Terms Moving from Scrs 2018 Mesh to Descriptors in 2019
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Therapy for Movement Disorders
Cynthia Comella, MD, FAAN Rush University Medical Center Chicago, IL TREATMENT OF MOTOR SYMPTOMS IN PARKINSON DISEASE Disclosures . Compensation/honoraria for services as a consultant or an advisory committee member: Acadia, Aeon, Allergan, Inc; Impax Pharmaceuticals; Ipsen Biopharmaceuticals, Inc; Medtronic Inc.; Merz Pharmaceuticals; Neurocrine. Royalties: Cambridge, Humana Press; Wolters Kluwer Objectives Treatment of PD . Available treatments for motor PD Treatment of motor symptoms Treatment of motor complications Motor fluctuations Dyskinesia . Overview new therapies in clinical trial Not my objectives Before I came here I was confused about this subject. Having listened to your lecture I am still confused. But on a higher level. Enrico Fermi PD motor symptoms: Therapeutic targets Oertel W, Shulz JB. J Neurochem 2016 . No effective neuroprotective agent . Monotherapy (Efficacious) Levodopa Dopamine agonists: (pramipexole, ropinirole, rotigotine) MAO-B inhibitors: (selegiline, rasagiline) Amantadine (likely) . Motor fluctuations (Efficacious) Efficacious: Dopamine agonists (pramipexole, ropinirole, rotigotine, apomorphine) Levodopa gel intestinal infusions COMT inhibitors (entacapone, tolcapone, opicapone) MAO-B inhibitors (rasagiline, safinamide) Zonisamide Bilateral STN and GPi stimulation . Dyskinesia (Efficacious) Intestinal infusions Amantadine Bilateral STN and GPi stimulation clozapine Fox et al. Mov Disord March 2018 Modest benefit . MAO-B inhibitors (selegiline, rasagiline, safinamide) Modest benefit -

(12) Patent Application Publication (10) Pub. No.: US 2013/0253056A1 Nemas Et Al
US 20130253 056A1 (19) United States (12) Patent Application Publication (10) Pub. No.: US 2013/0253056A1 Nemas et al. (43) Pub. Date: Sep. 26, 2013 (54) CONTINUOUS ADMINISTRATION OF (60) Provisional application No. 61/179,511, filed on May LEVODOPA AND/OR DOPA 19, 2009. DECARBOXYLASE INHIBITORS AND COMPOSITIONS FOR SAME Publication Classification (71) Applicant: NEURODERM, LTD., Ness-Ziona (IL) (51) Int. Cl. A63L/216 (2006.01) (72) Inventors: Mara Nemas, Gedera (IL); Oron (52) U.S. Cl. Yacoby-Zeevi, Moshav Bitsaron (IL) CPC .................................... A6 IK3I/216 (2013.01) USPC .......................................................... 514/538 (73) Assignee: Neuroderm, Ltd., Ness-Ziona (IL) (57) ABSTRACT (21) Appl. No.: 13/796,232 Disclosed herein are for example, liquid aqueous composi (22) Filed: Mar 12, 2013 tions that include for example an ester or salt of levodopa, or an ester or salt of carbidopa, and methods for treating neuro Related U.S. Application Data logical or movement diseases or disorders such as restless leg (63) Continuation-in-part of application No. 12/961,534, syndrome, Parkinson's disease, secondary parkinsonism, filed on Dec. 7, 2010, which is a continuation of appli Huntington's disease, Parkinson's like syndrome, PSP. MSA, cation No. 12/836,130, filed on Jul. 14, 2010, now Pat. ALS, Shy-Drager syndrome, dystonia, and conditions result No. 7,863.336, which is a continuation of application ing from brain injury including carbon monoxide or manga No. 12/781,357, filed on May 17, 2010, now Pat. No. nese intoxication, using Substantially continuous administra 8,193,243. tion of levodopa and/or carbidopa or ester and/or salt thereof. -

