Respiratory System
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Te2, Part Iii
TERMINOLOGIA EMBRYOLOGICA Second Edition International Embryological Terminology FIPAT The Federative International Programme for Anatomical Terminology A programme of the International Federation of Associations of Anatomists (IFAA) TE2, PART III Contents Caput V: Organogenesis Chapter 5: Organogenesis (continued) Systema respiratorium Respiratory system Systema urinarium Urinary system Systemata genitalia Genital systems Coeloma Coelom Glandulae endocrinae Endocrine glands Systema cardiovasculare Cardiovascular system Systema lymphoideum Lymphoid system Bibliographic Reference Citation: FIPAT. Terminologia Embryologica. 2nd ed. FIPAT.library.dal.ca. Federative International Programme for Anatomical Terminology, February 2017 Published pending approval by the General Assembly at the next Congress of IFAA (2019) Creative Commons License: The publication of Terminologia Embryologica is under a Creative Commons Attribution-NoDerivatives 4.0 International (CC BY-ND 4.0) license The individual terms in this terminology are within the public domain. Statements about terms being part of this international standard terminology should use the above bibliographic reference to cite this terminology. The unaltered PDF files of this terminology may be freely copied and distributed by users. IFAA member societies are authorized to publish translations of this terminology. Authors of other works that might be considered derivative should write to the Chair of FIPAT for permission to publish a derivative work. Caput V: ORGANOGENESIS Chapter 5: ORGANOGENESIS -

Embryology of Branchial Region
TRANSCRIPTIONS OF NARRATIONS FOR EMBRYOLOGY OF THE BRANCHIAL REGION Branchial Arch Development, slide 2 This is a very familiar picture - a median sagittal section of a four week embryo. I have actually done one thing correctly, I have eliminated the oropharyngeal membrane, which does disappear sometime during the fourth week of development. The cloacal membrane, as you know, doesn't disappear until the seventh week, and therefore it is still intact here, but unlabeled. But, I've labeled a couple of things not mentioned before. First of all, the most cranial part of the foregut, that is, the part that is cranial to the chest region, is called the pharynx. The part of the foregut in the chest region is called the esophagus; you probably knew that. And then, leading to the pharynx from the outside, is an ectodermal inpocketing, which is called the stomodeum. That originally led to the oropharyngeal membrane, but now that the oropharyngeal membrane is ruptured, the stomodeum is a pathway between the amniotic cavity and the lumen of the foregut. The stomodeum is going to become your oral cavity. Branchial Arch Development, slide 3 This is an actual picture of a four-week embryo. It's about 5mm crown-rump length. The stomodeum is labeled - that is the future oral cavity that leads to the pharynx through the ruptured oropharyngeal membrane. And I've also indicated these ridges separated by grooves that lie caudal to the stomodeum and cranial to the heart, which are called branchial arches. Now, if this is a four- week old embryo, clearly these things have developed during the fourth week, and I've never mentioned them before. -

Insect Digestion
INSECT DIGESTION Zoo 514 Dr. Reem Alajmi Insect digestive system The alimentary canal is concerned with digestion and absorption of food stuffs. Different parts of the gut are concerned with different aspects of these functions. In fluid feeding insects digestion begin before the food is ingested through the injection or regurgitation of enzymes on to the food . In general it occurs in the mid gut (most of the enzymes are produced). The enzymes break down the complex substances in the food into simple substances which can be absorbed and assimilated. Enzymes function optimally only within limited range of pH and temperature. Absorption is passive process in some cases , but in others active transport occurs. Absorption of water is important in terrestrial insects , rectum remove water from faeces. • Insects of different groups consume astonishing variety of foods, including watery xylem sap, vertebrate blood, dry wood, bacteria and algae and the internal tissues of