Low Dose Combinations in the Treatment of Hypertension: Theory and Practice
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Shilluk Lexicography with Audio Data Bert Remijsen, Otto Gwado Ayoker & Amy Martin
Shilluk Lexicography With Audio Data Bert Remijsen, Otto Gwado Ayoker & Amy Martin Description This archive represents a resource on the lexicon of Shilluk, a Nilo-Saharan language spoken in South Sudan. It includes a table of 2530 lexicographic items, plus 10082 sound clips. The table is included in pdf and MS Word formats; the sound clips are in wav format (recorded with Shure SM10A headset mounted microphone and and Marantz PMD 660/661 solid state recorder, at a sampling frequency of 48kHz and a bit depth of 16). For each entry, we present: (a) the entry form (different for each word class, as explained below); (b) the orthographic representation of the entry form; (c) the paradigm forms and/or example(s); and (d) a description of the meaning. This collection was built up from 2013 onwards. The majority of entries were added between 2015 and 2018, in the context of the project “A descriptive analysis of the Shilluk language”, funded by the Leverhulme Trust (RPG-2015- 055). The main two methods through which the collection was built up are focused lexicography collection by semantic domain, whereby we would collect e.g. words relating to dwellings / fishing / etc., and text collection, whereby we would add entries as we came across new words in the course of the analysis of narrative text. We also added some words on the basis of two earlier lexicographic studies on Shilluk: Heasty (1974) and Ayoker & Kur (2016). We estimate that we drew a few hundred words from each. Comparing the lexicography resource presented here with these two resources, our main contribution is detail, in that we present information on the phonological form and on the grammatical paradigm. -

A Grammar of Umbeyajts As Spoken by the Ikojts People of San Dionisio Del Mar, Oaxaca, Mexico
ResearchOnline@JCU This file is part of the following reference: Salminen, Mikko Benjamin (2016) A grammar of Umbeyajts as spoken by the Ikojts people of San Dionisio del Mar, Oaxaca, Mexico. PhD thesis, James Cook University. Access to this file is available from: http://researchonline.jcu.edu.au/50066/ The author has certified to JCU that they have made a reasonable effort to gain permission and acknowledge the owner of any third party copyright material included in this document. If you believe that this is not the case, please contact [email protected] and quote http://researchonline.jcu.edu.au/50066/ A Grammar of Umbeyajts as spoken by the Ikojts people of San Dionisio del Mar, Oaxaca, Mexico Mikko Benjamin Salminen, MA A thesis submitted to James Cook University, Cairns In fulfillment of the requirements for the degree of Doctor of Philosophy Language and Culture Research Centre, Cairns Institute College of Arts, Society and Education - James Cook University October 2016 Copyright Care has been taken to avoid the infringement of anyone’s copyrights and to ensure the appropriate attributions of all reproduced materials in this work. Any copyright owner who believes their rights might have been infringed upon are kindly requested to contact the author by e-mail at [email protected]. The research presented and reported in this thesis was conducted in accordance with the National Health and Medical Research Council (NHMRC) National Statement on Ethical Conduct in Human Research, 2007. The proposed research study received human ethics approval from the JCU Human Research Ethics Committee Approval Number H4268. -

Conventions and Abbreviations
Conventions and abbreviations Example sentences consist of four lines. The first line uses a practical orthography. The second line shows the underlying morphemes. The third line is a gloss, and the fourth line provides a free translation in English. In glosses, proper names are represented by initials. Constituents are in square brackets. Examples are numbered separately for each chapter. If elements are marked in other ways (e.g. with boldface), this is indicated where relevant. A source reference is given for each example; the reference code consists of the initials of the speaker (or ‘Game’ for the Man and Tree games), the date the recording was made, and the number of the utterance. An overview of recordings plus reference codes can be found in Appendix I. The following abbreviations and symbols are used in glosses: 1 first person 2 second person 3 third person ADJ adjectiviser ANIM animate APPL applicative CAUS causative CLF classifier CNTF counterfactual COMP complementiser COND conditional CONT continuative DEF definiteness marker DEM demonstrative DIM diminutive DIST distal du dual EMP emphatic marker EXCL exclusive FREE free pronoun FOC focus marker HAB habitual IMP imperative INANIM inanimate INCL inclusive INT intermediate INTJ interjection INTF intensifier IPFV imperfective IRR irrealis MOD modal operator NEG negation marker NOM nominaliser NS non-singular PART partitive https://doi.org/10.1515/9783110675177-206 XXIV Conventions and abbreviations pc paucal PERT pertensive PFV perfective pl plural POSS possessive PRF perfect PROG progressive PROX proximate RECIP reciprocal REDUP reduplication REL relative clause marker sg singular SPEC.COLL specific collective SUB subordinate clause marker TAG tag question marker ZERO person/number reference with no overt realisation - affix boundary = clitic boundary . -

