Summary of Drug Limitations Mary C
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Therapy for Movement Disorders
Cynthia Comella, MD, FAAN Rush University Medical Center Chicago, IL TREATMENT OF MOTOR SYMPTOMS IN PARKINSON DISEASE Disclosures . Compensation/honoraria for services as a consultant or an advisory committee member: Acadia, Aeon, Allergan, Inc; Impax Pharmaceuticals; Ipsen Biopharmaceuticals, Inc; Medtronic Inc.; Merz Pharmaceuticals; Neurocrine. Royalties: Cambridge, Humana Press; Wolters Kluwer Objectives Treatment of PD . Available treatments for motor PD Treatment of motor symptoms Treatment of motor complications Motor fluctuations Dyskinesia . Overview new therapies in clinical trial Not my objectives Before I came here I was confused about this subject. Having listened to your lecture I am still confused. But on a higher level. Enrico Fermi PD motor symptoms: Therapeutic targets Oertel W, Shulz JB. J Neurochem 2016 . No effective neuroprotective agent . Monotherapy (Efficacious) Levodopa Dopamine agonists: (pramipexole, ropinirole, rotigotine) MAO-B inhibitors: (selegiline, rasagiline) Amantadine (likely) . Motor fluctuations (Efficacious) Efficacious: Dopamine agonists (pramipexole, ropinirole, rotigotine, apomorphine) Levodopa gel intestinal infusions COMT inhibitors (entacapone, tolcapone, opicapone) MAO-B inhibitors (rasagiline, safinamide) Zonisamide Bilateral STN and GPi stimulation . Dyskinesia (Efficacious) Intestinal infusions Amantadine Bilateral STN and GPi stimulation clozapine Fox et al. Mov Disord March 2018 Modest benefit . MAO-B inhibitors (selegiline, rasagiline, safinamide) Modest benefit -

(12) Patent Application Publication (10) Pub. No.: US 2013/0253056A1 Nemas Et Al
US 20130253 056A1 (19) United States (12) Patent Application Publication (10) Pub. No.: US 2013/0253056A1 Nemas et al. (43) Pub. Date: Sep. 26, 2013 (54) CONTINUOUS ADMINISTRATION OF (60) Provisional application No. 61/179,511, filed on May LEVODOPA AND/OR DOPA 19, 2009. DECARBOXYLASE INHIBITORS AND COMPOSITIONS FOR SAME Publication Classification (71) Applicant: NEURODERM, LTD., Ness-Ziona (IL) (51) Int. Cl. A63L/216 (2006.01) (72) Inventors: Mara Nemas, Gedera (IL); Oron (52) U.S. Cl. Yacoby-Zeevi, Moshav Bitsaron (IL) CPC .................................... A6 IK3I/216 (2013.01) USPC .......................................................... 514/538 (73) Assignee: Neuroderm, Ltd., Ness-Ziona (IL) (57) ABSTRACT (21) Appl. No.: 13/796,232 Disclosed herein are for example, liquid aqueous composi (22) Filed: Mar 12, 2013 tions that include for example an ester or salt of levodopa, or an ester or salt of carbidopa, and methods for treating neuro Related U.S. Application Data logical or movement diseases or disorders such as restless leg (63) Continuation-in-part of application No. 12/961,534, syndrome, Parkinson's disease, secondary parkinsonism, filed on Dec. 7, 2010, which is a continuation of appli Huntington's disease, Parkinson's like syndrome, PSP. MSA, cation No. 12/836,130, filed on Jul. 14, 2010, now Pat. ALS, Shy-Drager syndrome, dystonia, and conditions result No. 7,863.336, which is a continuation of application ing from brain injury including carbon monoxide or manga No. 12/781,357, filed on May 17, 2010, now Pat. No. nese intoxication, using Substantially continuous administra 8,193,243. tion of levodopa and/or carbidopa or ester and/or salt thereof. -

XERMELO™ (Telotristat Ethyl)
