Fact Sheet: Indigenous Women's Maternal Health
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

The Immediate and Long-Term Effects of Namibia's Colonization Process
The Immediate and Long-Term Effects of Namibia’s Colonization Process By: Jonathan Baker Honors Capstone Through Professor Taylor Politics of Sub-Saharan Africa Baker, 2 Table of Contents I. Authors Note II. Introduction III. Pre-Colonization IV. Colonization by Germany V. Colonization by South Africa VI. The Struggle for Independence VII. The Decolonization Process VIII. Political Changes- A Reaction to Colonization IX. Immediate Economic Changes Brought on by Independence X. Long Term Political Effects (of Colonization) XI. Long Term Cultural Effects XII. Long Term Economic Effects XIII. Prospects for the Future XIV. Conclusion XV. Bibliography XVI. Appendices Baker, 3 I. Author’s Note I learned such a great deal from this entire honors capstone project, that all the knowledge I have acquired can hardly be covered by what I wrote in these 50 pages. I learned so much more that I was not able to share both about Namibia and myself. I can now claim that I am knowledgeable about nearly all areas of Namibian history and life. I certainly am no expert, but after all of this research I can certainly consider myself reliable. I have never had such an extensive knowledge before of one academic area as a result of a school project. I also learned a lot about myself through this project. I learned how I can motivate myself to work, and I learned how I perform when I have to organize such a long and complicated paper, just to name a couple of things. The strange inability to be able to include everything I learned from doing this project is the reason for some of the more random appendices at the end, as I have a passion for both numbers and trivia. -

African Dialects
African Dialects • Adangme (Ghana ) • Afrikaans (Southern Africa ) • Akan: Asante (Ashanti) dialect (Ghana ) • Akan: Fante dialect (Ghana ) • Akan: Twi (Akwapem) dialect (Ghana ) • Amharic (Amarigna; Amarinya) (Ethiopia ) • Awing (Cameroon ) • Bakuba (Busoong, Kuba, Bushong) (Congo ) • Bambara (Mali; Senegal; Burkina ) • Bamoun (Cameroons ) • Bargu (Bariba) (Benin; Nigeria; Togo ) • Bassa (Gbasa) (Liberia ) • ici-Bemba (Wemba) (Congo; Zambia ) • Berba (Benin ) • Bihari: Mauritian Bhojpuri dialect - Latin Script (Mauritius ) • Bobo (Bwamou) (Burkina ) • Bulu (Boulou) (Cameroons ) • Chirpon-Lete-Anum (Cherepong; Guan) (Ghana ) • Ciokwe (Chokwe) (Angola; Congo ) • Creole, Indian Ocean: Mauritian dialect (Mauritius ) • Creole, Indian Ocean: Seychelles dialect (Kreol) (Seychelles ) • Dagbani (Dagbane; Dagomba) (Ghana; Togo ) • Diola (Jola) (Upper West Africa ) • Diola (Jola): Fogny (Jóola Fóoñi) dialect (The Gambia; Guinea; Senegal ) • Duala (Douala) (Cameroons ) • Dyula (Jula) (Burkina ) • Efik (Nigeria ) • Ekoi: Ejagham dialect (Cameroons; Nigeria ) • Ewe (Benin; Ghana; Togo ) • Ewe: Ge (Mina) dialect (Benin; Togo ) • Ewe: Watyi (Ouatchi, Waci) dialect (Benin; Togo ) • Ewondo (Cameroons ) • Fang (Equitorial Guinea ) • Fõ (Fon; Dahoméen) (Benin ) • Frafra (Ghana ) • Ful (Fula; Fulani; Fulfulde; Peul; Toucouleur) (West Africa ) • Ful: Torado dialect (Senegal ) • Gã: Accra dialect (Ghana; Togo ) • Gambai (Ngambai; Ngambaye) (Chad ) • olu-Ganda (Luganda) (Uganda ) • Gbaya (Baya) (Central African Republic; Cameroons; Congo ) • Gben (Ben) (Togo -

