2018 Endovascular Reimbursement Coding Fact Sheet
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Coding for Angioplasty & Stent Procedures
Coding for Angioplasty & Stent Procedures July 2020 Jennifer Bash, RHIA, CIRCC, RCCIR, CPC, RCC Director of Coding Education Agenda • Introduction • Definitions • General Coding Guidelines • Presenting Problems/Medical Necessity for Angioplasty & Stent • General Angioplasty & Stent Procedures • Cervicocerebral Procedures • Lower Extremity Procedures Disclaimer The information presented is based on the experience and interpretation of the presenters. Though all of the information has been carefully researched and checked for accuracy and completeness, ADVOCATE does not accept any responsibility or liability with regard to errors, omissions, misuse or misinterpretation. CPT codes are trademark and copyright of the American Medical Association. Resources •AMA •CMS • ACR/SIR • ZHealth Publishing Angioplasty & Stent Procedures Angioplasty Angioplasty, also known as balloon angioplasty and percutaneous transluminal angioplasty, is a minimally invasive endovascular procedure used to widen narrowed or obstructed arteries or veins, typically to treat arterial atherosclerosis. Vascular Stent A stent is a tiny tube placed into the artery or vein used to treat vessel narrowing or blockage. Most stents are made of a metal or plastic mesh-like material. General Angioplasty & Stent Coding Guidelines • Angioplasty is not separately billable when done with a stent • Pre-Dilatation • PTA converted to Stent • Prophylaxis • EXCEPTION-Complication extending to a different vessel • Coded per vessel • Codes include RS&I • Territories • Hierarchy General Angioplasty -

Deep Venous Thrombosis with Suspected Pulmonary Embolism
Thoracic Imaging Peter A. Loud, MD Deep Venous Thrombosis Douglas S. Katz, MD Dennis A. Bruce, MD with Suspected Pulmonary Donald L. Klippenstein, MD Zachary D. Grossman, MD Embolism: Detection with Combined CT Venography Index terms: Computed tomography (CT), 1 angiography, 9*.129142, and Pulmonary Angiography 9*.12915, 9*.12916 Embolism, pulmonary, 60.72 Pulmonary angiography, 944.12914, 944.12915, 944.12916 PURPOSE: To determine the frequency and location of deep venous thrombosis at Veins, thrombosis, 9*.751, 9*.12914 computed tomographic (CT) venography after CT pulmonary angiography in a large series of patients clinically suspected of having pulmonary embolism and to Radiology 2001; 219:498–502 compare the accuracy of CT venography with lower-extremity venous sonography. Abbreviation: MATERIALS AND METHODS: Venous phase images were acquired from the DVT ϭ deep venous thrombosis diaphragm to the upper calves after completion of CT pulmonary angiography in 650 patients (373 women, 277 men; age range, 18–99 years; mean age, 63 years) 1 From the Department of Radiology, to determine the presence and location of deep venous thrombosis. Results of CT Roswell Park Cancer Institute, Elm and Carlton Sts, Buffalo, NY 14263 (P.A.L., venography were compared with those of bilateral lower-extremity venous sonog- D.L.K., Z.D.G.), and the Department raphy in 308 patients. of Radiology, Winthrop University Hospital, Mineola, NY (D.S.K., D.A.B.). RESULTS: A total of 116 patients had pulmonary embolism and/or deep venous From the 1999 RSNA scientific assem- thrombosis, including 27 patients with pulmonary embolism alone, 31 patients with bly. -

Coronary Angiogram, Angioplasty and Stent Placement
