Artemether-Lumefantrine (Six-Dose Regimen) for Treating Uncomplicated Falciparum Malaria (Review)
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

How to Protect Yourself Against Malaria 1 Fig
From our Whitepaper Files: How to > See companion document Protect Yourself Against Malaria World Malaria Risk Chart 2015 Edition Canada 67 Mowat Avenue, Suite 036 Toronto, Ontario M6K 3E3 (416) 652-0137 USA 1623 Military Road, #279 Niagara Falls, New York 14304-1745 (716) 754-4883 New Zealand 206 Papanui Road Christchurch 5 www.iamat.org | [email protected] | Twitter @IAMAT_Travel | Facebook IAMATHealth THE ENEMY area. Of the 460 Anopheles species, approximately 100 can transmit malaria Sunset — the hunt for human blood begins. parasites. From dusk to dawn the female Anopheles, Mosquitoes prey on a variety of hosts — the malaria-carrying mosquito searches for a host humans, monkeys, lizards, birds — carrying to supply her with blood. Blood is an absolute different species of malaria parasites which in necessity for her because it provides the protein turn infect only specific hosts. Of the approxi- needed for the development of her eggs which mately 50 different species of malaria parasites she later deposits in her breeding place. sharing the genetic name Plasmodium, only She has a tiny, elegant body, measuring 5 infect humans: Plasmodium falciparum, from 8 mm to 1 cm. She has dark spots on the killer; Plasmodium vivax; Plasmodium ovale, her wings, three pairs of long, slender legs and Plasmodium malariae and Plasmodium knowlesi. a prominent tubular proboscis with which The latter, a malaria parasite of Old World she draws blood. monkeys, has been identified to infect humans Fig. 1 Female Anopheles mosquito. The Anopheles enters your room at night. in Southeast Asia. In the past this parasite has Image source: World Health Organization You may recognize her by the way she rests been misdiagnosed as Plasmodium malariae. -

Hydroxychloroquine Or Chloroquine for Treating Coronavirus Disease 2019 (COVID-19) – a PROTOCOL for a Systematic Review of Individual Participant Data
Hydroxychloroquine or Chloroquine for treating Coronavirus Disease 2019 (COVID-19) – a PROTOCOL for a systematic review of Individual Participant Data Authors Fontes LE, Riera R, Miranda E, Oke J, Heneghan CJ, Aronson JK, Pacheco RL, Martimbianco ALC, Nunan D BACKGROUND In the face of the pandemic of SARS CoV2, urgent research is needed to test potential therapeutic agents against the disease. Reliable research shall inform clinical decision makers. Currently, there are several studies testing the efficacy and safety profiles of different pharmacological interventions. Among these drugs, we can cite antimalarial, antivirals, biological drugs, interferon, etc. As of 6 April 2020 there are three published reportsand 100 ongoing trials testing hydroxychloroquine/chloroquine alone or in association with other drugs for COVID-19. This prospective systematic review with Individual Participant data aims to assess the rigour of the best-available evidence for hydroxychloroquine or chloroquine as treatment for COVID-19 infection. The PICO framework is: P: adults with COVID-19 infection I: chloroquine or hydroxychloroquine (alone or in association) C: placebo, other active treatments, usual standard care without antimalarials O: efficacy and safety outcomes OBJECTIVES To assess the effects (benefits and harms) of chloroquine or hydroxychloroquine for the treatment of COVID-19 infection. METHODS Criteria for considering studies for this review Types of studies We shall include randomized controlled trials (RCTs) with a parallel design. We intend to include even small trials (<50 participants), facing the urgent need for evidence to respond to the current pandemic. Quasi-randomized, non-randomized, or observational studies will be excluded due to a higher risk of confounding and selection bias (1). -

