World Health Organization Donor Update 2014 (Q2)
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Syria SITREP Map 07
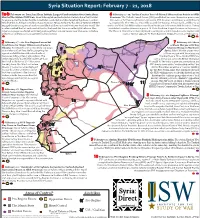
Syria Situation Report: February 7 - 21, 2018 1a-b February 10: Israel and Iran Initiate Largest Confrontation Over Syria Since 6 February 9 - 15: Turkey Creates Two Additional Observation Points in Idlib Start of the Syrian Civil War: Israel intercepted and destroyed an Iranian drone that violated Province: The Turkish Armed Forces (TSK) established two new observation points near its airspace over the Golan Heights. Israel later conducted airstrikes targeting the drone’s control the towns of Tal Tuqan and Surman in Eastern Idlib Province on February 9 and February vehicle at the T4 Airbase in Eastern Homs Province. Syrian Surface-to-Air Missile Systems (SAMS) 15, respectively. The TSK also reportedly scouted the Taftanaz Airbase north of Idlib City as engaged the returning aircraft and successfully shot down an Israeli F-16 over Northern Israel. The well as the Wadi Deif Military Base near Khan Sheikhoun in Southern Idlib Province. Turkey incident marked the first such combat loss for the Israeli Air Force since the 1982 Lebanon War. established a similar observation post at Al-Eis in Southern Aleppo Province on February 5. Israel in response conducted airstrikes targeting at least a dozen targets near Damascus including The Russian Armed Forces later deployed a contingent of military police to the regime-held at least four military positions operated by Iran in Syria. town of Hadher opposite Al-Eis in Southern Aleppo Province on February 14. 2 February 17 - 20: Pro-Regime Forces Set Qamishli 7 February 18: Ahrar Conditions for Major Offensive in Eastern a-Sham Merges with Key Ghouta: Pro-regime forces intensified a campaign 9 Islamist Group in Northern of airstrikes and artillery shelling targeting the 8 Syria: Salafi-Jihadist group Ahrar opposition-held Eastern Ghouta suburbs of Al-Hasakah a-Sham merged with Islamist group Damascus, killing at least 250 civilians. -

REGIONAL ANALYSIS SYRIA Received Little Or No Humanitarian Assistance in More Than 10 Months
currently estimated to be living in hard to reach or besieged areas, having REGIONAL ANALYSIS SYRIA received little or no humanitarian assistance in more than 10 months. 07 February 2014 Humanitarian conditions in Yarmouk camp continued to worsen with 70 reported deaths in the last 4 months due to the shortage of food and medical supplies. Local negotiations succeeded in facilitating limited amounts of humanitarian Part I – Syria assistance to besieged areas, including Yarmouk, Modamiyet Elsham and Content Part I Barzeh neighbourhoods in Damascus although the aid provided was deeply This Regional Analysis of the Syria conflict (RAS) is an update of the December RAS and seeks to Overview inadequate. How to use the RAS? bring together information from all sources in the The spread of polio remains a major concern. Since first confirmed in October region and provide holistic analysis of the overall Possible developments Syria crisis. In addition, this report highlights the Map - Latest developments 2013, a total of 93 polio cases have been reported; the most recent case in Al key humanitarian developments in 2013. While Key events 2013 Hasakeh in January. In January 2014 1.2 million children across Aleppo, Al Part I focuses on the situation within Syria, Part II Information gaps and data limitations Hasakeh, Ar-Raqqa, Deir-ez-Zor, Hama, Idleb and Lattakia were vaccinated covers the impact of the crisis on neighbouring Operational constraints achieving an estimated 88% coverage. The overall health situation is one of the countries. More information on how to use this Humanitarian profile document can be found on page 2. -
Weekly Conflict Summary | 3 – 9 June 2019
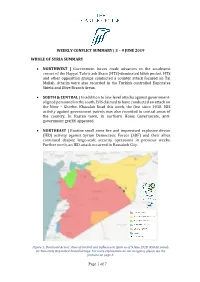