PHARMACY COVERAGE GUIDELINES ORIGINAL EFFECTIVE DATE: 5/18/2017 SECTION: DRUGS LAST REVIEW DATE: 5/20/2021 LAST CRITERIA REVISION DATE: 5/20/2021 ARCHIVE DATE: XERMELO™ (telotristat ethyl) Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific benefit plan. This Pharmacy Coverage Guideline must be read in its entirety to determine coverage eligibility, if any. This Pharmacy Coverage Guideline provides information related to coverage determinations only and does not imply that a service or treatment is clinically appropriate or inappropriate. The provider and the member are responsible for all decisions regarding the appropriateness of care. Providers should provide BCBSAZ complete medical rationale when requesting any exceptions to these guidelines. The section identified as “Description” defines or describes a service, procedure, medical device or drug and is in no way intended as a statement of medical necessity and/or coverage. The section identified as “Criteria” defines criteria to determine whether a service, procedure, medical device or drug is considered medically necessary or experimental or investigational. State or federal mandates, e.g., FEP program, may dictate that any drug, device or biological product approved by the U.S. Food and Drug Administration (FDA) may not be considered experimental or investigational and thus the drug, device or biological product may be assessed only on the basis of medical necessity. Pharmacy Coverage Guidelines are subject to change as new information becomes available. For purposes of this Pharmacy Coverage Guideline, the terms "experimental" and "investigational" are considered to be interchangeable. BLUE CROSS®, BLUE SHIELD® and the Cross and Shield Symbols are registered service marks of the Blue Cross and Blue Shield Association, an association of independent Blue Cross and Blue Shield Plans. -

Safinamide: an Add-On Treatment for Managing Parkinson's Disease
Journal name: Clinical Pharmacology: Advances and Applications Article Designation: REVIEW Year: 2018 Volume: 10 Clinical Pharmacology: Advances and Applications Dovepress Running head verso: Müller Running head recto: Safinamide for levodopa/carbidopa-treated PD patients with “off ” episodes open access to scientific and medical research DOI: http://dx.doi.org/10.2147/CPAA.S137740 Open Access Full Text Article REVIEW Safinamide: an add-on treatment for managing Parkinson’s disease Thomas Müller Abstract: Heterogeneous expression of neurotransmitter deficits results from onset and progression of Parkinson’s disease. Intervals, characterized by reappearance of motor and Department of Neurology, St. Joseph Hospital Berlin-Weißensee, Berlin, associated certain nonmotor symptoms, determine the end of good tolerability and efficacy of Germany oral levodopa therapy. These “OFF” states result from levodopa pharmacokinetics and disease progression-related deterioration of the central buffering capacity for fluctuations of dopamine levels. This review discusses safinamide as an add-on therapeutic agent in orally levodopa-treated patients with “OFF” phenomena. Safinamide provided beneficial effects on “OFF” symptoms in pivotal trials with doses of 50 or 100 mg once daily. Safinamide reversibly inhibits mono- amine oxidase B and declines abnormal glutamate release by modulation of potassium- and For personal use only. sodium ion channels. An ideal candidate for combination with safinamide is opicapone. This inhibitor of peripheral catechol-O-methyltransferase supports continuous brain delivery of levodopa and, thus, the continuous dopaminergic stimulation concept. Both compounds with their once-daily application and good tolerability may complement each other by reduction of necessary oral levodopa intakes and “OFF” times. Thus, a promising, future option will be combination of safinamide and opicapone in one formulation. -

