How to Assess and Stabilize a Mare Suspected of Periparturient Hemorrhage in the Field
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

October 2009 Pin Titles Americas, Europe and South Pacific
OCTOBER 2009 PIN TITLES AMERICAS, EUROPE AND SOUTH PACIFIC NEW BLUE DIAMOND EXECUTIVES Name Hometown Sponsor Derek Tillotson Salt Lake City, Utah, United States GOT YOUR NUMBER, INC NEW DIAMOND EXECUTIVES Name Hometown Sponsor Carmela Phillips Corona Del Mar, California, United States ELDRIDGE, LISA Elizabeth Rowe Mtubatuba, South Africa HINRICHSEN, STEVEN Helena Kammer Frankfurt, Germany EDELMANN, SUSANNE Hong Jie Euro Kft Gu Pinghua Budapest, Hungary Laurence Brem Matzenheim, France SCHILLINGER, MIREILLE Marco Roberto and Sally Mastrantonio North Vancouver, British Columbia, Canada VINT, JAMES Peter Auer Schlehdorf, Germany KAMMER, HELENA Retha Argent Krugersdorp, South Africa BETTINGS, ELANA Tonya R King Ione, California, United States HUTMACHER, DOUG NEW EMERALD EXECUTIVES Name Hometown Sponsor Brenden Moore Enoch, Alberta, Canada OLDHAM, SUE I Synchronex Consulting KFT Szentendre, Hungary ARANY, ZSUZSANNA Vagvolgyi Es Fiai BT Dunakeszi, Hungary KEREKES, ANDRAS Jeannette Bray Lake Stevens, Washington, United States MACHORRO, KENDA Aleksandr Shevyakov Russia ZHIDENKO ALEXANDR Elana Bettings Krugersdorp, South Africa NEL, ELRINA Erika Dienes, Konkoly Gabor Budapest, Hungary ZABORSZKY, ANDREA Hailing Yu San Jose, California, United States FENG, WEI Hong Jie Euro Kft Gu Pinghua Budapest, Hungary LUN-X 2008 KFT Hongyan Li, Zihong Zheng Bellevue, Washington, United States SUPER SUCCESS INT'L INC. Jeff Dang, Terri Tu Renton, Washington, United States NAGAO, PRISCILLA Justin and Johanna Armstrong Calgary, Alberta, Canada GANSKE, JULIETTE -

Onset of Luteal Activity in Non-Foaling Mares During the Early Breeding Season in Finland
Acta vet. scand. 1991,32. 319-325 . Onset of Luteal Activity in Non-Foaling Mares during the Early Breeding Season in Finland By Erkki Koskinen and Terttu Katila Agricultural Research Centre, Equine Research Station, Ypiijii,and College of Veterinary Medicine, Department of Clinical Veterinary Sciences, Hautjiirvi, Finland. Koskinen, E. and T. Katila: Onset of luteal activity in non-foaling mares during the early breeding season in Finland. Acta vet. scand. 1991,32,319-325. - The luteal activity in mares was studied in the Equine Research Station (ERS) and in trotting stables (TS) in South-Finland. The mares were Standardbreeds in the TS and mainly Finnhorses in the ERS. Between January and June blood was collected once a week for serum progesterone determinations. The mares in the ERS were distributed in I of 3 groups: three-years old not yet in training (N = 38), brood mares (N =21) and mares in training (N =47). A 4th group was the mares in training in the trotting stables (N = 73). Every 5th mare in the ERS and every 4th mare in the trotting stables were cycling already at the beginning of the year. Onset of luteal activity in anoestrous mares was most common in the middle of May. Over 95 % of the mares were cycling at the beginning of June. In the ERS 40 % of the Finnhorse mares in training were cycling through the win ter. The three-years old and the brood mares were all anoestrous during winter. They started to cycle on average before the middle of May. Anoestrous training mares started before the middle of April. -
Reproductive Behavior of the Stallion
Behavior 0749-0739186 $00.00 + .20 Reproductive Behavior of the Stallion Sue McDonnell, Ph.D.* The article begins with a brief description of the reproductive behavior of semi-wild and feral horses, which is intended to provide a background on the reproductive patterns and the specific behavioral elements comprising courtship and mating in the horse. The remain- der of the article focuses on the domestic stallion. Various breeding conditions are described, including normal breeding performance. Fi- nally, considerable attention is devoted to sexual behavior problems. SEMI-WILD AND FERAL ENVIRONMENT Considerable observational information has amassed concerning the behavior of semi-wild and feral horses throughout the world. The following summary of reproductive behavior is based on descriptions of behavior of free-running horses in the Western United States and Canada, in the New Forest of Southern England, in Poland, and on islands off the coast of North America. 1, 5, 8, 10, 13, 21, 24, 25, 29, 30 Each of these populations, although free-running for most or all of the year, is subject to breeding or population management. Reproductive Patterns Free-running horses are polygynous, seasonal breeders with some overlap of the late spring to midsummer foaling and mating seasons. Breeding occurs within a harem group that generally consists of one stallion and several mares with their foals and yearling offspring. The harem group is a relatively stable social unit year-round. Most of the matings observed among the Pryor Mountain, Western Canadian, Pol- ish, and New Forest populations are between April and July. Although most harem mares will be bred by the harem stallion, younger mares may be bred by Syear-old colts that are occasionally tolerated as group members by a harem stallion. -