Possessive Constructions in Tongugbe, an Ewe Dialect Promise Dodzi Kpoglu
Possessive constructions in Tongugbe, an Ewe dialect Promise Dodzi Kpoglu To cite this version: Promise Dodzi Kpoglu. Possessive constructions in Tongugbe, an Ewe dialect. Linguistics. Université de Lille; Universiteit Leiden (Leyde, Pays-Bas), 2019. English. NNT : 2019LILUH003. tel-02453932 HAL Id: tel-02453932 https://tel.archives-ouvertes.fr/tel-02453932 Submitted on 24 Jan 2020 HAL is a multi-disciplinary open access L’archive ouverte pluridisciplinaire HAL, est archive for the deposit and dissemination of sci- destinée au dépôt et à la diffusion de documents entific research documents, whether they are pub- scientifiques de niveau recherche, publiés ou non, lished or not. The documents may come from émanant des établissements d’enseignement et de teaching and research institutions in France or recherche français ou étrangers, des laboratoires abroad, or from public or private research centers. publics ou privés. UNIVERSITÉ DE LILLE CONSTRUCTIONS POSSESSIVES EN TONGUGBE, UN DIALECTE DE L'ÉWÉ POSSESSIVE CONSTRUCTIONS IN TONGUGBE, AN EWE DIALECT Promise DODZI KPOGLU Soutenue le 28 Février 2019 Directeurs de thèse: Prof.dr. A. Carlier (Université de Lille, Lille) Prof.dr. M.P.G.M. Mous (Université de Leyde, Leyde) Co-encadrant: Dr. F.K. Ameka (Université de Leyde, Leyde) Membres du jury: Prof.emer. D. Creissels (Université Lumière, Lyon) Prof.dr. M. Vanhove (Inalco & LLACAN CNRS, Paris) Prof.dr. J.E.C.V. Rooryck (Université de Leyde, Leyde), Président Dr. P.K. Agbedor (Central University, Accra) Dr. C. Patin (Université de Lille, Lille) POSSESSIVE CONSTRUCTIONS IN TONGUGBE, AN EWE DIALECT Possessive constructions in Tongugbe, an Ewe dialect Proefschrift ter verkrijging van de graad van Doctor aan de Universiteit Leiden, op gezag van Rector Magnificus prof.mr. -

Effect of Exogenous Glucocorticoid on Osmotically Stimulated Antidiuretic
European Journal of Endocrinology (2006) 155 845–848 ISSN 0804-4643 CLINICAL STUDY Effect of exogenous glucocorticoid on osmotically stimulated antidiuretic hormone secretion and on water reabsorption in man Volker Ba¨hr1, Norma Franzen1, Wolfgang Oelkers2, Andreas F H Pfeiffer1 and Sven Diederich1,2 1Department of Endocrinology, Diabetes and Nutrition, Charite-Universitatsmedizin Berlin, Campus Benjamin Franklin, Hindenburgdamm 30, 12200 Berlin, Germany and 2Endokrinologikum Berlin, Centre for Endocrine and Metabolic Diseases, Berlin, Germany (Correspondence should be addressed to V Ba¨hr; Email: [email protected]) Abstract Objective: Glucocorticoids exert tonic suppression of antidiuretic hormone (ADH) secretion. Hypocortisolism in secondary adrenocortical insufficiency can result in a clinical picture similar to the syndrome of inappropriate ADH secretion. On the other hand, in vitro and in vivo results provide evidence for ADH suppression in states of hypercortisolism. To test the hypothesis that ADH suppression is of relevance during glucocorticoid therapy, we investigated the influence of prednisolone on the osmotic stimulation of ADH. Design and methods: Seven healthy men were subjected to water deprivation tests with the measurement of plasma ADH (pADH) and osmolality (posmol) before and after glucocorticoid treatment (5 days 30 mg prednisolone per day). Results: Before glucocorticoid treatment, the volunteers showed a normal test with an adequate increase of pADH (basal 0.54G0.2 to 1.9G0.72 pg/ml (meanGS.D.)) in relation to posmol(basal 283.3G8.5 to 293.7G6 mosmol/kg). After prednisolone intake, pADH was attenuated (!0.4 pg/ml) in spite of an increase of posmol from 289.3G3.6 to 297.0G5.5 mosmol/kg. -