WEEKLY CONFLICT SUMMARY | 3 – 9 JUNE 2019 WHOLE OF SYRIA SUMMARY • NORTHWEST | Government forces made advances in the southwest corner of the Hayyat Tahrir ash Sham (HTS)-dominated Idleb pocket. HTS and other opposition groups conducted a counter attack focused on Tal Mallah. Attacks were also recorded in the Turkish-controlled Euphrates Shield and Olive Branch Areas. • SOUTH & CENTRAL | In addition to low-level attacks against government- aligned personnel in the south, ISIS claimed to have conducted an attack on the Nimr – Gherbet Khazalah Road this week, the first since 2018. ISIS activity against government patrols was also recorded in central areas of the country. In Rastan town, in northern Homs Governorate, anti- government graffiti appeared. • NORTHEAST | Routine small arms fire and improvised explosive device (IED) activity against Syrian Democratic Forces (SDF) and their allies continued despite large-scale security operations in previous weeks. Further north, an IED attack occurred in Hassakeh City. Figure 1: Dominant Actors’ Area of Control and Influence in Syria as of 9 June 2019. NSOAG stands for Non-state Organized Armed Groups. For more explanation on our mapping, please see the footnote on page 2. Page 1 of 7 WEEKLY CONFLICT SUMMARY | 3 – 9 JUNE 2019 NORTHWEST SYRIA1 This week, Government of Syria (GOS) forces made advances in the southwest corner of the Hayyat Tahrir ash Sham (HTS)-dominated Idleb enclave. On 3 June, GOS Tiger Forces captured al Qasabieyh town to the north of Kafr Nabuda, before turning west and taking Qurutiyah village a day later. Currently, fighting is concentrated around Qirouta village. However, late on 5 June, HTS and the Turkish-Backed National Liberation Front (NLF) launched a major counter offensive south of Kurnaz town after an IED detonated at a fortified government location. -
Monthly Every 2 Months Yearly
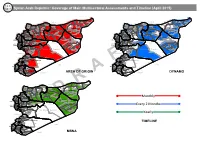
Syrian Arab Republic: Coverage of Main Multisectoral Assessments and Timeline (April 2015) Al-Malikeyyeh Al-Malikeyyeh Turkey Turkey Quamishli Quamishli Jarablus Jarablus Ras Al Ain Ras Al Ain Afrin Ain Al Arab Afrin Ain Al Arab Azaz Tell Abiad Azaz Tell Abiad Al-Hasakeh Al Bab Al-Hasakeh Al Bab Al-Hasakeh Al-Hasakeh Harim Harim Jebel Saman Ar-Raqqa Jebel Saman Ar-Raqqa Menbij Menbij Aleppo Aleppo Ar-Raqqa Idleb Ar-Raqqa Idleb Jisr-Ash-Shugur Jisr-Ash-Shugur As-Safira Ariha As-Safira Lattakia Ariha Ath-Thawrah Lattakia Ath-Thawrah Al-Haffa Idleb Al-Haffa Idleb Deir-ez-Zor Al Mara Deir-ez-Zor Al-Qardaha Al Mara Al-Qardaha As-Suqaylabiyah Deir-ez-Zor Lattakia As-Suqaylabiyah Deir-ez-Zor Lattakia Jablah Jablah Muhradah Muhradah As-Salamiyeh As-Salamiyeh Hama Hama Banyas Banyas Hama Sheikh Badr Masyaf Hama Sheikh Badr Masyaf Tartous Tartous Dreikish Al Mayadin Dreikish Ar-Rastan Al Mayadin Ar-Rastan Tartous TartousSafita Al Makhrim Safita Al Makhrim Tall Kalakh Tall Kalakh Homs Syrian Arab Republic Homs Syrian Arab Republic Al-Qusayr Al-Qusayr Abu Kamal Abu Kamal Tadmor Tadmor Homs Homs Lebanon Lebanon An Nabk An Nabk Yabroud Yabroud Al Qutayfah Al Qutayfah Az-Zabdani Az-Zabdani At Tall At Tall Rural Damascus Rural Damascus Rural Damascus Rural Damascus Damascus Damascus Darayya Darayya Duma Duma Qatana Qatana Rural Damascus Rural Damascus IraqIraq IraqIraq Quneitra As-Sanamayn Quneitra As-Sanamayn Dar'a Quneitra Dar'a Quneitra Shahba Shahba Al Fiq Izra Al Fiq Izra As-Sweida As-Sweida As-Sweida As-Sweida Dara Jordan AREA OF ORIGIN Dara Jordan -

UK Home Office
Country Policy and Information Note Syria: the Syrian Civil War Version 4.0 August 2020 Preface Purpose This note provides country of origin information (COI) and analysis of COI for use by Home Office decision makers handling particular types of protection and human rights claims (as set out in the Introduction section). It is not intended to be an exhaustive survey of a particular subject or theme. It is split into two main sections: (1) analysis and assessment of COI and other evidence; and (2) COI. These are explained in more detail below. Assessment This section analyses the evidence relevant to this note – i.e. the COI section; refugee/human rights laws and policies; and applicable caselaw – by describing this and its inter-relationships, and provides an assessment of, in general, whether one or more of the following applies: x A person is reasonably likely to face a real risk of persecution or serious harm x The general humanitarian situation is so severe as to breach Article 15(b) of European Council Directive 2004/83/EC (the Qualification Directive) / Article 3 of the European Convention on Human Rights as transposed in paragraph 339C and 339CA(iii) of the Immigration Rules x The security situation presents a real risk to a civilian’s life or person such that it would breach Article 15(c) of the Qualification Directive as transposed in paragraph 339C and 339CA(iv) of the Immigration Rules x A person is able to obtain protection from the state (or quasi state bodies) x A person is reasonably able to relocate within a country or territory x A claim is likely to justify granting asylum, humanitarian protection or other form of leave, and x If a claim is refused, it is likely or unlikely to be certifiable as ‘clearly unfounded’ under section 94 of the Nationality, Immigration and Asylum Act 2002. -