Us 8530498 B1 3
USOO853 0498B1 (12) UnitedO States Patent (10) Patent No.: US 8,530,498 B1 Zeldis (45) Date of Patent: *Sep. 10, 2013 (54) METHODS FORTREATING MULTIPLE 5,639,476 A 6/1997 OShlack et al. MYELOMAWITH 5,674,533 A 10, 1997 Santus et al. 3-(4-AMINO-1-OXO-1,3-DIHYDROISOINDOL- 395 A 22 N. 2-YL)PIPERIDINE-2,6-DIONE 5,731,325 A 3/1998 Andrulis, Jr. et al. 5,733,566 A 3, 1998 Lewis (71) Applicant: Celgene Corporation, Summit, NJ (US) 5,798.368 A 8, 1998 Muller et al. 5,874.448 A 2f1999 Muller et al. (72) Inventor: Jerome B. Zeldis, Princeton, NJ (US) 5,877,200 A 3, 1999 Muller 5,929,117 A 7/1999 Muller et al. 5,955,476 A 9, 1999 Muller et al. (73) Assignee: Celgene Corporation, Summit, NJ (US) 6,020,358 A 2/2000 Muller et al. - 6,071,948 A 6/2000 D'Amato (*) Notice: Subject to any disclaimer, the term of this 6,114,355 A 9, 2000 D'Amato patent is extended or adjusted under 35 SS f 1939. All et al. U.S.C. 154(b) by 0 days. 6,235,756 B1 5/2001 D'Amatoreen et al. This patent is Subject to a terminal dis- 6,281.230 B1 8/2001 Muller et al. claimer 6,316,471 B1 1 1/2001 Muller et al. 6,326,388 B1 12/2001 Man et al. 6,335,349 B1 1/2002 Muller et al. (21) Appl. No.: 13/858,708 6,380.239 B1 4/2002 Muller et al. -

Bonviva, INN- Ibandronic Acid
European Medicines Agency London, 1 September 2005 Doc.Ref.: EMEA/278873/2005 Bonviva International Nonproprietary Name: Ibandronic acid Following the procedure EMEA/H/C/501/X/01 7 Westferry Circus, Canary Wharf, London E14 4HB, UK Tel. (44-20) 74 18 84 00 Fax (44-20) 74 18 86 68 E-mail: [email protected] http://www.emea.eu.int EMEA 2005 Reproduction and/or distribution of this document is authorised for non commercial purposes only provided the EMEA is acknowledged 1 SCIENTIFIC DISCUSSION 1.1 Introduction and rationale The MAH submitted an extension application under Annex II, point 2 iii to Commission Regulation (EC) No 1085/2003 to request the approval of a 150 mg tablet as a monthly dosing regimen of ibandronate only for the indication of “treatment of osteoporosis in postmenopausal women, in order to reduce the risk of vertebral fractures”. This claim is based on the results of a phase III study MOBILE (BM16549) comparing 100 and 150 mg once monthly to 2.5 mg once daily. Due to the inconveniences associated with intake of oral bisphosphonates (i.e. fasting conditions, frequent upper gastrointestinal intolerance) that may result in poor compliance, it was considered desirable to develop a more convenient drug formulation. Hence a 150 mg once monthly oral regimen is expected to offer greater convenience to postmenopausal women when compared to the currently approved 2.5mg once daily tablet. The development programme No new pre-clinical pharmacodynamic and pharmacokinetic studies have been performed in addition to those included in the previous submission for ibandronate 2.5 mg daily oral tablets. -

Summary of Drug Limitations Mary C
RON DESANTIS GOVERNOR SUMMARY OF DRUG LIMITATIONS MARY C. MAYHEW SECRETARY **Medications listed in this document may or may not require a prior authorization. Please view the Preferred Drug List at: http://ahca.myflorida.com/Medicaid/Prescribed_Drug/pharm_thera/fmpdl.shtml** Summary of Drug Limitations Abilify (aripiprazole) 2mg, 5mg, 20mg, 30mg tablets Minimum age = 6; Maximum of 1 tablet per day Abilify (aripiprazole) 10mg, 15mg tablets Minimum age = 6; Maximum of 15mg per day for ages = 6 - 11; Maximum of 30mg per day for ages = 12-17 Maximum of 1 tablet per day Abilify (aripiprazole) Discmelt 10mg, 15mg tabs Minimum age = 6; Maximum of 15mg per day for ages = 6 - 11; Maximum of 30mg per day for ages = 12-17; Maximum of 2 tablets per day Abilify (aripiprazole) 1mg/ml solution Minimum age = 6; Maximum of 15ml per day for ages = 6 - 11; Maximum of 30ml per day for ages = 12-17; Maximum of 30ml per day for ages =/> 18 Abilify Maintena (aripiprazole) syringe/vial Minimum age = 18; Maximum of 1 syringe or vial every 28 days Absorica (isotretinoin) 10mg, 20mg, 25mg,30mg, 35mg, & Minimum age = 12 40mg capsules Abstral (fentanyl citrate) sublingual tablets Minimum age = 18; Maximum of 4 sublingual tablets per day Acanya (benzoyl peroxide/clindamycin)Gel, gel pump Minimum Age= 12 Accolate (zafirlukast) tablets Maximum of 3 tablets per day Aciphex (rabeprazole) 5mg, 10mg sprinkle capsules Minimum age = 1; Maximum age = 11; Maximum of 1 capsule per day Aciphex (rabeprazole) 20mg tablets Minimum age = 1; Maximum of 2 tablets per day Actemra (tocilizumab) 80mg/4ml, 200mg/10ml, Minimum age= 2 400mg/20ml Vials, & 162mg/0.9ml Syringe Actimmune (Interferon Gamma-1b) Maximum of 6ml every 28days Actiq (fentanyl citrate) Lozenges Minimum age = 18; Maximum of 4 lozenges per day Activella (estradiol/norethindrone) tablets Minimum age = 18 Updated 02/28/2019 1 RON DESANTIS GOVERNOR SUMMARY OF DRUG LIMITATIONS MARY C. -