Opicapone for the Management of End-Of-Dose Motor Fluctuations in Patients with Parkinson’S Disease Treated with L-DOPA
Opicapone for the management of end-of-dose motor fluctuations in patients with Parkinson’s disease treated with L-DOPA Andrew J. Lees MD1, Joaquim Ferreira MD2, Olivier Rascol MD3, Heinz Reichmann MD,4 Fabrizio Stocchi MD,5 Eduardo Tolosa MD,6 Werner Poewe MD7 1. University College London, Reta Lila Weston Institute, London, UK 2. Hospital de Santa Maria, Centro de Estudos Egas Moniz, Lisbon, Portugal 3. Departments of Clinical Pharmacology and Neurosciences, Clinical Investigation Center CIC 1436, NS-Park/FCRIN network and NeuroToul COEN Center, INSERM, Toulouse University Hospital and Toulouse3 University, Toulouse, France 4. Department of Neurology, Technische Universitaet Dresden, Dresden, Germany 5. Institute of Neurology, IRCCS San Raffaele Pisana, Rome, Italy 6. Neurology Service, Centro de Investigación Biomédica en Red sobre Enfermedades Neurodegenerativas (CIBERNED), Hospital Clínic, IDIBAPS, Universitat de Barcelona, Spain. 7. Department of Neurology, Innsbruck Medical University, Innsbruck, Austria Corresponding author Professor Andrew Lees University College London, Reta Lila Weston Institute, 1 Wakefield Street London WC1N 1PJ London, UK Email: [email protected] Direct telephone: + 44 20 7xxxxxxx Fax: +44 20 7xxxxxxx 1 Joaquim Ferreira [email protected] Olivier Rascol [email protected] Eduardo Tolosa [email protected] Fabrizio Stocchi [email protected] Heinz Reichmann [email protected] Werner Poewe [email protected] 2 Summary Introduction: Opicapone is a third generation, highly potent and effective catechol O‑methyltransferase (COMT) inhibitor that optimizes the pharmacokinetics and bioavailability of L- DOPA therapy. Areas covered: In this review, we describe the preclinical and clinical development of opicapone. -
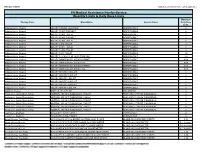
Quantity Limits/Daily Dose Limits
Effective 07/20/21 Alphabetical by Brand Name (when applicable) PA Medical Assistance Fee-for-Service Quantity Limits & Daily Dose Limits Maximum Therapy Class Brand Name Generic Name Daily Dose Limit Antipsychotics, Atypical ABILIFY 1 MG/ML SOLUTION ARIPIPRAZOLE 25 Antipsychotics, Atypical ABILIFY 10 MG DISCMELT ARIPIPRAZOLE 2 Antipsychotics, Atypical ABILIFY 10 MG TABLET ARIPIPRAZOLE 1 Antipsychotics, Atypical ABILIFY 15 MG DISCMELT ARIPIPRAZOLE 2 Antipsychotics, Atypical ABILIFY 15 MG TABLET ARIPIPRAZOLE 1 Antipsychotics, Atypical ABILIFY 2 MG TABLET ARIPIPRAZOLE 2 Antipsychotics, Atypical ABILIFY 20 MG TABLET ARIPIPRAZOLE 1 Antipsychotics, Atypical ABILIFY 30 MG TABLET ARIPIPRAZOLE 1 Antipsychotics, Atypical ABILIFY 5 MG TABLET ARIPIPRAZOLE 1.5 Antipsychotics, Atypical ABILIFY 9.75 MG/1.3 ML INJECTION VIAL ARIPIPRAZOLE 3.9 Antipsychotics, Atypical ABILIFY MAINTENA ER 300 MG SYRINGE ARIPIPRAZOLE 0.04 Antipsychotics, Atypical ABILIFY MAINTENA ER 300 MG VIAL ARIPIPRAZOLE 0.04 Antipsychotics, Atypical ABILIFY MAINTENA ER 400 MG SYRINGE ARIPIPRAZOLE 0.04 Antipsychotics, Atypical ABILIFY MAINTENA ER 400 MG VIAL ARIPIPRAZOLE 0.04 Antipsychotics, Atypical ABILIFY MYCITE 10 MG KIT ARIPIPRAZOLE 1 Antipsychotics, Atypical ABILIFY MYCITE 15 MG KIT ARIPIPRAZOLE 1 Antipsychotics, Atypical ABILIFY MYCITE 2 MG KIT ARIPIPRAZOLE 1 Antipsychotics, Atypical ABILIFY MYCITE 20 MG KIT ARIPIPRAZOLE 1 Antipsychotics, Atypical ABILIFY MYCITE 30 MG KIT ARIPIPRAZOLE 1 Antipsychotics, Atypical ABILIFY MYCITE 5 MG KIT ARIPIPRAZOLE 1 Antivirals, Herpes ABREVA 10% -

207145Orig1s000