In PDF Format, Please Click Here
Deprivatio of Existence The use of Disguised Legalization as a Policy to Seize Property by Successive Governments of Syria A special report sheds light on discrimination projects aiming at radical demographic changes in areas historically populated by Kurds Acknowledgment and Gratitude The present report is the result of a joint cooperation that extended from 2018’s second half until August 2020, and it could not have been produced without the invaluable assistance of witnesses and victims who had the courage to provide us with official doc- uments proving ownership of their seized property. This report is to be added to researches, books, articles and efforts made to address the subject therein over the past decades, by Syrian/Kurdish human rights organizations, Deprivatio of Existence individuals, male and female researchers and parties of the Kurdish movement in Syria. Syrians for Truth and Justice (STJ) would like to thank all researchers who contributed to documenting and recording testimonies together with the editors who worked hard to produce this first edition, which is open for amendments and updates if new credible information is made available. To give feedback or send corrections or any additional documents supporting any part of this report, please contact us on [email protected] About Syrians for Truth and Justice (STJ) STJ started as a humble project to tell the stories of Syrians experiencing enforced disap- pearances and torture, it grew into an established organization committed to unveiling human rights violations of all sorts committed by all parties to the conflict. Convinced that the diversity that has historically defined Syria is a wealth, our team of researchers and volunteers works with dedication at uncovering human rights violations committed in Syria, regardless of their perpetrator and victims, in order to promote inclusiveness and ensure that all Syrians are represented, and their rights fulfilled. -
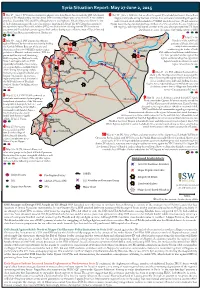
SYR SITREP Map May 27-June 2 2015
Syria Situation Report: May 27-June 2, 2015 1 May 27 – June 1: YPG forces continued to advance west from Ras al-Ayn towards the ISIS-held border 6 May 29 – June 2: ISIS launched an oensive against JN and rebel positions in the northern crossing of Tel Abyad, seizing over two dozen ISIS-controlled villages with support from U.S.-led coalition Aleppo countryside, seizing the town of Soran Azaz and several surrounding villages in a airstrikes. Meanwhile, YPG and FSA-aliated rebels in the Euphrates Volcano Operations Room in Ayn multi-pronged attack which included an SVBIED attack. In response, JN and numerous al-Arab canton announced the start of an oensive targeting Tel Abyad. e YPG denied accusations by Aleppo-based rebel groups deployed large numbers of reinforcements to the area. Clashes are the opposition Syrian National Coalition (SNC) and local activists claiming that the YPG conducted still ongoing amidst reported regime airstrikes in the area, which prompted the U.S. State executions and forced displacements against Arab civilians during recent oensives west of Ras al-Ayn and Department to accuse the regime of providing support to ISIS. on Abdul Aziz Mountain southwest of Hasaka city. Qamishli 7 May 27 – 30: 2 May 30 – June 2: ISIS launched an oensive Ayn al-Arab Residents of the rebel-held Ras al-Ayn against Hasaka City from three axes, heavily shelling 6 portions of Dera’a City held the Kawkab Military Base east of the city and 1 multiple demonstrations detonating at least two SVBIEDs against regime 10 Hasakah condemning the leaders of both FSA-aliated and Islamist rebel factions positions in Hasaka’s southern outskirts. -
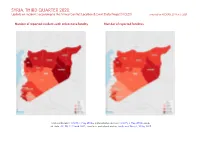
SYRIA, THIRD QUARTER 2020: Update on Incidents According to the Armed Conflict Location & Event Data Project (ACLED) Compiled by ACCORD, 25 March 2021
