Adenosine Triphosphate Turnover in Humans. Decreased Degradation During Relative Hyperphosphatemia
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

ATP—The Free Energy Carrier
ATP—The Free Energy Carrier How does the ATP molecule capture, store, and release energy? Why? A sporting goods store might accept a $100 bill for the purchase of a bicycle, but the corner store will not take a $100 bill when you buy a package of gum. That is why people often carry smaller denominations in their wallets—it makes everyday transactions easier. The same concept is true for the energy transactions in cells. Cells need energy (their “currency”) to take care of everyday functions, and they need it in many denominations. As humans we eat food for energy, but food molecules provide too much energy for our cells to use all at once. For quick cellular transactions, your cells store energy in the small molecule of ATP. This is analogous to a $1 bill for your cells’ daily activities. Model 1 – Adenosine Triphosphate (ATP) NH2 N N O– O– O– CH OP OP OP O– N N O 2 ADENINE O O O TRI-PHOSPHATE GROUP OH OH RIBOSE 1. The diagram of ATP in Model 1 has three parts. Use your knowledge of biomolecules to label the molecule with an “adenine” section, a “ribose sugar” section, and a “phosphate groups” section. 2. Refer to Model 1. a. What is meant by the “tri-” in the name adenosine triphosphate? 3 PHOSPHATES b. Discuss with your group what the structure of adenosine diphosphate (ADP) might look like. Draw or describe your conclusions. SAME AS ABOVE, BUT WITH ONLY 2 PHOSPHATES IN PHOSPHATE GROUP. ATP— The Free Energy Carrier 1 Model 2 – Hydrolysis of ATP H2O NH2 NH2 Energy N – – – N – – N O O O N O O O– CH OPOPOPO– CH O P O P OH HO P O– N N O 2 N N O 2 + O O O O O O Inorganic OH OH OH OH Phosphate (Pi) 3. -

Use of Phosphate Solubilizing Bacteria to Leach Rare Earth Elements from Monazite-Bearing Ore
Minerals 2015, 5, 189-202; doi:10.3390/min5020189 OPEN ACCESS minerals ISSN 2075-163X www.mdpi.com/journal/minerals Article Use of Phosphate Solubilizing Bacteria to Leach Rare Earth Elements from Monazite-Bearing Ore Doyun Shin 1,2,*, Jiwoong Kim 1, Byung-su Kim 1,2, Jinki Jeong 1,2 and Jae-chun Lee 1,2 1 Mineral Resources Resource Division, Korea Institute of Geoscience and Mineral Resources (KIGAM), Gwahangno 124, Yuseong-gu, Daejeon 305-350, Korea; E-Mails: [email protected] (J.K.); [email protected] (B.K.); [email protected] (J.J.); [email protected] (J.L.) 2 Department of Resource Recycling Engineering, Korea University of Science and Technology, Gajeongno 217, Yuseong-gu, Daejeon 305-350, Korea * Author to whom correspondence should be addressed; E-Mail: [email protected]; Tel.: +82-42-868-3616. Academic Editor: Anna H. Kaksonen Received: 8 January 2015 / Accepted: 27 March 2015 / Published: 2 April 2015 Abstract: In the present study, the feasibility to use phosphate solubilizing bacteria (PSB) to develop a biological leaching process of rare earth elements (REE) from monazite-bearing ore was determined. To predict the REE leaching capacity of bacteria, the phosphate solubilizing abilities of 10 species of PSB were determined by halo zone formation on Reyes minimal agar media supplemented with bromo cresol green together with a phosphate solubilization test in Reyes minimal liquid media as the screening studies. Calcium phosphate was used as a model mineral phosphate. Among the test PSB strains, Pseudomonas fluorescens, P. putida, P. rhizosphaerae, Mesorhizobium ciceri, Bacillus megaterium, and Acetobacter aceti formed halo zones, with the zone of A. -