CENTER FOR DRUG EVALUATION AND RESEARCH APPLICATION NUMBER: 207145Orig1s000 MEDICAL REVIEW(S) Clinical Review Leonard P. Kapcala, M.D. NDA 207145 XADAGO (SAFINAMIDE) CLINICAL REVIEW Application Type NDA Application Number 207145 Priority or Standard Standard Submit Date 9/21/16 Received Date 9/21/16 PDUFA Goal Date 3/21/17 Division / Office DNP/ODE 1 Reviewer Name Leonard P. Kapcala, M.D. Review Completion Date 2/7/17 Established Name SAFINAMIDE (Proposed) Trade Name XADAGO Therapeutic Class Monoamine Oxidase B Inhibitor Applicant Newron Formulation(s) Tablet Dosing Regimen Once daily orally Indication(s) Treatment of signs and symptoms of Parkinson's disease Intended Population(s) Patients with early and advanced Parkinson's disease 1 Reference ID: 4071416 Clinical Review Leonard P. Kapcala, M.D. NDA 207145 XADAGO (SAFINAMIDE) Table of Contents 1 RECOMMENDATIONS/RISK BENEFIT ASSESSMENT ......................................... 4 1.1 Recommendation on Regulatory Action ............................................................. 4 1.2 Risk Benefit Assessment .................................................................................... 4 1.3 Recommendations for Postmarket Risk Evaluation and Mitigation Strategies ... 5 1.4 Recommendations for Postmarket Requirements and Commitments ................ 5 2 INTRODUCTION AND REGULATORY BACKGROUND ........................................ 5 2.1 Product Information (Based Upon Sponsor Summary) ....................................... 5 2.2 Other Relevant Background Information ........................................................... -

212489Orig1s000 SUMMARY REVIEW
CENTER FOR DRUG EVALUATION AND RESEARCH APPLICATION NUMBER: 212489Orig1s000 SUMMARY REVIEW Gerald D. Podskalny, DO From Eric Bastings, MD Billy Dunn, MD Subject Joint Summary Review NDA/BLA # and Supplement# NDA 212489 Applicant Neurocrine Biosciences, Inc. Date of Submission 04/26/2019 PDUFA Goal Date 04/26/2020 Proprietary Name Ongentys Established or Proper Name Opicapone Dosage Form(s) 25-mg and 50-mg capsules Adjunctive treatment to levodopa/carbidopa in patients Applicant Proposed with Parkinson’s disease (PD) experiencing “off” Indication(s)/Population(s) episodes Applicant Proposed Dosing 50 mg orally once daily at bedtime. Regimen(s) Regulatory Action Approval Recommended Adjunctive treatment to levodopa/carbidopa in patients Indication(s)/Population(s) (if with Parkinson’s disease (PD) experiencing “off” applicable) episodes. Recommended Dosing 50 mg orally once daily at bedtime. Regimen(s) (if applicable) 1 Reference ID: 4597937 Reference ID: 4597937 1. Benefit-Risk Assessment Benefit-Risk Integrated Assessment Parkinson’s disease (PD) is the second most common neurodegenerative disease, with an estimated prevalence of 930,000 individuals in the United States. PD is caused by progressive loss of dopamine producing neurons in the substantia nigra located in the midbrain. The cardinal motor features of PD are bradykinesia, tremor, rigidity, and postural instability. As PD progresses, it causes increasing motor disability. Medications that replace or enhance the effects of dopamine, such as levodopa, treat the motor aspects of PD and remain the mainstay of treatment. About 5 years after starting treatment with levodopa, many patients develop motor fluctuations (dyskinesia and wearing-off). In advanced PD (approaching 10 years with PD and beyond), patients may develop cognitive impairment, neuropsychiatric symptoms (e.g., hallucinations and impulse control disorders) and impaired autonomic function (e.g., incontinence and orthostatic hypotension). -

Mississippi Division of Medicaid Universal Preferred Drug List