Information for the User Riamet® 20 Mg/120 Mg Tablets Artemether And
Package leaflet: Information for the user Riamet® 20 mg/120 mg tablets artemether and lumefantrine Read all of this leaflet carefully before you start taking this medicine because it contains important information for you. - Keep this leaflet. You may need to read it again. - If you have any further questions, ask your doctor or pharmacist. - This medicine has been prescribed for you only. Do not pass it on to others. It may harm them, even if their signs of illness are the same as yours. - If you get any side effects, talk to your doctor or pharmacist. This includes any possible side effects not listed in this leaflet. (See section 4). What is in this leaflet 1. What Riamet is and what it is used for 2. What you need to know before you take Riamet 3. How to take Riamet 4. Possible side effects 5. How to store Riamet 6. Contents of the pack and other information 1. What Riamet is and what it is used for Riamet contains two substances called artemether and lumefantrine. They belong to a group of medicines called anti-malarials. Riamet is only used for the treatment of acute uncomplicated malaria infections caused by a parasite called “Plasmodium falciparum”. This parasite is a tiny organism made up of one cell that is found inside red blood cells. Riamet is used to treat adults, children and infants of 5 kg body weight and above. Riamet is not used to prevent malaria or to treat severe malaria (where it has affected the brain, lungs or kidneys). -
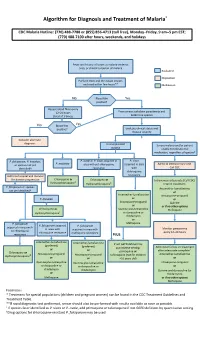
Algorithm for Diagnosis and Treatment of Malaria*
Algorithm for Diagnosis and Treatment of Malaria* CDC Malaria Hotline: (770) 488-7788 or (855) 856-4713 (toll free), Monday–Friday, 9 am–5 pm EST; (770) 488-7100 after hours, weekends, and holidays Fever and history of travel to malaria-endemic area, or clinical suspicion of malaria Evaluation Disposition Perform thick and thin blood smears and read within few hours** Medication No Blood film Yes positive? Repeat blood films every 12–24 hours From smear: calculate parasitemia and (total of 3 times) determine species No Blood film Yes positive? Evaluate clinical status and disease severity Consider alternate diagnosis Uncomplicated Severe malaria and/or patient malaria unable to tolerate oral medication, regardless of species† P. falciparum, P. knowlesi, P. ovale or P. vivax acquired in P. vivax P. malariae or species not yet area without chloroquine acquired in area Admit to intensive care unit. identified† resistance with Call CDC chloroquine Admit to hospital and monitor resistance for disease progression Chloroquine or Chloroquine or ‡ Intravenous artesunate (Call CDC) Hydroxychloroquine Hydroxychloroquine‡ Interim treatment: P. falciparum or species Artemether-lumefantrine not yet identified† or Artemether-lumefantrine Atovaquone-proguanil P. knowlesi or or Atovaquone-proguanil Quinine or or if no other options Chloroquine or Quinine plus tetracycline Mefloquine Hydroxychloroquine‡ or doxycycline or clindamycin or P. falciparum Mefloquine P. falciparum acquired P. falciparum acquired in area with in area with acquired in area with -

Artemether-Lumefantrine Compared to Atovaquone-Proguanil As a Treatment for Uncomplicated Plasmodium Falciparum Malaria in Travelers
Am. J. Trop. Med. Hyg., 92(1), 2015, pp. 13–17 doi:10.4269/ajtmh.14-0249 Copyright © 2015 by The American Society of Tropical Medicine and Hygiene Artemether-Lumefantrine Compared to Atovaquone-Proguanil as a Treatment for Uncomplicated Plasmodium falciparum Malaria in Travelers Shirly Grynberg, Tamar Lachish, Eran Kopel, Eyal Meltzer, and Eli Schwartz* The Center of Geographic Medicine and Tropical Diseases, Sheba Medical Center, Tel Hashomer, Israel; The Infectious Diseases Unit, Shaare-Zedek Medical Center, Jerusalem, Israel; The Sackler Faculty of Medicine, Tel Aviv University, Tel Aviv, Israel Abstract. Atovaquone-proguanil (AP) and artemether-lumefantrine (AL) are both treatments for uncomplicated Plasmodium falciparum malaria, but comparative clinical trials are lacking. We performed a retrospective analysis, comparing treatment failure and fever clearance time in non-immune travelers with uncomplicated P. falciparum malaria, treated with AP or AL. Sixty-nine patients were included during 2001–2013: 44 in the AP group and 25 in the AL group. Treatment failure was observed in 6 of 44 (13.6%) and 1 of 25 (4.0%) patients in the AP and AL groups, respectively. Six treatment failures were observed in travelers from West Africa. Fever clearance time was 44 ± 23 h in AL group versus 77 ± 28 h in AP group, (P < 0.001). Hospitalization time was significantly shorter in the AL group; 3.8 + 1.3 versus 5.1 + 2.8 days in the AP group (P = 0.04) In conclusion, travelers with uncomplicated P. falciparum malaria recover faster on AL than on AP. The AL should probably be the drug of choice for this population. -