Prebiological Evolution and the Metabolic Origins of Life
Prebiological Evolution and the Andrew J. Pratt* Metabolic Origins of Life University of Canterbury Keywords Abiogenesis, origin of life, metabolism, hydrothermal, iron Abstract The chemoton model of cells posits three subsystems: metabolism, compartmentalization, and information. A specific model for the prebiological evolution of a reproducing system with rudimentary versions of these three interdependent subsystems is presented. This is based on the initial emergence and reproduction of autocatalytic networks in hydrothermal microcompartments containing iron sulfide. The driving force for life was catalysis of the dissipation of the intrinsic redox gradient of the planet. The codependence of life on iron and phosphate provides chemical constraints on the ordering of prebiological evolution. The initial protometabolism was based on positive feedback loops associated with in situ carbon fixation in which the initial protometabolites modified the catalytic capacity and mobility of metal-based catalysts, especially iron-sulfur centers. A number of selection mechanisms, including catalytic efficiency and specificity, hydrolytic stability, and selective solubilization, are proposed as key determinants for autocatalytic reproduction exploited in protometabolic evolution. This evolutionary process led from autocatalytic networks within preexisting compartments to discrete, reproducing, mobile vesicular protocells with the capacity to use soluble sugar phosphates and hence the opportunity to develop nucleic acids. Fidelity of information transfer in the reproduction of these increasingly complex autocatalytic networks is a key selection pressure in prebiological evolution that eventually leads to the selection of nucleic acids as a digital information subsystem and hence the emergence of fully functional chemotons capable of Darwinian evolution. 1 Introduction: Chemoton Subsystems and Evolutionary Pathways Living cells are autocatalytic entities that harness redox energy via the selective catalysis of biochemical transformations. -
Discovery, Metabolism and Functions of NAD and NADP
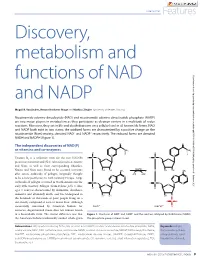
Coenzymes Features Discovery, metabolism and functions of NAD Downloaded from http://portlandpress.com/biochemist/article-pdf/37/1/9/3189/bio037010009.pdf by guest on 01 October 2021 and NADP Magali R. VanLinden, Renate Hvidsten Skoge and Mathias Ziegler (University of Bergen, Norway) Nicotinamide adenine dinucleotide (NAD) and nicotinamide adenine dinucleotide phosphate (NADP) are two major players in metabolism as they participate as electron carriers in a multitude of redox reactions. Moreover, they act in life and death decisions on a cellular level in all known life forms. NAD and NADP both exist in two states; the oxidized forms are characterized by a positive charge on the nicotinamide (Nam) moiety, denoted NAD+ and NADP+ respectively. The reduced forms are denoted NADH and NADPH (Figure 1). The independent discoveries of NAD(P) as vitamins and co-enzymes Vitamin B3 is a collective term for the two NAD(P) precursors nicotinic acid (NA) (also referred to as niacin) and Nam, as well as their corresponding ribosides. Niacin and Nam were found to be essential nutrients after severe outbreaks of pellagra (originally thought to be a new pestilence) in 18th Century Europe. Large outbreaks of pellagra occurred in North America in the early 20th Century. Pellagra (from Italian: pelle = skin; agra = sour) is characterized by dermatitis, diarrhoea, dementia and ultimately death, and was widespread in the hundreds of thousands of poor people living on a diet mostly composed of corn or maize flour. Although successfully consumed by American Indians for centuries, degerminated maize does not contain niacin in a bioavailable form. The crucial difference was that Figure 1. -