Page 1 of 6 Coronary Angiogram, Angioplasty and Stent Placement A Patient’s Guide Page 2 of 6 What is coronary artery disease? What is angioplasty and a stent? Coronary artery disease means that you have a If your doctor finds a blocked artery during your narrowed or blocked artery. It is caused by the angiogram, you may need an angioplasty (AN-jee- buildup of plaque (fatty material) inside the artery o-plas-tee). This is a procedure that uses a small over many years. This buildup can stop blood from inflated balloon to open a blocked artery. It can be getting to the heart, causing a heart attack (the death done during your angiogram test. of heart muscle cells). The heart can then lose some of its ability to pump blood through the body. Your doctor may also place a stent at this time. A stent is a small mesh tube that is placed into an Coronary artery disease is the most common type of artery to help keep it open. Some stents are coated heart disease. It is also the leading cause of death for with medicine, some are not. Your doctor will both men and women in the United States. For this choose the stent that is right for you. reason, it is important to treat a blocked artery. Angioplasty and stent Anatomy of the Heart 1. Stent with 2. Balloon inflated 3. Balloon balloon inserted to expand stent. removed from into narrowed or expanded stent. What is a coronary angiogram? blocked artery. A coronary angiogram (AN-jee-o-gram) is a test that uses contrast dye and X-rays to look at the blood vessels of the heart. -
Spring Programme 2011
Faculty of Radiologists Royal College of Surgeons in Ireland Combined Spring Meeting 8th & 9 th April 2011 Venue: Castlemartyr Hotel, Co. Cork. Programme Faculty of Radiologists, Royal College of Surgeons in Ireland CPD Credits Awarded: 5 Royal College of Radiologists credits are applied for. Friday 8 th April 2011 3.30-4.30pm Registration 4.30-5.30pm Stroke in 2011, Moderator: Dr. Ian Kelly, Waterford Regional Hospital 4.30-5.00pm Acute Stoke Imaging. Dr Noel Fanning, Cork University Hospital, Cork 5.00-5.30pm Stroke: A clinical perspective. Dr. George Pope, John Radcliffe Hospitals, Oxford 5.30-6.30pm Moderator: Dr. Adrian Brady, Dean, Faculty of Radiologists Belfast to Bosnia and Autopsy to Virtopsy Dr. Jack Crane, State Pathologist, NI 8pm Dinner Saturday 9 th April 2011 8.30-9.00am Registration 9.00-10.00am Liver hour. Moderator: Dr John Feeney, AMNCH, Dublin 9.00-9.30am Liver imaging pre metastatectomy. Dr. Peter MacEneaney, Mercy University Hospital, Cork 9.30-10.00am Parenchymal and focal liver biopsy - when and how. Dr Stephen J Skehan St Vincent's University Hospital, Dublin 10.00-11.00am Paediatric Hour. Moderator: Dr. Stephanie Ryan, The Children’s University Hospital Temple Street, Dublin 10.00-10.30am Paediatric Abdominal Emergencies. Dr Eoghan Laffan, The Children’s, University Hospital Temple Street, Dublin 10.30-11.00am Non Accidental Injury. Dr Conor Bogue, Cork University Hospital, Cork 11.00-11.30am Tea/Coffee Break and Poster Exhibition 11.30-12.30pm MSK Hour. Moderator: Dr Orla Buckley, AMNCH, Dublin 11.30-12.00pm Image guided joint interventions. -
CT Venography: Technique and Indications
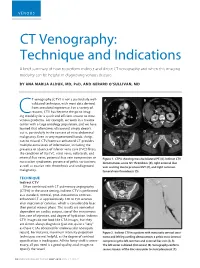
VENOUS CT Venography: Technique and Indications A brief summary of how to perform indirect and direct CT venography and when this imaging modality can be helpful in diagnosing venous disease. BY ANA MARIJA ALDUK, MD, PHD, AND GERARD O’SULLIVAN, MD T venography (CTV) is not a particularly well- A B validated technique, with most data derived from anecdotal experience. For a variety of reasons, CTV has become the go-to imag- Cing modality for a quick and efficient answer to most venous problems. For example, we work in a trauma center with a large oncology population, and we have learned that oftentimes ultrasound simply doesn’t cut it, particularly in the context of intra-abdominal C D malignancy. Even in very experienced hands, things can be missed. CTV/contrast-enhanced CT provides multiple extra levels of information, including the presence or absence of inferior vena cava (IVC) filters; the condition