MISSISSIPPI DIVISION OF MEDICAID EFFECTIVE 01/01/2021 UNIVERSAL PREFERRED DRUG LIST Version 2021.13a Updated: 8-30-2021 (For All Medicaid, MSCAN and CHIP Beneficiaries) Conduent’s SmartPA Pharmacy Application (SmartPA) is a proprietary electronic prior authorization system used for Medicaid fee for service claims. MSCAN plans may/may not -have electronic PA functionality. However, they must adhere to Medicaid’s PA criteria. THERAPEUTIC PREFERRED AGENTS NON-PREFERRED AGENTS PA CRITERIA DRUG CLASS ACNE AGENTS ANTI-INFECTIVE clindamycin gel (generic Cleocin-T) ACZONE (dapsone) Maximum Age Limit clindamycin lotion AKNE-MYCIN (erythromycin) • 21 years – all agents except clindamycin solution azelaic acid isotretinoins AMZEEQ FOAM (minocycline) AZELEX (azelaic acid) CLEOCIN-T (clindamycin) CLINDAMYCIN PAC (clindamycin) CLINDAGEL (clindamycin) clindamycin foam clindamycin gel daily (generic Clindagel) dapsone ERY (erythromycin) ERYGEL (erythromycin) erythromycin gel, swabs, solution EVOCLIN (clindamycin) KLARON (sulfacetamide) sulfacetamide RETINOIDS RETIN-A (tretinoin) adapalene tretinoin cream AKLIEF (trifarotene) ALTRENO (tretinoin) ARAZLO (tazarotene) ATRALIN (tretinoin) AVITA (tretinoin) DIFFERIN (adapalene) FABIOR (tazarotene) PLIXDA (adapalene) 1 Drug coverage subject to the rules and regulations set forth in Sec. 1927 of Social Security Act.This is not an all-inclusive list of available covered drugs and includes only managed categories. Unless otherwise stated, the listing of a particular brand or generic name includes all dosage forms of that drug. NR indicates a new drug that has not yet been reviewed by the P&T Committee. PREFERRED BRANDS will not count toward the two brand monthly Rx limit. Drugs highlighted in yellow denote a change in PDL status. An * denotes existing users will be grandfathered; grandfathering is defined as approving a Non-Preferred agent for an existing user; all other changes will not qualify for grandfathering. -
Third Quarter 2017 Update
JULY 2017 THIRD QUARTER 2017 UPDATE CHANGES TO THE HIGHMARK DRUG FORMULARIES Following is the Third Quarter 2017 update to the Highmark Drug Formularies and pharmaceutical management procedures. The formularies and pharmaceutical management procedures are updated on a quarterly basis, and the following changes reflect the decisions made in May 2017 by our Pharmacy and Therapeutics Committee. These updates are effective on the dates noted throughout this document. Please reference the guide below to navigate this communication: Section I. Highmark Commercial and Healthcare Reform Formularies A. Changes to the Highmark Comprehensive Formulary and the Highmark Comprehensive Healthcare Reform Formulary B. Changes to the Highmark Progressive Formulary and the Highmark Progressive Healthcare Reform Formulary C. Changes to the Highmark Healthcare Reform Essential Formulary D. Updates to the Pharmacy Utilization Management Programs 1. Prior Authorization Program 2. Managed Prescription Drug Coverage (MRxC) Program 3. Quantity Level Limit (QLL) Programs Section II. Highmark Medicare Part D Formularies A. Changes to the Highmark Medicare Part D 5-Tier Incentive Formulary B. Changes to the Highmark Medicare Part D 5-Tier Closed Formulary C. Additions to the Specialty Tier D. Updates to the Pharmacy Utilization Management Programs 1. Prior Authorization Program 2. Managed Prescription Drug Coverage (MRxC) Program 3. Quantity Level Limit (QLL) Program As an added convenience, you can also search our drug formularies and view utilization management policies on the Provider Resource Center (accessible via NaviNet® or our website). Click the Pharmacy/Formulary Information link from the menu on the left Highmark Blue Shield is an independent licensee of the Blue Cross and Blue Shield Association. -