44259 - Materie 16/08/04 7:27 Side I
A Windfall for the Magnates. The Development of Woodland Ownership in Denmark c. 1150-1830 Fritzbøger, Bo Publication date: 2004 Document version Publisher's PDF, also known as Version of record Citation for published version (APA): Fritzbøger, B. (2004). A Windfall for the Magnates. The Development of Woodland Ownership in Denmark c. 1150-1830. Syddansk Universitetsforlag. Download date: 29. Sep. 2021 44259 - Materie 16/08/04 7:27 Side i “A Windfall for the magnates” 44259 - Materie 16/08/04 7:27 Side ii Denne afhandling er af Det Humanistiske Fakultet ved Københavns Universitet antaget til offentligt at forsvares for den filosofiske doktorgrad. København, den 16. september 2003 John Kuhlmann Madsen Dekan Forsvaret finder sted fredag den 29. oktober 2004 i auditorium 23-0-50, Njalsgade 126, bygning 23, kl. 13.00 44259 - Materie 16/08/04 7:27 Side iii “A Windfall for the magnates” The Development of Woodland Ownership in Denmark c. 1150-1830 by Bo Fritzbøger University Press of Southern Denmark 2004 44259 - Materie 16/08/04 7:27 Side iv © The author and University Press of Southern Denmark 2004 University of Southern Denmark Studies in History and Social Sciences vol. 282 Printed by Special-Trykkeriet Viborg a-s ISBN 87-7838-936-4 Cover design: Cover illustration: Published with support from: Forskningsstyrelsen, Danish Research Agency The University of Copenhagen University Press of Southern Denmark Campusvej 55 DK-5230 Odense M Phone: +45 6615 7999 Fax: +45 6615 8126 [email protected] www.universitypress.dk Distribution in the United States and Canada: International Specialized Book Services 5804 NE Hassalo Street Portland, OR 97213-3644 USA Phone: +1-800-944-6190 www.isbs.com 44259 - Materie 16/08/04 7:27 Side v Contents Preface . -

Folkemængden 1965
STATISTISKE MEDDELELSER 1968:3 Folkemængden 27. september 1965 og Danmarks administrative inddeling Population 27 September 1965 and Administrative Division DANMARKS STATISTIK Kobenhavn 1968 DANMARKS STATISTIK BIBUOTEKET Tidligere publikationer om folketællingerne i Danmark STATISTISK TABELVÆRK Folketællingen 1801 og 1834: I, 1 1890: IV A, 8a og b 1840: I, 6 1901: V A, 3 og 4 1845: I, 10 1911: V A, 9 og 10 1850: II, 1, 3 og 7 1916: VA, 14 1855: II, 12,1.-2.afd. 1921: V A, 16 1860: III, 1 1930: V A, 20 1870: III, 18 1940: V A, 22 og 23 1880: IV A, 3 1960: 1963, I, III, V, VI 1960: 1964, I, II, IV, V STATISTISKE MEDDELELSER Folketællingen 1855: 1, 3, II 1921: 4, 63, 1 1860: 1, 6, VI 1925: 4, 76, 1 1870: 2, 12, I 1930: 4, 86, 2 1880: 3, 4, IV 1935: 4, 101, 1 1890: 3, 12, I 1935: 4, 105, 1 1901: 4, 10, 3 1940: 4, 113, 3 1906: 4, 21, 1 1945: 4, 128, 1.-2. 1906: 4, 28, 5 1950: 4, 147, 1 1911: 4, 37, 1 1950: 4, 162, 1.-4. 1916: 4, 51, 1 1955: 4, 166, 1 Befolkningsforholdene i Danmark i det 19. Arhundrede: Statistisk Tabel- værk V A, 5. Danmarks administrative inddeling (nov. 1930) : Statistiske Meddelelser 4, 86, 1. Folkemængden 26. september 1960 og Danmarks administrative ind- deling (nov. 1962) : Statistiske Meddelelser 1962: 13. Folketællingen 1950: Statistiske Efterretninger 1953, nr. 13. Folketællingen 1955: Statistiske Efterretninger 1959, nr. 20. Danmarks Statistik Rettelse til Folkemængden 27. september 1965 og Danmarks administrative inddeling". -