The International Response to Conflict and Genocide:Lessom from the Rwanda Experience
The International Response to Conflict and Genocide: Lessons from the Rwanda Experience March 1996 Published by: Steering Committee of the Joint Evaluation of Emergency Assistance to Rwanda Editor: David Millwood Cover illustrations: Kiure F. Msangi Graphic design: Designgrafik, Copenhagen Prepress: Dansk Klich‚, Copenhagen Printing: Strandberg Grafisk, Odense ISBN: 87-7265-335-3 (Synthesis Report) ISBN: 87-7265-331-0 (1. Historical Perspective: Some Explanatory Factors) ISBN: 87-7265-332-9 (2. Early Warning and Conflict Management) ISBN: 87-7265-333-7 (3. Humanitarian Aid and Effects) ISBN: 87-7265-334-5 (4. Rebuilding Post-War Rwanda) This publication may be reproduced for free distribution and may be quoted provided the source - Joint Evaluation of Emergency Assistance to Rwanda - is mentioned. The report is printed on G-print Matt, a wood-free, medium-coated paper. G-print is manufactured without the use of chlorine and marked with the Nordic Swan, licence-no. 304 022. 2 The International Response to Conflict and Genocide: Lessons from the Rwanda Experience Study 2 Early Warning and Conflict Management by Howard Adelman York University Toronto, Canada Astri Suhrke Chr. Michelsen Institute Bergen, Norway with contributions by Bruce Jones London School of Economics, U.K. Joint Evaluation of Emergency Assistance to Rwanda 3 Contents Preface 5 Executive Summary 8 Acknowledgements 11 Introduction 12 Chapter 1: The Festering Refugee Problem 17 Chapter 2: Civil War, Civil Violence and International Response 20 (1 October 1990 - 4 August -

Central African Republic Giraffe Conservation Status Report February 2020
Country Profile Central African Republic Giraffe Conservation Status Report February 2020 General statistics Size of country: 622,984 km² Size of protected areas / percentage protected area coverage: 13% Species and subspecies In 2016 the International Union for the Conservation of Nature (IUCN) completed the first detailed assessment of the conservation status of giraffe, revealing that their numbers are in peril. This was further emphasised when the majority of the IUCN recognised subspecies where assessed in 2018 – some as Critically Endangered. While this update further confirms the real threat to one of Africa’s most charismatic megafauna, it also highlights a rather confusing aspect of giraffe conservation: how many species/subspecies of giraffe are there? The IUCN currently recognises one species (Giraffa camelopardalis) and nine subspecies of giraffe (Muller et al. 2016) historically based on outdated assessments of their morphological features and geographic ranges. The subspecies are thus divided: Angolan giraffe (G. c. angolensis), Kordofan giraffe (G. c. antiquorum), Masai giraffe (G. c. tippleskirchi), Nubian giraffe (G. c. camelopardalis), reticulated giraffe (G. c. reticulata), Rothschild’s giraffe (G. c. rothschildi), South African giraffe (G. c. giraffa), Thornicroft’s giraffe (G. c. thornicrofti) and West African giraffe (G. c. peralta). However, over the past decade GCF together with their partner Senckenberg Biodiversity and Climate Research Centre (BiK-F) have performed the first-ever comprehensive DNA sampling and analysis (genomic, nuclear and mitochondrial) from all major natural populations of giraffe throughout their range in Africa. As a result, an update to the traditional taxonomy now exists. This study revealed that there are four distinct species of giraffe and likely five subspecies (Fennessy et al. -
Creating a Competitive Rwanda
Creating a Competitive Rwanda Professor Michael E. Porter Harvard Business School Kigali, Rwanda June 2007 This presentation draws on ideas from Professor Porter’s articles and books, in particular, The Competitive Advantage of Nations (The Free Press, 1990), “Building the Microeconomic Foundations of Competitiveness,” in The Global Competitiveness Report 2006 (World Economic Forum, 2006), “Clusters and the New Competitive Agenda for Companies and Governments” in On Competition (Harvard Business School Press, 1998), and ongoing research on clusters and competitiveness. No part of this publication may be reproduced, stored in a retrieval system, or transmitted in any form or by any means - electronic, mechanical, photocopying, recording, or otherwise - without the permission of Michael E. Porter. Further information on Professor Porter’s work and the Institute for Strategy and Competitiveness is available at www.isc.hbs.edu Kenya CAON 2007 June-07.ppt 1 Copyright 2007 © Professor Michael E. Porter The Changing Nature of International Competition • Fewer barriers to trade and investment Drivers • Rapidly increasing stock and diffusion of knowledge • Competitiveness upgrading in many countries • Globalization of markets • Globalization of capital investment Market • Globalization of value chains reaction • Increasing knowledge and skill intensity of competition • Value migrating to the service component of the value chain • Improving competitiveness is increasingly essential to Rwanda’s prosperity Kenya CAON 2007 June-07.ppt 2 Copyright -