SYRIA, THIRD QUARTER 2020: Update on incidents according to the Armed Conflict Location & Event Data Project (ACLED) compiled by ACCORD, 25 March 2021 Number of reported incidents with at least one fatality Number of reported fatalities National borders: GADM, 6 May 2018a; administrative divisions: GADM, 6 May 2018b; incid- ent data: ACLED, 12 March 2021; coastlines and inland waters: Smith and Wessel, 1 May 2015 SYRIA, THIRD QUARTER 2020: UPDATE ON INCIDENTS ACCORDING TO THE ARMED CONFLICT LOCATION & EVENT DATA PROJECT (ACLED) COMPILED BY ACCORD, 25 MARCH 2021 Contents Conflict incidents by category Number of Number of reported fatalities 1 Number of Number of Category incidents with at incidents fatalities Number of reported incidents with at least one fatality 1 least one fatality Explosions / Remote Conflict incidents by category 2 1439 241 633 violence Development of conflict incidents from September 2018 to September Battles 543 232 747 2020 2 Violence against civilians 400 209 262 Strategic developments 394 0 0 Methodology 3 Protests 107 0 0 Conflict incidents per province 4 Riots 12 1 2 Localization of conflict incidents 4 Total 2895 683 1644 This table is based on data from ACLED (datasets used: ACLED, 12 March 2021). Disclaimer 7 Development of conflict incidents from September 2018 to September 2020 This graph is based on data from ACLED (datasets used: ACLED, 12 March 2021). 2 SYRIA, THIRD QUARTER 2020: UPDATE ON INCIDENTS ACCORDING TO THE ARMED CONFLICT LOCATION & EVENT DATA PROJECT (ACLED) COMPILED BY ACCORD, 25 MARCH 2021 Methodology GADM. Incidents that could not be located are ignored. The numbers included in this overview might therefore differ from the original ACLED data. -
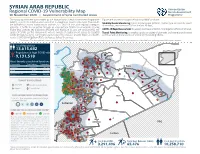
COVID Vulnerability October.Indd
SYRIAN ARAB REPUBLIC Humanitarian Regional COVID-19 Vulnerability Map Needs Assessment 10 November 2020 | Government of Syria Controlled Areas Programme The following factsheet was created by the Humanitarian Needs Assessment Programme Figures are sourced through the following HNAP products: (HNAP), a joint UN ini� a� ve which monitors humanitarian needs inside Syria. The results Mobility Needs Monitoring: tracks displacement pa� erns, shelter type and priority needs are intended to inform humanitarian partners on COVID-19 risks and regional contagion of residents, returnees and IDPs in the last 30 days; poten� al. It fulfi lls this objec� ve through an inter-sectoral COVID-19 vulnerability scoring matrix that assesses key indicators affi liated with exposure to, and are conducive to, the COVID-19 Rapid Assessment: bi-weekly overview of COVID-19 mi� ga� on eff orts at SD level; spread of COVID-19. The components include: burden of displacement, access to essen� al Transit Point Monitoring: bi-weekly update on status of domes� c and interna� onal transit COVID-19 hygiene items, community awareness of the disease, priority WASH and health points as well as the presence of COVID-19 monitoring eff orts. needs, COVID-19 mi� ga� on eff orts and access to health services. Turkey Disclaimer: The boundaries, areas, names and the designati ons used in this report do not imply offi cial endorsement or acceptance. Detailed methodology available upon request. Total Population 13,615,682 Population at high COVID risk Turkey 9,131,518 Al-Hasakeh Aleppo Most -

Turkey and Russia in Syrian War: Hostile Friendship
https://securityandefence.pl/ Turkey and Russia in Syrian war: Hostile friendship Cemil Doğaç İpek1, Mehmet Çağatay Güler2 [email protected] https://orcid.org/0000-0001-5007-7151 1Turkish National Defense University, Konaklar, Org. İzzettin Aksalur Cd., 34334 Beşiktaş/İstanbul/Turkey [email protected] https://orcid.org/0000-0001-8604-0449 2Bilkent University, Üniversiteler, 06800 Çankaya/Ankara, Turkey Abstract This study considers Russian-Turkish relations within the context of the Syrian war. We elaborate on both Russia’s and Turkey’s strategies and their understanding of the Syrian War, and consider how the two countries have managed to stay on the same page despite conflic- tual strategies and geopolitical interests in Syria. The current literature does not address this question and does not thoroughly compare their actions and engagements in the field. This article aims to clarify Turkey-Russia relations in the Syria and provides evidence of how they are in conflict and cooperate at the same time. In this regard, it is argued that the available evidence indicates that Turkey-Russia