A Spanish Consensus on the Use of Safinamide for Parkinson's Disease in Clinical Practice
brain sciences Review A Spanish Consensus on the Use of Safinamide for Parkinson’s Disease in Clinical Practice Javier Pagonabarraga 1,2,3,*, José Matías Arbelo 4,5 , Francisco Grandas 6,7, Maria-Rosario Luquin 8,9, Pablo Martínez Martín 10,11 , Mari Cruz Rodríguez-Oroz 12,13, Francesc Valldeoriola 14,15 and Jaime Kulisevsky 1,2,3,16,17 1 Movement Disorders Unit, Neurology Department, Hospital de la Santa Creu i Sant Pau, 08041 Barcelona, Spain; [email protected] 2 Department of Medicine, Autonomous University of Barcelona, 08193 Barcelona, Spain 3 Centro de Investigación en Red sobre Enfermedades Neurodegenerativas (CIBERNED), 28031 Madrid, Spain 4 Movement Disorders Unit, Neurology Department, Hospital Universitario San Roque, 35001 Las Palmas, Spain; [email protected] 5 Department of Medicine, Universidad Fernando Pessoa-Canarias, 35450 Las Palmas, Spain 6 Movement Disorders Unit-CSUR, Neurology Department, Hospital General Universitario Gregorio Marañón, 28007 Madrid, Spain; [email protected] 7 Department of Medicine, Universidad Complutense de Madrid, 28040 Madrid, Spain 8 Movement Disorders Unit, Clínica Universidad de Navarra (CUN), 31008 Pamplona, Spain; [email protected] 9 Navarra Institute for Health Research (IdiSNA), 31008 Pamplona, Spain 10 Instituto de Salud Carlos III, 28029 Madrid, Spain; [email protected] 11 Centro de Investigación Biomédica en Red sobre Enfermedades Neurodegenerativas (CIBERNED), 28031 Madrid, Spain 12 Neurology and Neuroscience Unit, Clínica Universidad de Navarra (CUN), 31008Pamplona, -

Opicapone Capsules for the Treatment of Parkinsons Disease (Pd) in Adult Patients Recommended for Restricted Use (Amber Initiation)
HERTFORDSHIRE MEDICINES MANAGEMENT COMMITTEE (HMMC) OPICAPONE CAPSULES FOR THE TREATMENT OF PARKINSONS DISEASE (PD) IN ADULT PATIENTS RECOMMENDED FOR RESTRICTED USE (AMBER INITIATION) Name: generic What it is Indication Date Decision NICE / SMC (trade) decision status Guidance last revised Opicapone 50mg Peripheral, Licensed as adjunctive October 2019 Final NICE TA: not hard capsules selective and therapy to available ® (Ongentys ) reversible catechol- preparations of NICE guidance 0-methyltransferase levodopa/ DOPA for Parkinson’s (COMT) inhibitor decarboxylase disease in adults inhibitors in adult (NG71) patients with SMC not Parkinson's disease recommended and end-of-dose motor AWMSG fluctuations who recommended cannot be stabilised on those combinations HMMC recommendation: Opicapone 50mg capsules, within licensed indications, is recommended for restricted use as AMBER initiation as a second line COMT inhibitor in adult patients with PD with end-of-dose motor fluctuations who are intolerant of entacapone and where the next step of treatment would be the non-oral treatment options or tolcapone. Background Information: Opicapone is the third COMT inhibitor licensed in the UK with the recommended dose of 50 mg as an adjunct to levodopa/DDCI inhibitors. It should be taken once-daily at bedtime, at least one hour before or after levodopa combinations. In certain patients, this may enable a simplified drug regimen which may potentially improve compliance. Some patients taking a complicated PD drug regimen may find it easier to add a single tablet such as opicapone and keep their familiar levodopa doses over the day. In contrast, entacapone has to be taken with each levodopa dose, which may be up to 10 times daily.