of the IVC, renal veins, collaterals, and internal iliac veins; potential iliac vein compression or Figure 1. CTPA showing massive bilateral PE (A). Indirect CTV nutcracker syndromes; presence of pelvic varicosities; demonstrates acute IVC thrombosis (B), right external iliac as well as ovarian vein thrombosis and undiagnosed vein scarring due to previous DVT (C), and right common malignancy. femoral vein thrombosis (D). TECHNIQUE A C Indirect CTV Often combined with CT pulmonary angiography (CTPA) in the acute setting, indirect CTV is performed as a standard, nonoral, post–intravenous contrast- enhanced CT at approximately 120 to 150 seconds after injection of contrast, which is considerably later than portal venous phase. -

2Nd Quarter 2001 Medicare Part a Bulletin
In This Issue... From the Intermediary Medical Director Medical Review Progressive Corrective Action ......................................................................... 3 General Information Medical Review Process Revision to Medical Record Requests ................................................ 5 General Coverage New CLIA Waived Tests ............................................................................................................. 8 Outpatient Hospital Services Correction to the Outpatient Services Fee Schedule ................................................................. 9 Skilled Nursing Facility Services Fee Schedule and Consolidated Billing for Skilled Nursing Facility (SNF) Services ............. 12 Fraud and Abuse Justice Recovers Record $1.5 Billion in Fraud Payments - Highest Ever for One Year Period ........................................................................................... 20 Bulletin Medical Policies Use of the American Medical Association’s (AMA’s) Current Procedural Terminology (CPT) Codes on Contractors’ Web Sites ................................................................................. 21 Outpatient Prospective Payment System January 2001 Update: Coding Information for Hospital Outpatient Prospective Payment System (OPPS) ......................................................................................................................... 93 he Medicare A Bulletin Providers Will Be Asked to Register Tshould be shared with all to Receive Medicare Bulletins and health care -

(MRA) and Magnetic Resonance Venography (MRV) Medical Policy
Magnetic Resonance Angiography (MRA) and Magnetic Resonance Venography (MRV) Medical Policy The content of this document is used by plans that do not utilize NIA review. Service: Magnetic Resonance Angiography (MRA) and Magnetic Resonance Venography (MRV) PUM 250-0027-1712 Medical Policy Committee Approval 12/11/2020 Effective Date 01/01/2021 Prior Authorization Needed Yes Description: Magnetic Resonance Angiography (MRA) and Magnetic Resonance Venography (MRV) use Magnetic resonance imaging (MRI) technology to produce detailed 2-dimensional or 3- dimensional images of the vascular system and may be tailored to assess arteries or veins. It is often used for vascular conditions where other types of imaging are considered inferior or contraindicated, and to decrease risk of cumulative radiation exposure and often instead of invasive procedures. Indications of Coverage: A. MRA/MRV is considered medically necessary for the anatomical regions listed below when the specific indications or symptoms described are documented: 1. Head/Brain: a. Suspected intracranial aneurysm (ICA) or arteriovenous malformation (AVM). Any of the following: 1. Acute severe headache, severe exertional headache, or sudden onset of explosive headache, in individuals with signs / symptoms highly suggestive of a leaking/ruptured internal carotid artery or arteriovenous malformation. 2. Known subarachnoid hemorrhage or diagnosis of spontaneous intracerebral hemorrhage with concern for underlying vascular abnormality. 3. Suspected arteriovenous malformation (AVM) or dural AV fistula in an individual with prior indeterminate imaging study 4. Thunderclap headache with question of underlying vascular abnormality AND prior negative workup to include EITHER i. negative brain MRI, OR ii. Negative brain CT and negative lumbar puncture Page 1 of 15 5. -