Club Health Assessment MBR0087
Club Health Assessment for District 101 M through April 2021 Status Membership Reports Finance LCIF Current YTD YTD YTD YTD Member Avg. length Months Yrs. Since Months Donations Member Members Members Net Net Count 12 of service Since Last President Vice Since Last for current Club Club Charter Count Added Dropped Growth Growth% Months for dropped Last Officer Rotation President Activity Account Fiscal Number Name Date Ago members MMR *** Report Reported Report *** Balance Year **** Number of times If below If net loss If no When Number Notes the If no report on status quo 15 is greater report in 3 more than of officers thatin 12 months within last members than 20% months one year repeat do not haveappears in two years appears appears appears in appears in terms an active red Clubs more than two years old 18406 ALFTA 01/22/1973 Active 17 1 1 0 0.00% 17 30 0 2 VP,MC,SC N/R 18356 ÅMÅL 01/14/1955 Active 2 0 4 -4 -66.67% 6 49 1 M,VP,MC,SC N/R 18360 ARBOGA 10/22/1951 Active 22 2 2 0 0.00% 22 2 0 N SC N/R 18358 ÅRJÄNG 11/12/1957 Cancelled(6*) 0 0 22 -22 -100.00% 22 22 1 None P,S,T,M,VP 24+ MC,SC 18359 ARVIKA 01/17/1956 Active 19 2 2 0 0.00% 19 22 0 N MC 16 18361 ASKERSUND 01/26/1960 Active 27 0 0 0 0.00% 25 5 2 R MC,SC 24 18408 AVESTA 12/28/1951 Active 28 0 2 -2 -6.67% 30 5 1 N MC,SC 4 18409 BERGSJÖ 09/01/1969 Active 20 0 2 -2 -9.09% 22 47 0 N MC,SC 16 18411 BORLÄNGE 05/28/1953 Active 24 0 2 -2 -7.69% 26 1 1 N MC,SC 8 46841 BORLÄNGE STORA TUNA 01/07/1987 Active 17 1 0 1 6.25% 16 0 N MC,SC 24+ 18362 DEGERFORS 03/15/1956 Active 15 0 0 0 0.00% -

Embryo Flush & Transfer
EMBRYO FLUSH & TRANSFER Embryo transfer (ET) is the process of flushing an embryo from a mare (donor) and placing it into the uterus of a second mare (recipient) to be carried for the remainder of the pregnancy. The genetic makeup of the resulting foal will be that of the donor mare and stallion, the recipient is merely a “surrogate mother”. Embryo transfer has been widely accepted by most breed registries in most countries. ET may benefit your breeding program if: your mare has fertility problems which decrease her ability to carry a pregnancy; the mare is a performance horse with a busy show or race schedule; you want to obtain a foal from a 2 year old filly; or you want to increase the number of foals produced from a valuable mare. The process starts when we synchronize the donor mare with 2 or 3 recipients’ cycles. This is done by monitoring the mares estrus cycle via veterinarian ultrasound and administering various drugs such as Regumate®, hCG, and prostaglandin, to control the timing of ovulation. It is crucial that the recipient mare ovulate within either 1 day before or 2 days after the donor mare ovulates. The donor mare is inseminated and she is monitored for ovulation. The donor mares ovulation date is considered day 0, with the flush to be performed on day 6, 7 or 8. On the day of the donor mare’s flush she will once again be examined via ultrasound to confirm the number of ovulation’s that occurred and the condition of her uterus. -