Country Codes ISO 3166
COUNTRY CODES - ISO 3166-1 ISO 3166-1 encoding list of the countries which are assigned official codes It is listed in alphabetical order by the country's English short name used by the ISO 3166/MA. Numeric English short name Alpha-2 code Alpha-3 code code Afghanistan AF AFG 4 Åland Islands AX ALA 248 Albania AL ALB 8 Algeria DZ DZA 12 American Samoa AS ASM 16 Andorra AD AND 20 Angola AO AGO 24 Anguilla AI AIA 660 Antarctica AQ ATA 10 Antigua and Barbuda AG ATG 28 Argentina AR ARG 32 Armenia AM ARM 51 Aruba AW ABW 533 Australia AU AUS 36 Austria AT AUT 40 Azerbaijan AZ AZE 31 Bahamas BS BHS 44 Bahrain BH BHR 48 Bangladesh BD BGD 50 Barbados BB BRB 52 Belarus BY BLR 112 Belgium BE BEL 56 Belize BZ BLZ 84 Benin BJ BEN 204 Bermuda BM BMU 60 Bhutan BT BTN 64 Bolivia (Plurinational State of) BO BOL 68 Bonaire, Sint Eustatius and Saba BQ BES 535 Bosnia and Herzegovina BA BIH 70 Botswana BW BWA 72 Bouvet Island BV BVT 74 Brazil BR BRA 76 British Indian Ocean Territory IO IOT 86 Brunei Darussalam BN BRN 96 Bulgaria BG BGR 100 Burkina Faso BF BFA 854 Burundi BI BDI 108 Cabo Verde CV CPV 132 Cambodia KH KHM 116 Cameroon CM CMR 120 Canada CA CAN 124 1500 Don Mills Road, Suite 800 Toronto, Ontario M3B 3K4 Telephone: 416 510 8039 Toll Free: 1 800 567 7084 www.gs1ca.org Numeric English short name Alpha-2 code Alpha-3 code code Cayman Islands KY CYM 136 Central African Republic CF CAF 140 Chad TD TCD 148 Chile CL CHL 152 China CN CHN 156 Christmas Island CX CXR 162 Cocos (Keeling) Islands CC CCK 166 Colombia CO COL 170 Comoros KM COM 174 Congo CG COG -
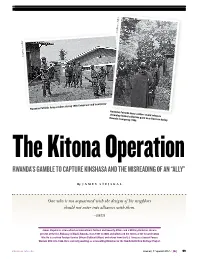
Kitona Operations: Rwanda's Gamble to Capture Kinshasa and The
Courtesy of Author Courtesy of Author of Courtesy Rwandan Patriotic Army soldiers during 1998 Congo war and insurgency Rwandan Patriotic Army soldiers guard refugees streaming toward collection point near Rwerere during Rwanda insurgency, 1998 The Kitona Operation RWANDA’S GAMBLE TO CAPTURE KINSHASA AND THE MIsrEADING OF An “ALLY” By JAMES STEJSKAL One who is not acquainted with the designs of his neighbors should not enter into alliances with them. —SUN TZU James Stejskal is a Consultant on International Political and Security Affairs and a Military Historian. He was present at the U.S. Embassy in Kigali, Rwanda, from 1997 to 2000, and witnessed the events of the Second Congo War. He is a retired Foreign Service Officer (Political Officer) and retired from the U.S. Army as a Special Forces Warrant Officer in 1996. He is currently working as a Consulting Historian for the Namib Battlefield Heritage Project. ndupress.ndu.edu issue 68, 1 st quarter 2013 / JFQ 99 RECALL | The Kitona Operation n early August 1998, a white Boeing remain hurdles that must be confronted by Uganda, DRC in 1998 remained a safe haven 727 commercial airliner touched down U.S. planners and decisionmakers when for rebels who represented a threat to their unannounced and without warning considering military operations in today’s respective nations. Angola had shared this at the Kitona military airbase in Africa. Rwanda’s foray into DRC in 1998 also concern in 1996, and its dominant security I illustrates the consequences of a failure to imperative remained an ongoing civil war the southwestern Bas Congo region of the Democratic Republic of the Congo (DRC). -