Optos 200Tx and Heidelberg Spectralis
EXPERIMENTAL AND THERAPEUTIC MEDICINE 21: 19, 2021 Performance evaluation of two fundus oculi angiographic imaging system: Optos 200Tx and Heidelberg Spectralis SHUANG LI, JING‑JING WANG, HONG‑YANG LI, WEI WANG, MENG TIAN, XU‑QIANG LANG and KANG WANG Department of Ophthalmology, Beijing Friendship Hospital, Capital Medical University, Beijing 100050, P.R. China Received December 15, 2018; Accepted October 29, 2019 DOI: 10.3892/etm.2020.9451 Abstract. The present study aimed to compare the imaging Introduction performance of two ultra‑wide‑field fluorescein angiog‑ raphy imaging systems, namely the OptosOptomap 200Tx Ultra‑wide‑field fluorescein angiography (UWFA) is a novel (Optos 200Tx) and the Heidelberg Spectralis (Spectralis). A total technology that has developed rapidly in recent years (1,2). of 18 patients (36 eyes) underwent angiography using the two As numerous pathological changes of fundus diseases occur systems at the Department of Ophthalmology, Beijing Friendship at the edge of the retina, the limitation of imaging leads to Hospital (Beijing, China) between January and June 2017. The insufficient diagnosis or underestimation of the severity of the images were obtained as a single shot centered on the macula. disease (3,4). Therefore, clear imaging of the edge of the retina The total area and area within each of four visualized quadrants is important for the diagnosis, monitoring and prognostication were calculated and compared. The averages of the total and of patients with ocular fundus diseases. The traditional fundus individual quadrant area captured by the Optos 200Tx were fluorescein angiography system may only provide a vision field all larger than those obtained with the Spectralis (P<0.05). -
Vela Proximal Endograft System Phoenix Atherectomy System
A PREVIEW OF today’s NEW PRODUCTS ONS I Vela Proximal Endograft System Endologix (Irvine, CA) has Endologix announced the United States (949) 595-7200 launch of the FDA-approved INNOVAT www.endologix.com/Vela Vela proximal endograft sys- KEY FEATURES tem, which is designed for • Circumferential graft line marker the treatment of proximal for enhanced visibility aortic neck anatomies during • New delivery system endovascular aneurysm repair. • ActiveSeal technology The Vela system, which was developed with feedback from leading physicians, features a new delivery system and a circumferen- tial graft line marker for enhanced visibility during the implantation procedure. One of the first Vela procedures in the United States was performed by Julio Rodriguez, MD, FACS, a vascular surgeon at the Arizona Heart Institute in Phoenix, Arizona. In the company’s press release, Dr. Rodriguez commented, “The Vela delivery system is very intuitive, and the endograft has excellent visibility.” Phoenix Atherectomy System AtheroMed, Inc. (Menlo Park, CA) AtheroMed, Inc. has received CE Mark approval and FDA (650) 473-6846 510(k) clearance to market the Phoenix www.atheromedinc.com Atherectomy System, a pushable, over-the- KEY FEATURES wire system that uses a rotating, front-cut- • Cut, capture, and clear mechanism ting element located at the distal tip of the of action catheter to shave diseased material directly • Able to treat soft plaque or calcium • Profile down to 5 F into the catheter. The debulked material is • No capital equipment required then continuously captured and removed • Front-cutting, single insertion by an internal Archimedes screw that runs the length of the catheter. -