How We Select, Prepare, and Maintain a Stimulus/Mount Mare. 59Th
AMBULATORY PRACTICE How We Select, Prepare, and Maintain a Stimulus/Mount Mare Kristina Janson Whitesell, DVM*; and Sue M. McDonnell, MS, PhD, CAAB A stimulus/mount mare that is an easy keeper, sound, and reliably attractive and receptive to most stallions, as well as comfortable with her work and easy to handle, is invaluable to a breeding facility. Organized and systematic behavior evaluation specific to your clinic’s protocols before selection will reveal undesirable behaviors that may prove unsafe in the semen collection environ- ment or may complicate or prevent successful semen collection. In the case of intact mares, bilateral ovariectomy performed through colpotomy or a hand-assisted laparoscopic approach with colpotomy allows for a short convalescent period compared with other approaches. Additionally, flank sensi- tivity can be avoided by colpotomy. In the absence of functional ovaries, frequent, low-dose estrogen supplementation can usually maintain estrus adequate for a stimulus/mount mare. Authors’ ad- dress: School of Veterinary Medicine, University of Pennsylvania, New Bolton Center, 382 West Street Road, Kennett Square, PA 19348; e-mail: [email protected]. *Corresponding and pre- senting author. © 2013 AAEP. 1. Introduction ural cover. Accordingly, a commonly used alterna- Although some stallions, initially or after training, tive to a cycling mare in estrus is a mare without respond adequately for semen collection in the ab- functional ovaries that is administered exogenous sence of a live mare, most semen collection facilities estrogen as needed to maintain estrus at a level do require a live mare to accommodate stallions that sufficient for the needs of the facility. -

07 Master Shorex.Qxd:SE7 Baltic
Shore Excursions 2007 scandinavia & russia se-7 Contents The Benefits of Booking With Us 2 Make Your Reservations Online 3 Frequently Asked Questions 4 The Medallion Collection/The Signature Collection 6 How to Choose Your Tours 9 Shore Excursion Prices 10 How to Book More Than One Tour in Each Port 10 Århus, Denmark 11 Copenhagen, Denmark 14 Gdansk, Poland 15 Gothenburg, Sweden 17 Hamburg, Germany 20 Helsinki, Finland 26 Kalmar, Sweden 31 Lübeck, Germany 33 Oslo, Norway 37 Riga, Latvia 42 Rønne, Bornholm, Denmark 44 Stockholm, Sweden 46 St. Petersburg, Russia 52 Tallinn, Estonia 63 Visby, Gotland, Sweden 68 Warnemünde, Germany 70 Ystad, Sweden 80 General Information 81 Some images supplied by Shutterstock 1 The Benefits of Booking Make Your Reservations With Us Online When you book your shore excursions with Holland America Now you can easily choose your tour times, book your Line, you can count on our Signature of Excellence® to tours and receive confirmation of your shore excursion consistently offer a superior experience ashore: reservations 24 hours a day. Visit us online at quality www.hollandamerica.com Clean and comfortable transportation equipment; we engage professional independent tour operators dedicated to Book online now, up until 10 days before sailing. Make your customer satisfaction. payment online via our secure website, and receive confirmation safety as well as your approximate tour departure times. You can also download the shore excursions, view tour prices, find answers to Tour operators have contractually agreed to comply with local frequently asked questions and read general information. government requirements and to carry liability insurance in amounts consistent with local standards to address personal Remember, online shore excursion reservations are processed injury and property damage claims. -