Belgian Veterinary Surveillance of Antibacterial Consumption
Belgian Veterinary Surveillance of Antibacterial Consumption National consumption report 2013 1 Summary This fifth BelVetSAC report, covers the results of the data collection on veterinary antibacterial consumption in Belgium in the year 2013. Data consist of all veterinary antibacterials sold to a veterinarian or pharmacist in Belgium and of antibacterial premixes incorporated in medicated feed intended to be used in Belgium for the year 2013. It includes thus consumption data for farm animals as well as companion animals. The denominator for animal production was the biomass (in kg) calculated as the sum of the amount of beef, pork and poultry meat produced in 2013, plus the number of dairy cattle present in Belgium times 500 kg of metabolic weight per head. As the usage data are concerned, this report shows for the second year in a row a decrease in the total consumption of antibacterial compounds in veterinary medicine of -6,6% between 2012 and 2013. Due to the relative stable animal production (expressed in biomass -0,3%) the decrease expressed in mg/kg biomass is -6,3%. When using 2011 as a reference, a reduction of -12,7% (expressed in mg/kg biomass) was achieved between 2011 and 2013, distributed over a reduction of -13,3% in antibacterial pharmaceuticals and -10,2% in antibacterial premixes. When looking more in detail to the different types of antibacterials used, it is observed that the penicillines (31,1%), sulphonamides (28,7%), and tetracyclines (24,1%) remain the three most used antibacterial classes. This year a substantial decrease in sulphonamide plus trimethoprim use and a limited decrease in penicillin and tetracycline use was observed. -

CCA Senior Care Options Formulary
Commonwealth Care Alliance Senior Care Option HMO SNP 2021 List of Covered Drugs Formulary 30 Winter Street • Boston, MA 02108 PLEASE READ: THIS DOCUMENT CONTAINS INFORMATION ABOUT THE DRUGS WE COVER IN THIS PLAN This formulary was updated on 08/01/2021. For more recent information or other questions, please contact Senior Care Options Program (HMO SNP) Member Services, at 1-866-610-2273 or, for TTY users, 711, 8 a.m. – 8 p.m., 7 days a week, or visit www.commonwealthcaresco.org. HPMS Approved Formulary File Submission ID 00021589, Version Number 13 Senior Care Options Program (HMO SNP) 2021 Formulary (List of Covered Drugs) PLEASE READ: THIS DO CUMENT CONTAINS INFORMATION ABOUT THE DRUGS WE COVER IN THIS PLAN HPMS Approved Formulary File Submission ID 00021589, Version Number 13 Note to existing members: This formulary has changed since last year. Please review this document to make sure that it still contains the drugs you take. When this drug list (formulary) refers to “we,” “us”, or “our,” it means Commonwealth Care Alliance. When it refers to “plan” or “our plan,” it means 2021 Senior Care Options Program. This document includes list of the drugs (formulary) for our plan which is current as of 08/01/2021. This formulary document applies to all SCO members. For an updated formulary, please contact us. Our contact information, along with the date we last updated the formulary, appears on the front and back cover pages. You must generally use network pharmacies to use your prescription drug benefit. Benefits, formulary, pharmacy n etwork, and/or copayments/coinsurance may change on January 1, 2022, and from time to time during the year. -
Guidelines for the Management of Heavy Menstrual Bleeding
i GUIDELINES FOR THE MANAGEMENT OF HEAVY MENSTRUAL BLEEDING Prepared by a Working Party on behalf of the National Health Committee ii MAY 1998 Women reporting with heavy menstrual bleeding 50% of women have menstrual blood loss Full menstrual history ● Examination ● Full blood count note1 Yes Prolonged irregular cycles No Refer Yes Abnormal exam specialist uterine size >12wks note 2 No mild or severe anaemic moderate treat < 80 g/l (80-115g/l) anaemia No Assess risk of endometrial hyperplasia low Offer medical therapy ● risk Unexplaine bodyweight 90kg heavy menstrual ● note5 note 6 age 45 years <2% bleeding ● other risk factors have 90% of women note 3 ● levonorgestrel endometrial >8% have hyperplasia intrauterine system ● tranexamic acid ● Assess endometrium nonsteroidal ● transvaginal ultrasound antiinflammatory agents ● (TVS) norethisterone long course or normal ● oc pill endometrium ● ● endometrial biopsy if danazol if one medical therapyfails endometrium 12mm others can be used note 7 or if TVS not available note 4 Treatment Hyperplastic endometrium success? or carcinoma No Yes Refer to specialist for hysteroscopic evaluation Continue Refer specialist me d i c a l for surgery therapy note8 note9 iii note 1 O In women <20 years old pelvic examination is unlikely to contribute to management of heavy bleeding (C) and the likelihood of pathology is small (C) O Increased likelihood (70%) of heavy menstrual blood loss >80mls/cycle if Hb <120g/l (A) O Consider pictorial blood loss assessment charts (appendix 6.5) for women with normal -