Beta-Blockers for Hypertension: Time to Call a Halt
Journal of Human Hypertension (1998) 12, 807–810 1998 Stockton Press. All rights reserved 0950-9240/98 $12.00 http://www.stockton-press.co.uk/jhh FOR DEBATE Beta-blockers for hypertension: time to call a halt DG Beevers University Department of Medicine, City Hospital, Birmingham B18 7QH, UK Beta-blockers are not very effective at lowering blood the endorsement of beta-blockers by the British Hyper- pressure in elderly hypertensive patients or in Afro- tension Society and other guidelines committees, Caribbeans and these two groups represent a large pro- except possibly for severe resistant hypertension, high portion of people with raised blood pressure. Further- risk post-infarct patients and those with angina pectoris. more they do not prevent more heart attacks than the The time has come to move across to newer, safer, more thiazide diuretics. Beta-blockers can also be dangerous tolerable and more effective antihypertensive agents in many hypertensive patients and even when these whilst continuing to use thiazide diuretics in low doses drugs are not contraindicated, they cause subtle and in the elderly as first choice, providing there are no depressing side effects which should preclude their contraindications. usefulness. The time has come therefore to reconsider Keywords: beta-blockers; hypertension Introduction Safety and tolerability Beta-adrenergic blockers were first introduced in the There is little doubt that the beta-blockers are the early 1960s for the treatment of angina pectoris. most unsafe of all antihypertensive drugs. They can Their antihypertensive properties were not fully precipitate or worsen heart failure in patients with recognised until the celebrated paper by Pritchard myocardial damage and they are contraindicated in and Gillam in 1964.1 They rapidly became popular patients with asthma. -

REVIEWS Possession and Ownership
REVIEWS Possession and ownership: A cross-linguistic typology. Ed. by Alexandra Y. Aikhenvald and R. M. W. Dixon . (Explorations in linguistic typology.) Oxford: Oxford University Press, 2013. Pp. xxii, 319. ISBN 9780199660223. $125 (Hb). Reviewed by Lars Johanson , Johannes Gutenberg-Universität Mainz This collection of essays about possession and ownership aims at combining linguistic and an - thropological concepts concerning the relation between language, culture, and modes of thinking, particularly the ways in which culture and cognition are manifested in grammar. Alexandra Y. Aikhenvald’s opening essay, ‘Possession and ownership: A cross-linguistic perspective’, is a lucid introduction that defines, explains, and exemplifies all conceivable aspects of the topic. Chs. 2–11 address the ways that linguistic structures reflect cultural patterns, attitudes toward possession, and effects of change. Isabelle Bril analyzes the complex system of ownership re - lations in the Oceanic language Nêlêmwa of New Caledonia. Gloria J. Gravelle investigates patterns of possession in Moskona, an East Bird’s Head language of West Papua, Indonesia. Alexandra Y. Aikhenvald deals with possession and ownership in Manambu, a Ndu language of the Sepik area of Papua New Guinea. Alan Dench analyzes possession in Martuthunira, once spoken in the Pilbara region of Western Australia. Lev Michael discusses Nanti, spoken in Peru, in the context of other Arawak languages. Mark W. Post deals with possession and association in the Tibeto-Burman Galo language and its culture. Yongxian Luo examines possessive con - structions in Mandarin Chinese. Anne Storch studies possession in Hone, a Jukonoid language Felix K. Ameka of Nigeria. deals with possessive constructions in Likpe (S ɛkp ɛlé), a Kwa lan - guage of Ghana. -
Initiation Titration Assess Monitoring **
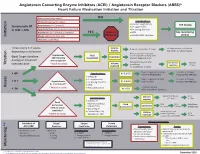
Angiotensin Converting Enzyme Inhibitors (ACEI) / Angiotensin Receptor Blockers (ARBS)* Heart Failure Medication Initiation and Titration Bilateral renal artery stenosis NO Moderate/Severe aortic stenosis Considerations: • Baseline cough (ACEi) Hyperkalemia: K+ > 5.2 mmol/L See dosing Symptomatic HF • K+ supplements or LVEF < 40% Renal Dysfunction:Serum creatinine >220 µmol/L • K+ sparing diuretics Hypotension: SBP < 90 mmHg or symptoms YES Refer to • MRA See monitoring Initiation Allergy: angioedema, hives, rash Physician • NSAIDS/COX2 inhibitors section Intolerance: cough (ACEi) Titrate every 1-3 weeks, Volume Reduce/hold diuretic x 2-3 days No improvement, hold/reduce depending on tolerance deplete ACEI/ARB x 1-2 wks & reassess Reassess diuretic dose/other Hypotension Fluid non-essential BP lowering meds Goal: Target dose(see Euvolemic SBP<90mmHg Assessment Consider staggering doses dosing) or maximum with symptoms* Reduce/hold dose of other See Diuretic Reassess Titration * Watch for trends Volume tolerated dose vasodilators algorithm 1-2 wks overload +/- ACEI/ARB x 1-2 weeks Stop K+ supplements, reduce/ Serum K+ in 3-5 days, Considerations: • BP K+ 5.2-5.5 hold MRA (if applicable) Reassess ACEI/ARB dose • Dietary K+ • K+ supplements Stop K+ supplements, MRA. Serum K+ in 2-3 days, • K + Hyperkalemia • K+ sparing diuretics K+ 5.6-6.0 hold ACEI/ARB Reassess ACEI/ARB dose K+ > 5.2 mmol/L* • MRA Assess * Watch for trends • Renal dysfunction Treat hyperkalemia • Scr K+ > 6.0 Refer to MD/NP +/- send to ED Reduce/hold diuretic Scr in Considerations: -