relations in Syria operate on the “compartmentalisation” strategy. In order to test this argument, the qualitative research method based on secondary resources is used while the theoretical framework previously formulated by Onis and Yilmaz (2015) is adopted. They conceptualise Turkey-Russia relations as if they do “compartmentalise economic issues and geopolitical rivalries in order to avoid the negative spillover of certain disagreements into areas of bilateral cooperation.” Furthermore, they claim that compartmentalisation can be hindered if there are deepening security concerns in an area like Syria. However, this article underscores that compartmentalisation does not only work by separating the economic issue from geopolitical rivalries; it also makes Turkey and Russia able to cooperate and conflict in a specific and fundamentally conflictual geopolitical issue such as Syria. -

From Daraa to Damascus: Regional and Temporal Protest Variation in Syria
From Daraa to Damascus: Regional and Temporal Protest Variation in Syria by Shena L. Cavallo B.A. International Relations and Spanish, Duquesne University, 2007 Submitted to the Graduate Faculty of The Graduate School of Public and International Affairs in partial fulfillment of the requirements for the degree of M.A International Development University of Pittsburgh 2012 UNIVERSITY OF PITTSBURGH Graduate School of Public and International Affairs This thesis was presented by Shena L. Cavallo It was defended on May 23, 2012 and approved by M. Müge Kokten-Finkel, PhD, Assistant Professor Ilia Murtazashvili, PhD, Assistant Professor Paul J. Nelson, PhD, Associate Professor Thesis Director: Luke N. Condra, PhD, Assistant Professor ii Copyright © by Shena L. Cavallo 2012 iii From Daraa to Damascus: Regional and Temporal Protest Variation in Syria Shena Cavallo, MID University of Pittsburgh, 2012 When protest erupted in Syria on March 2011, there was considerable analysis seeking to explain the initial display of collective action. While this initial showing of dissent caught some off-guard, what was more remarkable is how the protest movement managed to endure, well over a year, despite policies of severe repression, a lack of established opposition organizations, and a lack of regime defections. This paper seeks to explore which factors have sustained the protest movement, as well as the role of these factors at different stages in the ‘protest wave’ and the relationship these variables share with region- specific waves of protest. I hypothesize that more traditional approaches to understanding protest longevity must be expanded in order to help explain contemporary events of protest, particularly in authoritarian contexts. -

Syrian Arab Republic
NEEDS & POPULATION MONITORING REPORT POPULATION BASELINE ROUND IV OCTOBER 2015 © NPM Lattakia team SYRIAN ARAB REPUBLIC Needs and Population Monitoring (NPM), Round IV, October 2015 Contents 1. Background ............................................................................................................................... 3 2. Methodology ............................................................................................................................. 3 2.1 Classification of Target Population ............................................................................................................................ 4 2.2 Limitations .................................................................................................................................................................. 5 3. Brief information on round IV (October 2015) ..................................................................... 6 4. Key findings .............................................................................................................................. 7 5. Coverage ................................................................................................................................... 8 6. Overview of target population categories by demographics ............................................. 8 6.1 Present population categories in assessed communities ......................................................................................... 9 6.1.1 IDPs ....................................................................................................................................................................