Aminolevulinic Acid (ALA) As a Prodrug in Photodynamic Therapy of Cancer
Molecules 2011, 16, 4140-4164; doi:10.3390/molecules16054140 OPEN ACCESS molecules ISSN 1420-3049 www.mdpi.com/journal/molecules Review Aminolevulinic Acid (ALA) as a Prodrug in Photodynamic Therapy of Cancer Małgorzata Wachowska 1, Angelika Muchowicz 1, Małgorzata Firczuk 1, Magdalena Gabrysiak 1, Magdalena Winiarska 1, Małgorzata Wańczyk 1, Kamil Bojarczuk 1 and Jakub Golab 1,2,* 1 Department of Immunology, Centre of Biostructure Research, Medical University of Warsaw, Banacha 1A F Building, 02-097 Warsaw, Poland 2 Department III, Institute of Physical Chemistry, Polish Academy of Sciences, 01-224 Warsaw, Poland * Author to whom correspondence should be addressed; E-Mail: [email protected]; Tel. +48-22-5992199; Fax: +48-22-5992194. Received: 3 February 2011 / Accepted: 3 May 2011 / Published: 19 May 2011 Abstract: Aminolevulinic acid (ALA) is an endogenous metabolite normally formed in the mitochondria from succinyl-CoA and glycine. Conjugation of eight ALA molecules yields protoporphyrin IX (PpIX) and finally leads to formation of heme. Conversion of PpIX to its downstream substrates requires the activity of a rate-limiting enzyme ferrochelatase. When ALA is administered externally the abundantly produced PpIX cannot be quickly converted to its final product - heme by ferrochelatase and therefore accumulates within cells. Since PpIX is a potent photosensitizer this metabolic pathway can be exploited in photodynamic therapy (PDT). This is an already approved therapeutic strategy making ALA one of the most successful prodrugs used in cancer treatment. Key words: 5-aminolevulinic acid; photodynamic therapy; cancer; laser; singlet oxygen 1. Introduction Photodynamic therapy (PDT) is a minimally invasive therapeutic modality used in the management of various cancerous and pre-malignant diseases. -
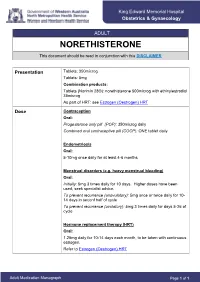
NORETHISTERONE This Document Should Be Read in Conjunction with This DISCLAIMER
King Edward Memorial Hospital Obstetrics & Gynaecology ADULT NORETHISTERONE This document should be read in conjunction with this DISCLAIMER Presentation Tablets: 350microg Tablets: 5mg Combination products: Tablets (Norimin 28®): norethisterone 500microg with ethinylestradiol 35microg As part of HRT: see Estrogen (Oestrogen) HRT Dose Contraception Oral: Progesterone only pill (POP): 350microg daily Combined oral contraceptive pill (COCP): ONE tablet daily Endometriosis Oral: 5-10mg once daily for at least 4-6 months Menstrual disorders (e.g. heavy menstrual bleeding) Oral: Initially: 5mg 3 times daily for 10 days. Higher doses have been used; seek specialist advice. To prevent recurrence (anovulatory): 5mg once or twice daily for 10- 14 days in seconf half of cycle To prevent recurrence (ovulatory): 5mg 3 times daily for days 5-26 of cycle Hormone replacement therapy (HRT) Oral: 1.25mg daily for 10-14 days each month, to be taken with continuous estrogen. Refer to Estrogen (Oestrogen) HRT Adult Medication Monograph Page 1 of 1 Norethisterone – Adult Administration Oral To be taken at the same time each day (or within 3 hours of the usual dose time). For Contraception: Start 4 weeks after the birth of baby (increased risk of abnormal vaginal bleeding if started earlier) Pregnancy 1st Trimester: Contraindicated 2nd Trimester: Contraindicated 3rd Trimester: Contraindicated Breastfeeding Considered safe to use. Progestogens are the preferred hormonal contraceptives as they do not inhibit lactation. Clinical Guidelines Estrogen (Oestrogen) HRT and Policies Progesterone Only Pill Contraception: Post Partum Gynaecology (Non-Oncological) Australian Medicines Handbook. Norethisterone. In: Australian References Medicines Handbook [Internet]. Adelaide (South Australia): Australian Medicines Handbook; 2017 [cited 2017 Apr 12]. -