other insects. • Types of mouth parts correlates with the diets of insect. Also gut structure and function affected by nutrient composition of the food eaten by insect. • Insects that take solid food typically have a wide, straight, short gut with strong musculature and obvious protection from abrasion (especially in the midgut, which has no cuticular lining). • These features are most obvious in solid-feeders with rapid throughput of food, as in many insects and plant-feeding caterpillars In contrast, insects feeding on blood, sap or nectar usually have long, narrow, convoluted guts to allow maximal contact with the liquid food; here, protection from abrasion is unnecessary. The most obvious gut specialization of liquid-feeders is a mechanism for removing excess water to concentrate nutrient substances prior to digestion, as seen in hemipterans. -

Embryology, Comparative Anatomy, and Congenital Malformations of the Gastrointestinal Tract
Edorium J Anat Embryo 2016;3:39–50. Danowitz et al. 39 www.edoriumjournals.com/ej/ae REVIEW ARTICLE PEER REVIEWED | OPEN ACCESS Embryology, comparative anatomy, and congenital malformations of the gastrointestinal tract Melinda Danowitz, Nikos Solounias ABSTRACT Human digestive development is an essential topic for medical students and physicians, Evolutionary biology gives context to human and many common congenital abnormalities embryonic digestive organs, and demonstrates directly relate to gastrointestinal embryology. how structural adaptations can fit changing We believe this comprehensive review of environmental requirements. Comparative gastrointestinal embryology and comparative anatomy is rarely included in the medical anatomy will facilitate a better understanding of school curriculum. However, its concepts gut development, congenital abnormalities, and facilitate a deeper comprehension of anatomy adaptations to various evolutionary ecological and development by putting the morphology conditions. into an evolutionary perspective. Features of gastrointestinal development reflect the transition Keywords: Anatomy education, Digestive, Embry- from aquatic to terrestrial environments, such as ology, Gastrointestinal tract the elongation of the colon in land vertebrates, allowing for better water reabsorption. In How to cite this article addition, fishes exhibit ciliary transport in the esophagus, which facilitates particle transport in Danowitz M, Solounias N. Embryology, comparative water, whereas land mammals develop striated anatomy, and congenital malformations of the and smooth esophageal musculature and utilize gastrointestinal tract. Edorium J Anat Embryo peristaltic muscle contractions, allowing for 2016;3:39–50. better voluntary control of swallowing. The development of an extensive vitelline drainage system to the liver, which ultimately creates Article ID: 100014A04MD2016 the adult hepatic portal system allows for the evolution of complex hepatic metabolic ********* functions seen in many vertebrates today. -
DIGESTIVE SYSTEM Generalized Insect Alimentary Tract the Digestive System Is Just a Tube Within a Surrounding Tube Called the Body
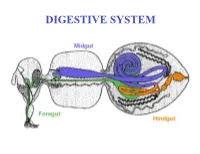
DIGESTIVE SYSTEM Generalized insect alimentary tract The digestive system is just a tube within a surrounding tube called the body. It starts with a mouth and ends with the anus. What goes on in between depends on the insect, its life stage and what it eats. The origin of the digestive tract. At the anterior pole of the embryo an indentation forms that will be the foregut or stomodeum. At the other end a similar thing occurs and the proctodeum or hindgut is formed. Both are lined by cuticle. They both are of ectodermal origin while the midgut is of mesodermal origin and is also called the mesenteron. This different origin of the midgut from the endoderm and not the ecotoderm probably explains why it is not lined with cuticle Anterior midgut invagination. In the bottom photo note the invagination starting forming the ventral furrow lumen (VF) MIDGUT FORMATION IN THE EMBRYO PMG in the above embryo shows the posterior midgut invagination cup where the posterior invagination shown in the drawing on the right will take place. Photo of Drosophila embryo. Hindgut invagination DIGESTIVE SYSTEM The digestive tract not only aids in obtaining, processing and digesting food molecules - It is the largest endocrine tissue in both humans and insects. The digestive system is involved in: 1. Obtaining food 2. Mechanically breaking it down into smaller particles that facilitate digestive enzymes acting on them 3. Enzymatic breakdown of larger food molecules into molecules that can pass through the digestive tract (midgut) and enter the hemolymph 4. Produces molecules or MESSENGERS (eg. -