Download Download
Dorjnamjaa et al. Mongolian Geoscientist 49 (2019) 41-49 https://doi.org/10.5564/mgs.v0i49.1226 Mongolian Geoscientist Review paper New scientific direction of the bacterial paleontology in Mongolia: an essence of investigation * Dorj Dorjnamjaa , Gundsambuu Altanshagai, Batkhuyag Enkhbaatar Department of Paleontology, Institute of Paleontology, Mongolian Academy of Sciences, Ulaanbaatar 15160, Mongolia *Corresponding author. Email: [email protected] ARTICLE INFO ABSTRACT Article history: We review the initial development of Bacterial Paleontology in Mongolia and Received 10 September 2019 present some electron microscopic images of fossil bacteria in different stages of Accepted 9 October 2019 preservation in sedimentary rocks. Indeed bacterial paleontology is one the youngest branches of paleontology. It has began in the end of 20th century and has developed rapidly in recent years. The main tasks of bacterial paleontology are detailed investigation of fossil microorganisms, in particular their morphology and sizes, conditions of burial and products of habitation that are reflected in lithological and geochemical features of rocks. Bacterial paleontology deals with fossil materials and is useful in analysis of the genesis of sedimentary rocks, and sedimentary mineral resources including oil and gas. The traditional paleontology is especially significant for evolution theory, biostratigraphy, biogeography and paleoecology; however bacterial paleontology is an essential first of all for sedimentology and for theories sedimentary ore genesis or biometallogeny Keywords: microfossils, phosphorite, sedimentary rocks, lagerstatten, biometallogeny INTRODUCTION all the microorganisms had lived and propagated Bacteria or microbes preserved well as fossils in without breakdowns. Bacterial paleontological various rocks, especially in sedimentary rocks data accompanied by the data on the first origin alike natural substances. -

Phosphorus Metabolism
rology & h T ep h e N r f a o p l e a u n t r i c Raina et al., J Nephrol Therapeutic 2012, S3 u s o J Journal of Nephrology & Therapeutics DOI: 10.4172/2161-0959.S3-008 ISSN: 2161-0959 Review Article Open Access Phosphorus Metabolism Rupesh Raina1*, Gaurav Garg2, Sidharth Kumar Sethi4, Martin J Schreiber3, James F Simon3 and George Thomas3 1Fellow at Rainbow Babies and Children Hospital, Case Western Reserve, Cleveland, OH, USA 2Observer at Cleveland Clinic, Department of Hospital Medicine, Cleveland, OH, USA 3Staff at Glickman Urology and Kidney Institute, Cleveland Clinic Foundation, Cleveland, OH, USA 4Kidney and Urology Institute, Medanta, The Medicity Hospital, Gurgaon, Haryana, India Abstract Phosphorus plays a pivotal role in various biological processes. Therefore, a deeper understanding of Phosphorus Homeostasis is essential for management and treatment of conditions causing an imbalance in phosphate metabolism. The widely understood parathyroid hormone (PTH) and vitamin D axis that governs this phosphate homeostasis has been critiqued for its inability to explain a few rare genetic and acquired conditions associated with phosphate imbalance. Such conditions are characterized by normal PTH and activated vitamin D hormone. For example, Tumor Induced osteomalacia, Autosomal Dominant hypophosphatemic rickets, and X-linked hypophosphatemic rickets. Recent studies of such conditions have led to the discovery of additional factors that play an important role in phosphorus homeostasis. These phosphaturetic factors, called “Phosphatonins” include Fibroblast Growth Factor 23 (FGF-23), Fibroblast Growth Factor 7 (FGF7), Frizzled related protein 4 (FRP4), and matrix extracellular phosphoglycoprotein (MEPE).Out of these phosphatonins, FGF-23 has been extensively studied. -

The Road of Sustainable Development for Phosphate Fertilizer Industry in China
The Road of Sustainable Development for Phosphate Fertilizer Industry in China China Phosphate Industry Association Wu Xiyan 2013.9.Beijing Remarkable Achievements Phosphate fertilizer industry in China has kept rapidly developing since 2000; Ranked first in the world,it's production over US in 2005 ,achieved banlance between production and marketing in 2006,a surplus after 2007and became large exporter for Ammonium phosphate& coarse whiting ; The P fertilizer output reached 1693 t P2O5 in 2012, about 40 percent of the world; yr during 2000-2012 increased 8.1 percent; The growth in the first year of 2013 was slow, upto 8.372 million t from Jan.to June P2O5,Slightly increased 0.9%。 Product Structure of Phosphate fertilizer in China 2012, High concentration of phosphate &compound fertilizer took up 86% in 2012 from 35% in 2005 Total yield of 16.93 million t P2O5 in 2012 High concentration of phosphate &compound fertilizer took up 86.4% with 14.62 million t P2O5 ; AP output 12.60 million t P2O5 ,took up 74.4%; DAPphysical quantity14.6million t; MAP physical quantity 1328million t TSPphysical quantity1.07 million t; Phosphate group NPK physical quantity8.47million t Industrial Distribution of Phosphate fertilizer in China Two transfer basically realized:Basic fertilizer to Resources origin; Special fertilizer to end market Soil testing formula fertilization by Ministry of Agri.led enterprises produce accordingly output in Yunnan,Guizhou,Sichuan ,Hubei took up 71% overhall ; Hubei,Yunnan,Guizhou,C hongqing,Anhui ranked first -