Nur-Isterate Injection
SELECT THE REQUIRED INFORMATION PROFESSIONAL INFORMATION PATIENT INFORMATION LEAFLET SCHEDULING STATUS: S4 PROPRIETARY NAME AND DOSAGE FORM: NUR-ISTERATE Oily solution for intramuscular injection COMPOSITION: 1 ml contains norethisterone enantate (17-ethinyl-17-heptanoyloxy-4-estrene-3-one) 200 mg. Other ingredients are: benzyl benzoate, castor oil for injection. PHARMACOLOGICAL CLASSIFICATION: A. 21.8.2 Progesterones without estrogens. PHARMACOLOGICAL ACTION: Pharmacodynamic properties: Protection against conception is based primarily upon an alteration of the cervical mucous. This alteration is present for the whole of the duration of action and prevents the ascent of the sperm into the uterine cavity. Radioimmunological studies have shown that, during the first 5 to 7 weeks after injection, ovulation is suppressed as a result of the high plasma level of norethisterone. In addition, NUR- ISTERATE causes morphological changes in the endometrium which have the effect of rendering nidation of a fertilised egg difficult. Pharmacokinetic properties: Norethisterone enantate was completely absorbed after intramuscular injection. The ester was eventually completely hydrolysed to its pharmacologically active compound norethisterone once it was released from the depot. Maximum levels of norethisterone were measured at about 3 to 10 days after IM administration. They amounted on average to 13.4 5.4 ng/ml and 12.2 2.7 ng/ml about 7 days (median) after IM administration of 200 mg norethisterone enantate in 2 ml and 1 ml oily solution, respectively. Plasma levels of norethisterone declined in two disposition phases with half-lives of 4 to 5 days and 15 to 20 days, respectively, which were due to a biphasic release of norethisterone enantate from the depot. -

Antibody-Directed Phototherapy (ADP)
Antibodies 2013, 2, 270-305; doi:10.3390/antib2020270 OPEN ACCESS antibodies ISSN 2073-4468 www.mdpi.com/journal/antibodies Review Antibody-Directed Phototherapy (ADP) Hayley Pye 1,3, Ioanna Stamati 1, Gokhan Yahioglu 1,2, M. Adil Butt 3 and Mahendra Deonarain 1,2,* 1 Faculty of Natural Sciences, Imperial College London, Exhibition Road, London, SW7 2AZ, UK 2 PhotoBiotics Ltd, Montague House, Chancery Lane, Thrapston, Northamptonshire, NN14 4LN, UK 3 National Medical Laser Centre, Charles Bell House, 67-73 Riding House Street, London, W1W 7EJ, UK * Author to whom correspondence should be addressed; E-Mail: [email protected]. Received: 25 February 2013; in revised form: 3 April 2013 / Accepted: 4 April 2013 / Published: 25 April 2013 Abstract: Photodynamic therapy (PDT) is a clinically-approved but rather under-exploited treatment modality for cancer and pre-cancerous superficial lesions. It utilises a cold laser or LED to activate a photochemical reaction between a light activated drug (photosensitiser-drug) and oxygen to generate cytotoxic oxygen species. These free radical species damage cellular components leading to cell death. Despite its benefits, the complexity, limited potency and side effects of PDT have led to poor general usage. However, the research area is very active with an increasing understanding of PDT-related cell biology, photophysics and significant progress in molecular targeting of disease. Monoclonal antibody therapy is maturing and the next wave of antibody therapies includes antibody-drug conjugates (ADCs), which promise to be more potent and curable. These developments could lift antibody-directed phototherapy (ADP) to success. ADP promises to increase specificity and potency and improve drug pharmacokinetics, thus delivering better PDT drugs whilst retaining its other benefits.