The Missing Link CASE REPORT
CASE REPORT 531 The missing link J. Maus1, S. Naegels1, H. Slabbynck2, L. De Waele1, I. Ruytjens1 (1) ZNA Middelheim, Department of Gastro-enterology ; (2) ZNA Middelheim, Department of Pneumology. Abstract We present a case of a 28-year old woman who presented with bizarre wheezing breath sounds on expiration and dysphagia, with unexplained significant dilation of the esophagus mimicking achalasia finally leading to the diagnosis of a very small congenital tracheoesophageal fistula (TEF). Congenital TEF is usually detected shortly after birth and is typically accompanied by esophageal atresia. Congenital TEF without esophageal atresia (H-type fistula) can be missed in early life and diagnosis may be postponed until adulthood due to subtle symptoms. Diagnosis is usually based upon a combination of esophagoscopy, bronchoscopy, barium esophagography and CT-scan. The only clue can be the finding of a significant dilated aperistaltic esophagus, with subsequent more detailed CT reconstruction revealing a very tiny H-type TEF. It is important to raise the awareness of small H-type TEF as a possible cause of achalasia-like esophageal dilation in adulthood and of very unusual and bizarre wheezing breath sounds. (Acta gastroenterol. belg., 2018, 81, 531-533). Key words : adult ; congenital ; tracheoesophageal fistula ; H-type. Introduction Most patients with congenital TEF are diagnosed shortly after birth or in early life due to frequent association with esophageal atresia which leads to life-threatening complications and warrants immediate surgery. (1) H-type TEF, where esophageal atresia is absent, is rare and diagnosis may be postponed until adulthood due to subtle symptoms and physician unfamiliarity (2). -

Gastroesophageal Reflux: Anatomy and Physiology
26th Annual Scientific Conference | May 1-4, 2017 | Hollywood, FL Gastroesophageal Reflux: Anatomy and Physiology Amy Lowery Carroll, MSN, RN, CPNP- AC, CPEN Children’s of Mississippi at The University of Mississippi Medical Center Jackson, Mississippi Disclosure Information I have no disclosures. Objectives • Review embryologic development of GI system • Review normal anatomy and physiology of esophagus and stomach • Review pathophysiology of Gastroesophageal Reflux 1 26th Annual Scientific Conference | May 1-4, 2017 | Hollywood, FL Embryology of the Gastrointestinal System GI and Respiratory systems are derived from the endoderm after cephalocaudal and lateral folding of the yolk sack of the embryo Primitive gut can be divided into 3 sections: Foregut Extends from oropharynx to the liver outgrowth Thyroid, esophagus, respiratory epithelium, stomach liver, biliary tree, pancreas, and proximal portion of duodenum Midgut Liver outgrowth to the transverse colon Develops into the small intestine and proximal colon Hindgut Extends from transverse colon to the cloacal membrane and forms the remainder of the colon and rectum Forms the urogenital tract Embryology of the Gastrointestinal System Respiratory epithelium appears as a bud of the esophagus around 4th week of gestation Tracheoesophageal septum develops to separate the foregut into ventral tracheal epithelium and dorsal esophageal epithelium Esophagus starts out short and lengthens to final extent by 7 weeks Anatomy and Physiology of GI System Upper GI Tract Mouth Pharynx Esophagus Stomach -

Embryology and Teratology in the Curricula of Healthcare Courses