Climate Finance Readiness
Published by Climate Finance Readiness Understanding readiness to access and use climate finance effectively Insights from Namibia, Tanzania and Zambia The need to support processes that enhance the capacity of developing countries to access, allocate and spend climate finance is increasingly acknowledged by the international community. Several bilateral and multilateral initiatives have been launched to strengthen recipient country readiness to use climate finance effectively, and “readiness” activities are envisaged to be supported through the Green Climate Fund (GCF). Greater attention to issues of national policy, planning, institutional arrangements and spending capacity, it is hoped, will not only ensure that climate change and development aspirations are well aligned, but also more effectively implemented through the ensuing activities funded. Since November 2012, ODI and the African Climate Finance Hub have worked with government, private sector, and civil society stakeholders in Namibia, Zambia and Tanzania to understand these countries’ unique climate finance readiness needs. This policy brief reflects on these three country experiences to draw synthetic lessons for efforts to deliver support for climate finance readiness activities. All three country studies and an initial note outlining the analytical approach taken and early findings from this research initiative are available online at: www.odi.org.uk/climatefinancereadiness and www.giz.de/climate > Climate finance > Further information. Understanding Climate Finance Readiness -

Recommendation 3 ISO Country Code for Representation of Names of Countries
Recommendation 3 ISO COUNTRY CODE for Representation of Names of Countries At its first session, held in January 1972, the Group of The Working Party on Facilitation of International Trade Experts on Automatic Data Processing and Coding de- Procedures, cided to include in its programme of work the following Being aware of the need of an internationally agreed code task: system to represent names of countries, “To define requirements for country codes for use in Considering the International Standard ISO 3166 “Codes international trade, to be forwarded to ISO and to be for the representation of names of countries” as a suitable pursued in co-operation with it”. basis for application in international trade, It was entrusted to the secretariat to pursue this task. Recommends that the two-letter alphabetic code referred to in the International Standard ISO 3166 as “ISO AL- At a Meeting of the relevant ISO body, Working Group 2 PHA-2 Country Code”, should be used for representing of Technical Committee 46 “Documentation” in April the names of countries for purposes of International Trade 1972, it was agreed to set up a Co-ordination Committee whenever there is a need for a coded alphabetical desig- with the task to prepare proposals regarding a list of nation; entities, candidate numerical and alphabetical codes and maintenance arrangements. This Committee was com- Invites the secretariat to inform the appropriate ISO body posed of one representative each from ISO and ITU and responsible for the maintenance of ISO 3166 of any of the UNCTAD Trade Facilitation Adviser. amendments which the Working Party may suggest. -

Evolution of the EU List of Tax Havens
Evolution of the EU list of tax havens 22 February 2021 12 jurisdictions 9 jurisdictions American Samoa, Anguilla, Australia, Barbados, Botswana, Eswatini, Jamaica, Jordan, Maldives, Dominica, Fiji, Guam, Palau, Thailand, Turkey Panama, Samoa, Seychelles, Trinidad and Tobago, Vanuatu, US Virgin Islands Moved from black list to grey list Barbados Added to the black list Removed from the grey list Dominica Morocco, Namibia and Saint Lucia 6 October 12 jurisdictions 2020 10 jurisdictions American Samoa, Anguilla, Australia, Botswana, Eswatini, Jordan, Maldives, Morocco, Namibia, Barbados, Fiji, Guam, Palau, Saint Lucia, Thailand, Turkey Panama, Samoa, Seychelles, Trinidad and Tobago, Vanuatu, US Virgin Islands 9 jurisdictions Moved from grey list to black list Anguilla American Samoa, Belize, Fiji, Guam, Oman, Samoa, Trinidad and Tobago, Vanuatu, Added to the black list Removed from the grey list US Virgin Islands Barbados Bosnia and Herzegovina, Mongolia Removed from the blacklist Cayman Islands, Oman Taxation and Customs Union 18 February 12 jurisdictions 2020 13 jurisdictions American Samoa, Cayman Anguilla, Australia, Bosnia and Herzegovina, Botswana, Eswatini, Jordan, Islands, Fiji, Guam, Palau, Maldives, Morocco, Mongolia, Namibia, Saint Lucia, Thailand and Turkey Panama, Samoa, Seychelles, Oman, Trinidad and Tobago, Vanuatu, US Virgin Islands Moved from grey list to black list Cayman Islands, Palau and Seychelles Added to the black list Removed from the grey list Panama Antigua and Barbuda, Armenia, Bahamas, Barbados, Belize, Bermuda, -