Resistance to Antimalarial Drugs: Molecular, Pharmacologic, and Clinical Considerations
0031-3998/09/6505-0064R Vol. 65, No. 5, Pt 2, 2009 PEDIATRIC RESEARCH Printed in U.S.A. Copyright © 2009 International Pediatric Research Foundation, Inc. Resistance to Antimalarial Drugs: Molecular, Pharmacologic, and Clinical Considerations MARK A. TRAVASSOS AND MIRIAM K. LAUFER Center for Vaccine Development, University of Maryland School of Medicine, Baltimore, Maryland 21201 ABSTRACT: One of the greatest obstacles to the control of hematin, a toxic byproduct of Hb degradation, in the Plasmo- malaria has been the spread of resistance to drugs used on a large dium parasite’s food vacuole. Although it is no longer recom- scale. This review provides an update of the current understanding mended for the treatment of P. falciparum, it is the drug of of the molecular basis for antimalarial drug resistance. Parasite choice to treat P. vivax and P. ovale, less severe forms of intrinsic resistance is just one component that determines the in vivo efficacy of a drug. Human immune responses and pharmaco- malaria that can cause recurrent infections. logic properties play important roles in determining the clinical With the spread of chloroquine resistance, many countries outcome of treatment. The emergence and spread of resistance adopted SP as the first-line antimalarial treatment. SP is com- also results from an interplay of these factors. Current efforts to posed of two drugs that act on sequential enzymes in the folate characterize and deter resistance to new combination therapy are synthesis pathway. When both drugs are used together, they act also discussed. (Pediatr Res 65: 64R–70R, 2009) synergistically. Although SP is a coformulation of two drugs, it is not considered combination therapy because the mechanisms of ne of the greatest obstacles to the control of malaria has action are closely linked. -

(Artemether / Lumefantrine 20Mg/120 Mg) Tablets
SUMMARY OF PRODUCT CHARACTERISTICS Page 1 of 13 1. NAME OF THE MEDICINAL PRODUCT Lumartem (Artemether / Lumefantrine 20mg/120 mg) Tablets 2. QUALITATIVE AND QUANTITATIVE COMPOSITION Each tablet contains: 20 mg artemether and 120 mg lumefantrine. For a full list of excipients see section 6.1. 3. PHARMACEUTICAL FORM Yellow coloured, circular, uncoated, flat faced, bevelled edged, matt finished tablets with a break line on one side and plain on the other side. The scoreline is only to facilitate breaking for ease of swallowing and not to divide into equal doses. 4. CLINICAL PARTICULARS 4.1 Therapeutic indication Artemether 20 mg and Lumefantrine 120 mg Tablets is indicated for the treatment of uncomplicated cases of malaria due to Plasmodium falciparum in adults, children and infants of 5 kg and above. The most recent official guidelines on the appropriate use of antimalarial agents and local information on the prevalence of resistance to antimalarial drugs must be taken into consideration for deciding on the appropriateness of therapy with Artemether 20 mg and Lumefantrine 120 mg Tablets. Official guidance will normally include WHO (http://whqlibdoc.who.int/publications/2010/9789241547925_eng.pdf) and local health authorities’ guidelines (see also sections 4.4 and 5.1). 4.2 Posology and method of administration Tablets for oral administration. Page 2 of 13 Number of Artemether 20 mg and Lumefantrine 120 mg Tablets for treatment according to weight bands st nd rd Weight range 1 day of 2 day of 3 day treatment treatment of treatment ≥ 5kg -