Atypology of Marked-S Languages
A typology of marked-S languages Corinna Handschuh language Studies in Diversity Linguistics, No 1 science press Studies in Diversity Linguistics Chief Editor: Martin Haspelmath Consulting Editors: Fernando Zúñiga, Peter Arkadiev, Ruth Singer, Pilar Valen zuela In this series: 1. Handschuh, Corinna. A typology of marked-S languages 2. Rießler, Michael. Adjective attribution 3. Klamer, Marian (ed.). The Alor-Pantar languages: History and typology 4. Berghäll, Liisa. A grammar of Mauwake (Papua New Guinea) A typology of marked-S languages Corinna Handschuh language science press Language Science Press Berlin Language Science Press Habelschwerdter Allee 45 14195 Berlin, Germany langsci-press.org This title can be downloaded at: http://langsci-press.org/catalog/book/18 © 2014, Corinna Handschuh Published under the Creative Commons Attribution 4.0 Licence (CC BY 4.0): http://creativecommons.org/licenses/by/4.0/ ISBN: 978-3-944675-19-0 Cover and concept of design: Ulrike Harbort Typesetting: Corinna Handschuh Proofreading: Eitan Grossman, Daniel W. Hieber, Aaron Sonnenschein Storage and cataloguing done by FU Berlin Language Science Press has no responsibility for the persistence or accuracy of URLs for external or third-party Internet websites referred to in this publication, and does not guarantee that any content on such websites is, or will remain, ac- curate or appropriate. Information regarding prices, travel timetables and other factual information given in this work are correct at the time of first publication but Language Science Press does not guarantee the accuracy of such information thereafter. Für Tommeck Contents Acknowledgments ix List of abbreviations xi I Preliminaries 1 1 Introduction 3 1.1 Marked-S coding .......................... -

