hundreds of years, sometimes in a page or two, the pace of events lead- ing up to the reign of King Arthur had steadily slowed, only to arrive at a near standstill in Geoffrey’s description of Arthur’s Plenary Court. It is a moment of great political importance, the celebration of the king’s victory both over the Saxons who had plagued the realm for a generation and over much of what is now France: like several of his more successful predecessors on the British throne, Arthur returns to Britain a conqueror. The Plenary Court held to stage Arthur’s coronation and to celebrate his glorious new order takes place on Pentecost in the Welsh city of Caerleon: “Located in Glamorgan on the River Usk at a lovely site not far from where the Severn empties into the sea, it had an abundance of riches greater than that of any other city and was thus an excellent place to hold a high feast.”1 No expense is spared, Geoffrey reminds his Anglo-Norman readers, and he treats them to lavish descriptions of the coronation processions, the splendid regalia, the celebratory games, and the feasting for many hundreds of guests – all of which seem calculated to drive home the fact that ancient Britain had attained a cultural pinnacle: -
Operators Manual Programmable / Digital Controller Models Manuel
Operators Manual Programmable / Digital Controller Models Pages 3 - 41 Manuel de l’utilisateur Modèles des Contrôleurs Numériques / Programmables Pages 42 - 78 Bedienungsanleitung Programmierbare/Digitale Regler Modelle Seiten 79 - 117 110-229 9/28/09 1 WEEE Directive A label with a crossed-out wheeled bin symbol and a rectangular bar indicates that the product is covered by the Waste Electrical and Electronic Equipment (WEEE) Directive and is not to be disposed of as unsorted municipal waste. Any products marked with this symbol must be collected separately, according to the regulatory guidelines in your area. or The objectives of this program are to preserve, protect and improve the quality of the environment, protect human health, and utilize natural resources prudently and rationally. Specific treatment of WEEE is indispensable in order to avoid the dispersion of pollutants into the recycled material or waste stream. Such treatment is the most effective means of protecting the customer’s environment. Requirements for waste collection, reuse, recycling, and recovery programs vary by regulatory authority at your location. Contact your local responsible body (e.g., your laboratory manager) or authorized representative for information regarding applicable disposal regulations. Contact PolyScience at the web site listed below for information. Web address: www.polyscience.com Customer Care: 1-800-229-7569 (inside the USA) (+1) 847-647-0611 (outside the USA) Fax 1-847-647-1155 2 13R, 712, 7306, 7312, 812, 8006, 8012, 8002, 8112, 8102, 8106, -

The Eucharist in Twelfth-Century Literature
University of Arkansas, Fayetteville ScholarWorks@UARK Theses and Dissertations 5-2016 Hoc Est Corpus Meum: The uchE arist in Twelfth- Century Literature Lindsey Zachary Panxhi University of Arkansas, Fayetteville Follow this and additional works at: http://scholarworks.uark.edu/etd Part of the History of Religion Commons, Medieval History Commons, and the Medieval Studies Commons Recommended Citation Panxhi, Lindsey Zachary, "Hoc Est Corpus Meum: The uchE arist in Twelfth-Century Literature" (2016). Theses and Dissertations. 1499. http://scholarworks.uark.edu/etd/1499 This Dissertation is brought to you for free and open access by ScholarWorks@UARK. It has been accepted for inclusion in Theses and Dissertations by an authorized administrator of ScholarWorks@UARK. For more information, please contact [email protected], [email protected]. Hoc Est Corpus Meum: The Eucharist in Twelfth-Century Literature A dissertation submitted in partial fulfillment of the requirements for the degree of Doctor of Philosophy in English by Lindsey Zachary Panxhi John Brown University Bachelor of Arts in English, 2009 University of Arkansas Master of Arts in English, 2011 May 2016 University of Arkansas This dissertation is approved for recommendation to the Graduate Council. _______________________________ Dr. William Quinn Dissertation Director _______________________________ ___________________________________ Dr. Joshua Byron Smith Dr. Mary Beth Long Committee Member Committee Member Abstract In “Hoc Est Corpus Meum: The Eucharist in Twelfth-Century Literature,” I analyze the appearance of the Eucharist as a sacred motif in secular lais, romances, and chronicles. The Eucharist became one of the most controversial intellectual topics of the High Middle Ages. While medieval historians and religious scholars have long recognized that the twelfth century was a critical period in which many eucharistic doctrines were debated and affirmed, literary scholars have given very little attention to the concurrent emergence of eucharistic themes in twelfth-century literature. -
ACE Appendix
CBP and Trade Automated Interface Requirements Appendix: PGA August 13, 2021 Pub # 0875-0419 Contents Table of Changes .................................................................................................................................................... 4 PG01 – Agency Program Codes ........................................................................................................................... 18 PG01 – Government Agency Processing Codes ................................................................................................... 22 PG01 – Electronic Image Submitted Codes .......................................................................................................... 26 PG01 – Globally Unique Product Identification Code Qualifiers ........................................................................ 26 PG01 – Correction Indicators* ............................................................................................................................. 26 PG02 – Product Code Qualifiers ........................................................................................................................... 28 PG04 – Units of Measure ...................................................................................................................................... 30 PG05 – Scientific Species Code ........................................................................................................................... 31 PG05 – FWS Wildlife Description Codes ........................................................................................................... -

3.2 Precipitation Or Dry-Wet Reconstructions
Climate change in China during the past 2000 years: An overview Ge Quansheng , Zheng Jingyun Institute of Geographic Sciences and Natural Resources Research, Chinese Academy of Sciences, Beijing 100101, China Email: [email protected] Outline 1 Introduction 2 Historical Documents as Proxy 3 Reconstructions and Analyses 4 Summary and Prospects 1. Introduction: E Asia2K Climate System Socio-economic System •typical East Asian •dense population and rapid monsoon climate economic development • significant seasonal and • be susceptible to global inter-annual and inter- warming and extreme decadal variability climate events Climate change study in the past 2ka in East Asian is both beneficial and advantageous. • various types of natural proxy • Plenty of historical documents Fig. Active regional working groups under as proxy the past 2ka theme (PAGES 2009) 2. Historical Documents as Proxy Type Period Amount Chinese classical 1,531 kinds, 137 BC~1470 AD documents 32,251 volumes More than 8,000 1471~1911 (The Ming Local gazettes books (部), 110, and Qing Dynasty) 000 volumes Memos to the About 120,000 1736~1911 emperor pieces Archives of the 1912~1949 20,000 volumes Republic of China More than 200 Private diaries 1550~ books (部) Chinese classical documents AD 833, North China plain: Extreme drought event was occurred, crops were shriveling, no yields, people were in hungry…. Fig. Example for Ancient Chinese writings Local gazettes The 28th year of the Daoguang reign (1848 AD), the 6th (lunar) month, strong wind and heavy rain, the Yangtze River overflowed; the 7th month, strong wind Fig. Gazettes of Yangzhou Prefecture and thunder storm, field published in 1874 AD and houses submerged.