Current Antimalarial Therapies and Advances in the Development of Semi-Synthetic Artemisinin Derivatives
Anais da Academia Brasileira de Ciências (2018) 90(1 Suppl. 2): 1251-1271 (Annals of the Brazilian Academy of Sciences) Printed version ISSN 0001-3765 / Online version ISSN 1678-2690 http://dx.doi.org/10.1590/0001-3765201820170830 www.scielo.br/aabc | www.fb.com/aabcjournal Current Antimalarial Therapies and Advances in the Development of Semi-Synthetic Artemisinin Derivatives LUIZ C.S. PINHEIRO1, LÍVIA M. FEITOSA1,2, FLÁVIA F. DA SILVEIRA1,2 and NUBIA BOECHAT1 1Fundação Oswaldo Cruz, Instituto de Tecnologia em Fármacos Farmanguinhos, Fiocruz, Departamento de Síntese de Fármacos, Rua Sizenando Nabuco, 100, Manguinhos, 21041-250 Rio de Janeiro, RJ, Brazil 2Universidade Federal do Rio de Janeiro, Programa de Pós-Graduação em Química, Avenida Athos da Silveira Ramos, 149, Cidade Universitária, 21941-909 Rio de Janeiro, RJ, Brazil Manuscript received on October 17, 2017; accepted for publication on December 18, 2017 ABSTRACT According to the World Health Organization, malaria remains one of the biggest public health problems in the world. The development of resistance is a current concern, mainly because the number of safe drugs for this disease is limited. Artemisinin-based combination therapy is recommended by the World Health Organization to prevent or delay the onset of resistance. Thus, the need to obtain new drugs makes artemisinin the most widely used scaffold to obtain synthetic compounds. This review describes the drugs based on artemisinin and its derivatives, including hybrid derivatives and dimers, trimers and tetramers that contain an endoperoxide bridge. This class of compounds is of extreme importance for the discovery of new drugs to treat malaria. Key words: malaria, Plasmodium falciparum, artemisinin, hybrid. -

Traveler Information
Traveler Information QUICK LINKS MALARIA—TRAVELER INFORMATION • Shoreland's Recommendations for Malaria Prevention • What's New • General Information • Symptoms • Disease Risk • Preventive Therapy • Timing of Antimalarial Drugs • Antimalarial Drugs • Pregnancy • Breastfeeding • Infants and Children • When to Seek Medical Attention • Self-Treatment of Presumptive Malaria Traveler Information MALARIA SHORELAND'S RECOMMENDATIONS FOR MALARIA PREVENTION Atovaquone/proguanil (Malarone), doxycycline, chloroquine, and mefloquine are equally effective antimalarial drugs when taken as instructed, as long as there is no resistance to the drug at the destination. In areas of chloroquine-resistant P. falciparum malaria, mefloquine, atovaquone/proguanil, and doxycycline are equally effective drug options. In areas of mefloquine resistance, either doxycycline or atovaquone/proguanil can be used. Another drug, primaquine, can be used in special cases but is not a first-choice drug for prevention. For short-term travelers (less than 2-3 weeks), atovaquone/proguanil may be preferable because travelers can stop taking the drug just 7 days after leaving the malarious area. Longer courses of atovaquone/proguanil appear safe but are more costly than mefloquine or doxycycline. For long-term travelers, mefloquine is preferable—if it is tolerated—due to lower cost and once-weekly doses (rather than daily doses). WHAT'S NEW The FDA has added a warning to the packaging label for mefloquine, stating that it can cause serious neurological and psychiatric side effects. These reactions can persist for months, years, or permanently, even after discontinuation of mefloquine. Use of either atovaquone/proguanil (Malarone) or co-artemether (combination artemether-lumefantrine; called Coartem in the U.S. and Riamet in Europe) is preferred for standby emergency treatment, if this strategy is chosen by the traveler. -

10 Artemether-Lumefantrine for The
PEDIATRIC PHARMACOTHERAPY A Monthly Newsletter for Health Care Professionals from the University of Virginia Children’s Hospital Volume 16 Number 10 October 2010 Artemether-Lumefantrine for the Treatment of Malaria in Infants and Children Marcia L. Buck, Pharm.D., FCCP, FPPAG alaria remains a significant medical break-down, to non-toxic hemozoin. M burden in many parts of the world. It is Accumulation of heme and free radicals results in responsible for approximately 1 million deaths parasite death.1-5 per year, mostly in infants and children. The availability of artemisinin-based compounds, Artemether, like other artemisinin-derived derived from the Chinese plant Artemisia annua, compounds, acts quickly to rapidly reduce the during the past decade has introduced a new era parasite burden, while lumefantrine serves as a in the treatment of this disease. Effective and longer-acting agent to eliminate remaining well tolerated, these drugs appear to offer parasites. The combination is effective in strains substantial benefits over traditional agents such known to be resistant to traditional antimalarials as chloroquine or sulfadoxine-pyrimethamine. such as chloroquine, and can be used for Artemisinin-based combination therapies (ACT) infections acquired in areas known to have are recommended as first-line therapy for malaria parasites that are multidrug-resistant.1-5 by the World Health Organization (WHO) and have been accepted as a mainstay of treatment in Pharmacokinetics more than 70 countries.1-3 Both artemether and lumefantrine are well absorbed after oral administration. Peak plasma A combination of artemether and lumefantrine artemether concentrations typically occur within recently became the first ACT to be made 2 hours after administration and peak available in the United States. -