Energy Drinks 800.232.4424 (Voice/TTY) 860.793.9813 (Fax)
Caffeine and Energy Boosting Drugs: Energy Drinks 800.232.4424 (Voice/TTY) 860.793.9813 (Fax) www.ctclearinghouse.org A Library and Resource Center on Alcohol, Tobacco, Other Drugs, Mental Health and Wellness What are energy drinks? you. You wouldn't use Mountain Dew as a sports Energy drinks are beverages like drink. And a drink like Red Bull and vodka is Red Bull, Venom, Adrenaline Rush, more like strong coffee and whisky than 180, ISO Sprint, and Whoopass, anything else. which contain large doses of caffeine and other legal stimulants What happens when energy drinks are like ephedrine, guarana, and ginseng. combined with alcohol? Energy drinks may contain as much as 80 mg. Energy drinks are also used as mixers with of caffeine, the equivalent of a cup of coffee. alcohol. This combination carries a number of Compared to the 37 mg. of caffeine in a dangers: Mountain Dew, or the 23 mg. in a Coca-Cola Classic, that's a big punch. These drinks are • Since energy drinks are stimulants and marketed to people under 30, especially to alcohol is a depressant, the combination of college students, and are widely available both effects may be dangerous. The stimulant on and off campus. effects can mask how intoxicated you are and prevent you from realizing how much Are there short-term dangers to drinking alcohol you have consumed. Fatigue is one energy drinks? of the ways the body normally tells Individual responses to caffeine vary, and someone that they've had enough to drink. these drinks should be treated carefully • The stimulant effect can give the person the because of how powerful they are. -

The Noun Phrase in Shilluk
Language Documentation & Conservation Special Publication No. 14 – A Grammar of Shilluk Chapter 5: The noun phrase by Bert Remijsen & Otto Gwado Ayoker http://hdl.handle.net/10125/24781 CHAPTER 5 The noun phrase in Shilluk Bert Remijsen & Otto Gwado Ayoker, University of Edinburgh Abstract • This chapter presents a descriptive analysis of the noun phrase in Shilluk, surveying the variety of modifiers that combine with a nominal head. For the sake of accountability, 270 sound clips are embedded, many of them drawn from spontaneous speech. The set of noun-phrase modifiers includes possessors, adjectives, verbs, non-possessor nouns, quantifiers (including numerals), determiners, and a diminuitive. Of all of these modifiers, the diminuitive is the only one that preceeds the head. This fits with the interpretation that the diminuitive represents an instance of grammaticalization, which developed out of a possessive noun phrase construction. Of particular interest in relation to the numeral system is the fact that, for numbers below 10, the cardinal is morphologically derived on the basis of the ordinal, rather than the way around. Also, in noun phrases modified by a verbal predicate, we find past tense marking on the modification marker. Noun phrases are conjoined in an asymmetric manner, with the non-initial noun phrase representing a prepositional phrase. We also describe vocatives and associative plurals, both of which involve morphological marking at the right edge of the noun phrase. As such, they stand out in the context of Shilluk morphology, which is primarily head-marking in nature. Licensed under Creative Commons Attribution Non-Commercial No Derivatives License ISBN 978-0-9973295-2-9 The noun phrase 2 1. -

Hypomnemata Glossopoetica
Hypomnemata Glossopoetica Wm S. Annis June 8, 2021 1. Phonology Normally illegal clusters may occur in particular grammatical contexts, and thus look common (cf. Latin -st in 3sg copula est). Hierarchy of codas:1 n < m, ɳ, ŋ < ɳ « l, ɹ < r, ʎ, ʁ < ɭ, ɽ « t < k, p < s, z, c, q, ʃ < b, d, g, x h « w, j. There is a slight place hierarchy: alveolar < velar < retroflex or tap. Classes percolate, such that in complex codas, if Nasals, Resonants and Stops are permitted you usually expect n, r, s, nr, ns and rs as coda sequences. Other orders are possible, but the above rule is common-ish. Hierarchy of clusters (s = sonorant, o = obstruent), word initial: os < oo < ss < so; word final: so < oo < ss < os. Onset clusters tend to avoid identical places of articulation, which leads to avoidance of things like *tl, dl, bw, etc., in a good number of languages. /j/ is lightly disfavored as c2 after dentals, alveolars and palatals; /j/ and palatals are in general disfavored before front vowels. Languages with sC- clusters often have codas. s+stop < s+fric / s+nasal < s+lat < s+rhot (the fricative and nasal are trickier to order). Even if a particular c is a permitted coda, its allowed environment may be quite restricted. Potential con- straints: forbidden before homorganic stop; or homorganic nasal; geminates forbidden. Solutions: delete with compensatory vowel lengthening; debuccalize (become fricative, glottal stop, delete without compensation); nasal deletion with nasalized vowel remaining; tone wackiness. Lower vowels are preferred as syllabic nuclei; high vowels are more prone to syncope (either midword or fi- nally).