Languages, Countries and Codes (LCCTM)
Date: September 2017 OBJECT MANAGEMENT GROUP Languages, Countries and Codes (LCCTM) Version 1.0 – Beta 2 _______________________________________________ OMG Document Number: ptc/2017-09-04 Standard document URL: http://www.omg.org/spec/LCC/1.0/ Normative Machine Consumable File(s): http://www.omg.org/spec/LCC/Languages/LanguageRepresentation.rdf http://www.omg.org/spec/LCC/201 708 01/Languages/LanguageRepresentation.rdf http://www.omg.org/spec/LCC/Languages/ISO639-1-LanguageCodes.rdf http://www.omg.org/spec/LCC/201 708 01/Languages/ISO639-1-LanguageCodes.rdf http://www.omg.org/spec/LCC/Languages/ISO639-2-LanguageCodes.rdf http://www.omg.org/spec/LCC/201 708 01/Languages/ISO639-2-LanguageCodes.rdf http://www.omg.org/spec/LCC/Countries/CountryRepresentation.rdf http://www.omg.org/spec/LCC/20170801/Countries/CountryRepresentation.rdf http://www.omg.org/spec/LCC/Countries/ISO3166-1-CountryCodes.rdf http://www.omg.org/spec/LCC/201 708 01/Countries/ISO3166-1-CountryCodes.rdf http://www.omg.org/spec/LCC/Countries/ISO3166-2-SubdivisionCodes.rdf http://www.omg.org/spec/LCC/201 708 01/Countries/ISO3166-2-SubdivisionCodes.rdf http://www.omg.org/spec/LCC/Countries/ UN-M49-RegionCodes .rdf http://www.omg.org/spec/LCC/201 708 01/Countries/ UN-M49-Region Codes.rdf http://www.omg.org/spec/LCC/201 708 01/Languages/LanguageRepresentation.xml http://www.omg.org/spec/LCC/201 708 01/Languages/ISO639-1-LanguageCodes.xml http://www.omg.org/spec/LCC/201 708 01/Languages/ISO639-2-LanguageCodes.xml http://www.omg.org/spec/LCC/201 708 01/Countries/CountryRepresentation.xml http://www.omg.org/spec/LCC/201 708 01/Countries/ISO3166-1-CountryCodes.xml http://www.omg.org/spec/LCC/201 708 01/Countries/ISO3166-2-SubdivisionCodes.xml http://www.omg.org/spec/LCC/201 708 01/Countries/ UN-M49-Region Codes. -
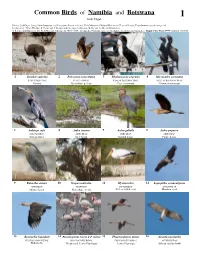
Common Birds of Namibia and Botswana 1 Josh Engel
Common Birds of Namibia and Botswana 1 Josh Engel Photos: Josh Engel, [[email protected]] Integrative Research Center, Field Museum of Natural History and Tropical Birding Tours [www.tropicalbirding.com] Produced by: Tyana Wachter, R. Foster and J. Philipp, with the support of Connie Keller and the Mellon Foundation. © Science and Education, The Field Museum, Chicago, IL 60605 USA. [[email protected]] [fieldguides.fieldmuseum.org/guides] Rapid Color Guide #584 version 1 01/2015 1 Struthio camelus 2 Pelecanus onocrotalus 3 Phalacocorax capensis 4 Microcarbo coronatus STRUTHIONIDAE PELECANIDAE PHALACROCORACIDAE PHALACROCORACIDAE Ostrich Great white pelican Cape cormorant Crowned cormorant 5 Anhinga rufa 6 Ardea cinerea 7 Ardea goliath 8 Ardea pupurea ANIHINGIDAE ARDEIDAE ARDEIDAE ARDEIDAE African darter Grey heron Goliath heron Purple heron 9 Butorides striata 10 Scopus umbretta 11 Mycteria ibis 12 Leptoptilos crumentiferus ARDEIDAE SCOPIDAE CICONIIDAE CICONIIDAE Striated heron Hamerkop (nest) Yellow-billed stork Marabou stork 13 Bostrychia hagedash 14 Phoenicopterus roseus & P. minor 15 Phoenicopterus minor 16 Aviceda cuculoides THRESKIORNITHIDAE PHOENICOPTERIDAE PHOENICOPTERIDAE ACCIPITRIDAE Hadada ibis Greater and Lesser Flamingos Lesser Flamingo African cuckoo hawk Common Birds of Namibia and Botswana 2 Josh Engel Photos: Josh Engel, [[email protected]] Integrative Research Center, Field Museum of Natural History and Tropical Birding Tours [www.tropicalbirding.com] Produced by: Tyana Wachter, R. Foster and J. Philipp,