Malaria Treatment
TREATMENT OF MALARIA IN ADULT AND PEDIATRIC PATIENTS WHO recommendations are to treat uncomplicated malaria from all species with artemisinin-based combination therapy (such as Coartem™) based on safety and effectiveness of the drug, as well as to help streamline treatment recommendations for malaria. CDC and WHO treatment guidelines now concur with recommendations for Coartem™ as first line agent with known chloroquine resistance or species not identified. The CDC currently recommends chloroquine- containing regimens as first line therapy for chloroquine-susceptible species of malaria, which differs from WHO recommendations. We have elected to streamline institutional recommendations to be in line with WHO recommendations when there is discrepancy, given local drug availability and that Coartem™ clears parasitemia faster than chloroquine. Definitions Uncomplicated malaria: Persons with a positive blood smear OR history of recent possible exposure and no other recognized pathology who do not meet severe criteria Severe malaria: Persons with a positive blood smear OR history of recent possible exposure and no other recognized pathology who have one or more of the following clinical criteria: Parasitemia of >5% Renal failure Disseminated intravascular Jaundice Impaired Pulmonary edema coagulation Repeated generalized consciousness/coma Acute respiratory distress Spontaneous bleeding convulsions Severe normocytic syndrome Acidosis anemia Circulatory shock Hemoglobinuria Chloroquine sensitivity: P. falciparum acquired in Central America (west of the Panama Canal), Haiti, and Dominican Republic All P. malariae, P. knowlesi, and P. ovale All P. vivax EXCEPT infections acquired in Papua New Guinea or Indonesia Uncomplicated malaria P. falciparum or not identified P. malariae or P. knowlesi P. vivax or P. ovale chloroquine sensitive P. -

Hydroxychloroquine (All Populations Monograph)
3/17/2020 Clinical Pharmacology powered by ClinicalKey Hydroxychloroquine (All Populations Monograph) Indications/Dosage expand all | collapse all Labeled malaria rheumatoid arthritis malaria prophylaxis systemic lupus erythematosus (SLE) Off-Label, Recommended coronavirus disease 2019 (COVID-19) † severe acute respiratory syndrome coronavirus lupus nephritis † 2 (SARS-CoV-2) infection † polymorphous light eruption † † Off-label indication Per the manufacturer, this drug has been shown to be active against most strains of the following microorganisms either in vitro and/or in clinical infections: Plasmodium falciparum, Plasmodium malariae, Plasmodium ovale, Plasmodium vivax. NOTE: The safety and effectiveness in treating clinical infections due to organisms with in vitro data only have not been established in adequate and well-controlled clinical trials. This drug may also have activity against the following microorganisms: severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2). NOTE: Some organisms may not have been adequately studied during clinical trials; therefore, exclusion from this list does not necessarily negate the drug’s activity against the organism. For the treatment of malaria due to susceptible strains of P. falciparum, P. knowlesi†, P. malariae, P. ovale, and P. vivax https://www.clinicalkey.com/pharmacology/monograph/print?cpnum=300&type=0&printSections=monindi&printSections=monsup&printSections=mon… 1/87 3/17/2020 Clinical Pharmacology powered by ClinicalKey Oral dosage Adults 13 mg (10 mg base)/kg/dose [Max: 800 mg (620 mg base)/dose] PO, then 6.5 mg (5 mg base)/kg/dose [Max: 400 mg (310 mg base)/dose] PO at 6, 24, and 48 hours after the initial dose.[41806] [64059] For P.