Tricarboxylic Acid (TCA) Cycle Intermediates: Regulators of Immune Responses
life Review Tricarboxylic Acid (TCA) Cycle Intermediates: Regulators of Immune Responses Inseok Choi , Hyewon Son and Jea-Hyun Baek * School of Life Science, Handong Global University, Pohang, Gyeongbuk 37554, Korea; [email protected] (I.C.); [email protected] (H.S.) * Correspondence: [email protected]; Tel.: +82-54-260-1347 Abstract: The tricarboxylic acid cycle (TCA) is a series of chemical reactions used in aerobic organisms to generate energy via the oxidation of acetylcoenzyme A (CoA) derived from carbohydrates, fatty acids and proteins. In the eukaryotic system, the TCA cycle occurs completely in mitochondria, while the intermediates of the TCA cycle are retained inside mitochondria due to their polarity and hydrophilicity. Under cell stress conditions, mitochondria can become disrupted and release their contents, which act as danger signals in the cytosol. Of note, the TCA cycle intermediates may also leak from dysfunctioning mitochondria and regulate cellular processes. Increasing evidence shows that the metabolites of the TCA cycle are substantially involved in the regulation of immune responses. In this review, we aimed to provide a comprehensive systematic overview of the molecular mechanisms of each TCA cycle intermediate that may play key roles in regulating cellular immunity in cell stress and discuss its implication for immune activation and suppression. Keywords: Krebs cycle; tricarboxylic acid cycle; cellular immunity; immunometabolism 1. Introduction The tricarboxylic acid cycle (TCA, also known as the Krebs cycle or the citric acid Citation: Choi, I.; Son, H.; Baek, J.-H. Tricarboxylic Acid (TCA) Cycle cycle) is a series of chemical reactions used in aerobic organisms (pro- and eukaryotes) to Intermediates: Regulators of Immune generate energy via the oxidation of acetyl-coenzyme A (CoA) derived from carbohydrates, Responses. -

Food Safety Terms and Definitions Adenosine Triphosphate Testing
Food Safety Terms and Definitions Adenosine Triphosphate Testing (ATP) – ATP is found in all animal, plant, bacterial, yeast, and mold cells. It occurs in food and in microbial contamination. The ATP test uses bioluminescence to detect the presence of ATP left on a surface after cleaning to verify the removal of product that could contribute to microbiological contamination on product contact surfaces. Adulteration – To make imperfect by adding extraneous, improper, or inferior ingredients. American National Standards Institute (ANSI) - ANSI facilitates the development of American National Standards (ANS) by accrediting the procedures of standards developing organizations (SDOs). Audit – A systematic, independent, and documented examination (through observation, investigation, records review, discussions with employees of the audited entity, and, as appropriate, sampling and laboratory analysis) to assess an entity’s food safety processes and procedures. Auditor – A person who conducts an audit. Back Siphonage – The flowing back of used, contaminated, or polluted water from plumbing fixture or vessel into the pipe which feeds it; caused by reduced pressure in the pipe. Certificate of Analysis (COA) – A document containing test results that are provided to the customer by the supplier to demonstrate that product meets the defined test. Control Point – Any step in the process at which biological, chemical or physical hazards can be controlled, reduced or eliminated. Corrective Action – Documented procedures followed when a process or product deviation occurs. Critical Control Points (CCP) – A point, step, or procedure in a food process at which control can be applied and is essential to prevent or eliminate a food safety hazard or reduce such a hazard to an acceptable level. -