Valgberettigede Ved Folkethingsvalg I 1849
STATISTISK TAI3ELVJERK. NY RIEKKE, ANDET BIND, INDEHOLDENDE en tabellarisk Oversigt over de Valgberettigede ved Folkethingsvalg i Kongeriget Danmark og over Valgrettens Afbenyttelse sammesteds i Aaret 1849. KJÖBENHAVN. TRYKT HOS IIOFBOGTRYKKER BIANCO LUNO. 1851. 1+ 4 S DET STATISTISKE `,,,.f 7-it DEPARTEMENTS BI3LIOTEK DANMARK G DET STATISTISKE DEPARTEMENTS BIBLIOTEV, DAN :1A RIK INDLEDNING. Da den Indflydetse paa Folkets Velvmre og Udvikling, som den betydningsfulde Gave, Nationen har modtaget i Grundloven, vil komme til at yttre, vmsenlig vil vmre afhmngig af Maaden, paa hvilken Valgretten bliver afbenyttet, maa Man önske, at den offenlige Opmmrk- somhed ret alvorligen vil vmre henvendt paa denne Sag og paa hvad der med samme staaer i Forbindelse; og for at leyere Publikum et Hjmlpemiddel i saa Henseende, og for at belyse Valgretsforholdene, har man troet at burde udarbeide denne Oversigt over de Valgberettigede og over Valgrettens Afbenyttelse ved de sidstafholdte Folkethingsvalg, ved hvilken vort Fmdreland giver det förste Exempel paa en udförlig og omfattende statistisk Opfattelse og Fremstilling af et Forhold, der for Tiden spiller en saa höist vigtig Rolle i alle europmiske Stater. Hvad Landsthingsvalgene angaaer, da lader en lignende Oversigt paa Grund af Valgmaaden og den skriftlige Stemmeafgivning til Valg -Urnen sig ikke give. For at bidrage til at veilede dem, som ikke maatte vmre fortrolige med Betragtninger af den her omhandlede Art, eller som maatte mangle Tid eller Lyst til selvstmndige Undersögelser, meddeles tillige herved fölgende Resultater af Tabellerne, tilligemed nogle indledende Bemmrkninger, ved hvis Udarbeidelse Herr Professor V. B j e r ri n g har ydet sin sagkyndige Bistand. I de forskjellige Stater, der have en representativ Forfatning, ere Betingelserne for Valgrettens. -
How to Manage Hydrops Allantois/Hydrops Amnion in a Mare
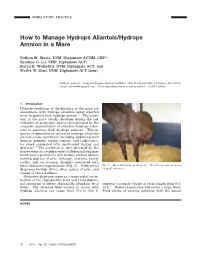
AMBULATORY PRACTICE How to Manage Hydrops Allantois/Hydrops Amnion in a Mare Nathan M. Slovis, DVM, Diplomate ACVIM, CHT*; Kristina G. Lu, VMD, Diplomate ACT; Karen E. Wolfsdorf, DVM, Diplomate ACT; and Walter W. Zent, DVM, Diplomate ACT (hon) Authors’ address: Hagyard Equine Medical Institute, 4250 Ironworks Pike, Lexington, KY 40511; e-mail: [email protected]. *Corresponding and presenting author. © 2013 AAEP. 1. Introduction Hydrops conditions of the placenta in the mare are uncommon, with hydrops allantois being reported more frequently than hydrops amnion.1 The condi- tion in the mare usually develops during the last trimester of pregnancy and is characterized by the excessive accumulation of allantoic (hydrops allan- tois) or amnionic fluid (hydrops amnion). The se- quelae of unnoticed or untreated hydrops allantois/ amnion can be significant, including abdominal wall hernias, prepubic tendon rupture, and cardiovascu- lar shock associated with unattended foaling and dystocia2–4 The condition is often detected by the horse owner as a sudden onset of abdominal enlarge- ment (over a period of a few weeks), ventral edema, varying degrees of colic, lethargy, anorexia, tachy- cardia, and, on occasion, dyspnea associated with intra-abdominal hypertension (Fig. 1). Differential Fig. 1. Mare with hydrops allantois. Note the pendulous “pear- diagnoses include twins, other causes of colic, and shaped” abdomen. causes of ventral edema. Definitive diagnosis requires a trans-rectal exam- ination of the reproductive tract and transabdomi- nal sonogram to detect abnormally abundant fetal whereas a normal volume at term ranges from 8 to fluids. The allantoic fluid volume in mares with 18 L.5 Rectal examination will reveal a large, fluid- hydrops allantois can range from 110 to 230 L, filled uterus of varying tightness with the dorsal NOTES 34 2013 ր Vol. -

Quality of Bathing Water 1988: Seventh Report
COMMISSION OF THE EUROPEAN COMMUNITIES COMMISSION DES COMMUNAUTÉS EUROPÉE"" L/J-.1V _JJ F BAT WATER ALITÉ DES EAUX DE BAIGNADE ■ *>~ <& t L- '4 «F • ■çptridh^-. r-v*ïe* - -rr-n &% ¥*"+- " R TfTVp $:$ t* >. / ^ ""#** . *& S QJi 3Yf Commission of the European Communities Commission des Communautés européennes QUALITY OF BATHING WATER LA QUALITÉ DES EAUX DE BAIGNADE 1988 SEGESsa Seventh report Septième rapport PARL. EUROP. Bibliofh. Directorate-General for Environment, Nuclear Safety and Civil Protection Direction générale Environnement, sécurité nucléaire et protection civile N.C./COM erF.'fh CL EUR 12579 1990 If, , à Published by the Commission of the European Communities Directorate-General for Environment, Nuclear Safety and Civil Protection Publié par la Commission des Communautés européennes Direction générale Environnement, sécurité nucléaire et protection civile LEGAL NOTICE Neither the Commission of the European Communities nor any person acting on behalf of the Commission is responsible for the use which might be made of the following information AVERTISSEMENT Ni la. Commission des Communautés européennes, ni aucune personne agissant au nom de la Commission n'est responsable de l'usage qui pourrait être fait des informations ci-après. Cataloguing data can be found at the end of this publication Une fiche bibliographique figure à la fin de cette publication. Luxembourg: Office for Officiai Publications of the European Communities, 1990 Luxembourg: Office des publications officielles des Communautés européennes, 1990 ISBN 92-826-1372-0