ANATOMICAL EDUCATION Eur. J. Anat. 21 (1): 77-91 (2017) Embryology and Teratology in the Curricula of Healthcare Courses Bernard J. Moxham 1, Hana Brichova 2, Elpida Emmanouil-Nikoloussi 3, Andy R.M. Chirculescu 4 1Cardiff School of Biosciences, Cardiff University, Museum Avenue, Cardiff CF10 3AX, Wales, United Kingdom and Department of Anatomy, St. George’s University, St George, Grenada, 2First Faculty of Medicine, Institute of Histology and Embryology, Charles University Prague, Albertov 4, 128 01 Prague 2, Czech Republic and Second Medical Facul- ty, Institute of Histology and Embryology, Charles University Prague, V Úvalu 84, 150 00 Prague 5 , Czech Republic, 3The School of Medicine, European University Cyprus, 6 Diogenous str, 2404 Engomi, P.O.Box 22006, 1516 Nicosia, Cyprus , 4Department of Morphological Sciences, Division of Anatomy, Faculty of Medicine, C. Davila University, Bucharest, Romania SUMMARY Key words: Anatomy – Embryology – Education – Syllabus – Medical – Dental – Healthcare Significant changes are occurring worldwide in courses for healthcare studies, including medicine INTRODUCTION and dentistry. Critical evaluation of the place, tim- ing, and content of components that can be collec- Embryology is a sub-discipline of developmental tively grouped as the anatomical sciences has biology that relates to life before birth. Teratology however yet to be adequately undertaken. Surveys (τέρατος (teratos) meaning ‘monster’ or ‘marvel’) of teaching hours for embryology in US and UK relates to abnormal development and congenital medical courses clearly demonstrate that a dra- abnormalities (i.e. morphofunctional impairments). matic decline in the importance of the subject is in Embryological studies are concerned essentially progress, in terms of both a decrease in the num- with the laws and mechanisms associated with ber of hours allocated within the medical course normal development (ontogenesis) from the stage and in relation to changes in pedagogic methodol- of the ovum until parturition and the end of intra- ogies. -
Development of Respiratory System
Development of respiratory system Respiratory block-Anatomy-Lecture 5 Editing file Color guide : Only in boys slides in Green Only in girls slides in Purple Objectives important in Red Doctor note in Blue Extra information in Grey ➔ Identify the development of the laryngotracheal (respiratory) diverticulum. ➔ Identify the development of the larynx. ➔ Identify the development of the trachea. ➔ Identify the development of the bronchi & Lungs. ➔ Describe the periods of the maturation of the lung. ➔ Identify the most congenital anomaly 3 Respiratory system Upper respiratory Lower respiratory tract tract Nasal cavity & Nose paranasal Laryngopharynx Larynx Trachea Bronchi Lungs sinuses Development of the respiratory tract 4 The endoderm & Begins during the 4th week of Development of longitudinal Proximal & distal parts of the surrounding splanchnic development tracheoesophageal septum respiratory diverticulum mesoderm ▹ Divides the diverticulum ▹ Begins as a median ▹ The proximal part of the ▹ The endoderm lining the into: outgrowth (laryngotracheal respiratory diverticulum laryngotracheal ▸ Dorsal portion*: groove) from the caudal part remains tubular and forms diverticulum (respiratory primordium (in the of the ventral wall of the larynx & trachea. diverticulum) gives rise to earliest stage of primitive pharynx (foregut). ▹ The distal end of the the: development) of the ▹ The groove invaginates (fold diverticulum dilates to form ▸ Epithelium & glands oropharynx & within itself) and forms lung bud, which divides to of the respiratory esophagus. laryngotracheal give rise to 2 lung buds tract. ▸ Ventral portion*: (respiratory) diverticulum. (primary bronchial buds). ▹ The surrounding splanchnic primordium (=give mesoderm gives rise to the: rise) of larynx, ▸ Connective tissue, trachea, bronchi & cartilage & smooth lungs. muscles of the respiratory tract. * Remember that the larynx, trachea, bronchi & lungs lie anteriorly while the oropharynx & esophagus lie posteriorly. -

Gross Anatomy of Abdominal Oesophagus, Stomach, Duodenum