China Fertilizer Industry Outlook
China Fertilizer Industry Outlook CONTENTS 1. Introduction 4 2. Chinese agriculture 6 3. Development of fertilizer demand 8 4. China’s fertilizer supply and international impact 9 5. Recent developments and outlook 12 6. Implications for GPCA members 14 1. Introduction China is the most important and most to support domestic crop production. It influential country in the fertilizer business. has now grown to such a scale that it is the Its development has been dramatic. In the largest producer, consumer and exporter mid-1990s, fertilizer demand was on the of urea and ammoniated phosphates in the scale of a medium sized country, albeit world, and one of the leading producers and growing at a rapid rate. Production was consumers of potash. relatively modest and the country was an importer of most fertilizer products. In this report we provide an overview of the Chinese fertilizer industry, tracking the development of For a period it ranked among the largest agriculture and demand, together with the supply side importers of urea. However, as the Chinese and its increasing international influence. We also economy has seen massive transformation, describe our expectations for its development in the so too has its agriculture sector, and the future and the impact it has on the GCC region and its fertilizer business whose target is primarily fertilizer producing companies. 4 | China - Fertilizer Industry Outlook China - Fertilizer Industry Outlook | 5 2. Chinese agriculture To understand the development of the growth in harvested area, therefore, has been the result Chinese fertilizer industry it is important to of increased multiple cropping. -

Origins of Life in the Universe Zackary Johnson
11/4/2007 Origins of Life in the Universe Zackary Johnson OCN201 Fall 2007 [email protected] Zackary Johnson http://www.soest.hawaii.edu/oceanography/zij/education.html Uniiiversity of Hawaii Department of Oceanography Class Schedule Nov‐2Originsof Life and the Universe Nov‐5 Classification of Life Nov‐7 Primary Production Nov‐9Consumers Nov‐14 Evolution: Processes (Steward) Nov‐16 Evolution: Adaptation() (Steward) Nov‐19 Marine Microbiology Nov‐21 Benthic Communities Nov‐26 Whale Falls (Smith) Nov‐28 The Marine Food Web Nov‐30 Community Ecology Dec‐3 Fisheries Dec‐5Global Ecology Dec‐12 Final Major Concepts TIMETABLE Big Bang! • Life started early, but not at the beginning, of Earth’s Milky Way (and other galaxies formed) history • Abiogenesis is the leading hypothesis to explain the beginning of life on Earth • There are many competing theories as to how this happened • Some of the details have been worked out, but most Formation of Earth have not • Abiogenesis almost certainly occurred in the ocean 20‐15 15‐94.5Today Billions of Years Before Present 1 11/4/2007 Building Blocks TIMETABLE Big Bang! • Universe is mostly hydrogen (H) and helium (He); for Milky Way (and other galaxies formed) example –the sun is 70% H, 28% He and 2% all else! Abundance) e • Most elements of interest to biology (C, N, P, O, etc.) were (Relativ 10 produced via nuclear fusion Formation of Earth Log at very high temperature reactions in large stars after Big Bang 20‐13 13‐94.7Today Atomic Number Billions of Years Before Present ORIGIN OF LIFE ON EARTH Abiogenesis: 3 stages Divine Creation 1. -

ATP Structure and Function
ATP: Universal Currency of Cellular Energy All living things including plants, animals, birds, insects, humans need energy for the proper functioning of cells, tissues and other organ systems. As we are aware that green plants, obtain their energy from the sunlight, and animals get their energy by feeding on these plants. Energy acts as a source of fuel. We, humans, gain energy from the food we eat, but how are the energy produced and stored in our body. A living cell cannot store significant amounts of free energy. Excess free energy would result in an increase of heat in the cell, which would result in excessive thermal motion that could damage and then destroy the cell. Rather, a cell must be able to handle that energy in a way that enables the cell to store energy safely and release it for use only as needed. Living cells accomplish this by using the compound adenosine triphosphate (ATP). ATP is often called the “energy currency” of the cell, and, like currency, this versatile compound can be used to fill any energy need of the cell. How? It functions similarly to a rechargeable battery. When ATP is broken down, usually by the removal of its terminal phosphate group, energy is released. The energy is used to do work by the cell, usually by the released phosphate binding to another molecule, activating it. For example, in the mechanical work of muscle contraction, ATP supplies the energy to move the contractile muscle proteins. Recall the active transport work of the sodium-potassium pump in cell membranes.