Development & histology of GIT & clinical considerations MASUD M. A. (BSC, MSC ANATOMY, PGDE) DEPARTMENT OF HUMAN ANATOMY KAMPALA INTERNATIONAL UNIVERSITY, WESTERN CAMPUS Objectives At the end of the lecture, student should be able to: • State the primordial of the guts and its associated glands/organs • List the derivatives of the guts: foregut, midgut and hindgut • Explain the development of GIT and its associated glands/organs • Outline and explain congenital anomalies in the development of the digestive system • State and describe the basic histological structures in the GIT • Identify histopathological GIT tissues on photomicrographs 2 Overview • during 4th week, the primordial gut is formed • cranial, caudal and lateral fold incorporate the dorsal part of umbilical vesicle • initially, the primordial gut is closed at its cranial and caudal ends by: • Oropharyngeal membrane Heart Pharynx • Cloacal membrane Cloaca Hindgut 3 Cont’d • The endoderm of the primordial gut gives rise to: • most of the gut • Epithelium and • Glands • The ectoderm of the stomodeum and proctodeum gives rise to: • epithelium at the cranial and caudal ends of GIT • The mesenchyme around the primordial gut gives rise to: • muscles of the GIT 4 Foregut Pharynx Heart The derivatives of the foregut are: • Primordial pharynx and its derivatives • Lower respiratory system • Esophagus and stomach • Duodenum and distal opening of bile duct • Liver, biliary apparatus and pancreas Cloaca Hindgut 5 Development of Esophagus • Develops from the foregut immediately caudal -

The Respiratory System
Embryology18 Dr.Ban The respiratory system Respiratory system development is a highly coordinated and complex process it’s development is tightly associated with the digestive system from the beginning.The respiratory tract is divided anatomically into 2 main parts: A-upper respiratory tract, consisting of the nose, nasal cavity and the pharynx B-lower respiratory tract consisting of the larynx, trachea, bronchi and the lungs. The pharynx is the part of the throat behind the mouth and nasal cavity, and above the esophagus and larynx. In humans, the pharynx is part of the digestive system and the conducting zone of the respiratory system. The conducting zone which also includes the nostrils of the nose, the larynx, trachea, bronchi, and bronchioles filters, warms and moistens air and conducts it into the lungs). The human pharynx is divided into three sections: . nasopharynx . oropharynx . laryngopharynx 1 Embryology18 Dr.Ban The larynx The internal lining of the larynx originates from endoderm, but the cartilages and muscles originate from mesenchyme of the 4th and 6th pharyngeal arches. As a result of rapid proliferation of this mesenchyme, the laryngeal orifice changes in appearance from a sagital slit to a T-shaped opening. When the mesenchyme of the two arches transforms into the thyroid, cricoid and arytenoid cartilages the adult shape of the laryngeal orifice can be recognized. The laryngeal epithelium proliferates rapidly, resulting in a temporary occlusion of the lumen. Subsequently, vacuolization and recanalization produces a pair of lateral recesses, the laryngeal ventricles that are bounded by folds of tissue that differentiate into the false and true vocal cords. -

Facial and Palatal Development
11. FACIAL AND PALATAL DEVELOPMENT Letty Moss-Salentijn DDS, PhD Dr. Edwin S.Robinson Professor of Dentistry (in Anatomy and Cell Biology) E-mail: [email protected] READING ASSIGNMENT: Larsen 3rd edition: p.352; pp.365-371; 398-404. SUMMARY: The external human face develops between the 4th and 6th weeks of embryonic development. Facial swellings arise on the frontonasal process (2 medial nasal and 2 lateral nasal processes) and the first pharyngeal arch (2 mandibular and 2 maxillary processes). By a process of merging and some localized fusion these processes come together to form the continuous surfaces of the external face. The primary palate is formed in this period by fusion/merging of the medial nasal and maxillary processes. Subsequently, between 6th and 12th embryonic/fetal weeks, the secondary palate is formed as the result of fusion between palatal processes growing from the oral surfaces of the maxillary processes. Each merging and fusion site is also the site of a potential facial or palatal cleft. LEARNING OBJECTIVES You should be able to: a. Demonstrate on a frontal image of a human face those parts of the face that are formed by contributions from the frontonasal process and those that are formed by contributions from the first pharyngeal arch. b. Describe the following as to site, composition, time of appearance, and fate: oropharyngeal membrane, oronasal membrane. c. List the derivatives of the four pairs of facial processes and the pair of palatal processes. d. Describe the development of the nose and primary palate. e. Explain the differences between the processes of merging and fusion.