Inpatient Coronary Angiography and Angioplasty (PCI)
If English is not your first language and you need help, please contact the Interpretation and Translation Service Jeśli angielski nie jest twoim pierwszym językiem i potrzebujesz pomocy, skontaktuj się z działem tłumaczeń ustnych i pisemnych ا رﮔ ا یزﯾرﮕﻧ پآ ﯽﮐ ﮩﭘ ﯽﻠ ﺑز نﺎ ںﯾﮩﻧ ﮯﮨ روا پآ وﮐ ددﻣ ﯽﮐ ترورﺿ ﮯﮨ وﺗ ، هارﺑ مرﮐ ﯽﻧﺎﻣﺟرﺗ روا ہﻣﺟرﺗ تﻣدﺧ تﻣدﺧ ہﻣﺟرﺗ روا ﯽﻧﺎﻣﺟرﺗ مرﮐ هارﺑ ، وﺗ ﮯﮨ ترورﺿ ﯽﮐ ددﻣ وﮐ پآ روا ﮯﮨ ںﯾﮩﻧ ﮯﺳ ر ا ﺑ ط ہ ﮐ ر ﯾ ںﯾرﮐ ﮯ Dacă engleza nu este prima ta limbă și ai nevoie de ajutor, te rugăm să contactezi Serviciul de interpretare și traducere Inpatient Coronary ইংরাজী যিদ আপনার .থম ভাষা না হয় এবং আপনার সাহােয9র .েয়াজন হয় তেব অনু=হ কের ?দাভাষী এবং অনুবাদ পিরেষবা@েত ?যাগােযাগ কBন Angiography and (Angioplasty (PCI إ ذ ا مﻟ نﻛﺗ ﻠﺟﻧﻹا ﺔﯾزﯾ ﻲھ كﺗﻐﻟ ﻰﻟوﻷا ﺗﺣﺗو جﺎ إ ﻰﻟ ةدﻋﺎﺳﻣ ، ﻰﺟرﯾﻓ لﺎﺻﺗﻻا ﺔﻣدﺧﺑ ا ﻟ ﺔﻣﺟرﺗ ا ﺔﯾوﻔﺷﻟ او ﻟ ﺔﯾرﯾرﺣﺗ وﺔوﺷ ﻣر ﻣﺧ ﺎﺗاﻰرﻓ،ةﻋﺳ ﻟإج ﺣوﻰواكﻐ ھﺔز ﺟﻹ ﻛ ﻟ : 0161 627 8770 An information guide : [email protected] To improve our care environment for Patients, Visitors and Staff, Northern Care Alliance NHS Group is Smoke Free including buildings, grounds & car parks. For advice on stopping smoking contact the Specialist Stop Smoking Service on 01706 517 522 For general enquiries please contact the Patient Advice and Liaison Service (PALS) on 0161 604 5897 For enquiries regarding clinic appointments, clinical care and treatment please contact 0161 624 0420 and the Switchboard Operator will put you through to the correct department / service The Northern Care Alliance NHS Group (NCA) is one of the largest NHS organisations The Northern Care Alliance NHS Group (NCA) is one of the largest NHS organisationsin the country, employingin the country 17,000 bringing staff and together providing two a NHS range Trusts, of hospital Salford and Royalcommunity NHS Foundationhealthcare services Trust and to around The Pennine 1 million Acute people Hospitals across Salford, NHS Trust. -

Preparing for Your Peripheral Artery Angioplasty and Stenting
Preparing for your Peripheral Artery Angioplasty and Stenting Michigan Medicine Frankel Cardiovascular Center Michigan Medicine Phone Numbers Billing ………………………………………………………………………… 855-855-0863 734-615-0863 Call Center ……………………………………………………………………888-287-1082 Vascular Surgery (use Call Center) ………………………………………888-287-1082 Cardiovascular Operating Room Desk …………………………………734-232-4553 Office of Clinical Safety (comments) ……………………………………877-285-7788 Emergency Department ……………………………………………………734-936-6666 Guest Assistance Program (GAP) (accommodations) …………………800-888-9825 Hospital Operator ……………………………………………………………734-936-4000 Lost & Found …………………………………………………………………734-936-7890 Mardigian Wellness Resource Center ……………………………………734-232-4120 Parking & Transportation …………………………………………………734-764-7474 Registration & Insurance4 Verification …………………………………866-452-9896 Med-Inn (hotel) ……………………………………………………………800-544-8684 734-936-0100 Tobacco Consultation Services ……………………………………………734-938-6222 Units (Patient Care): CVC-4 ICU ……………………………………………………………734-936-6514 CVC-5 Cardiac Surgery ……………………………………………734-232-4772 CVC-2A Cardiac Procedure Unit………………………………… 734-232-4200 Other: Michigan Quit Line (Smoking) ……………………………………………800-784-8669 Address (mail): Frankel CVC (room number/unit if known) or UH (room number/unit if known) Person’s Name University of Michigan Health System 1500 E. Medical Center Drive Ann Arbor, MI 48109 Building Location (visiting): Samuel and Jean Frankel Cardiovascular Center East Ann Street & Observatory Street Ann Arbor, MI 481 Table of Contents: -

Diagnosing and Treating Vascular Disease
THE CENTER FOR VASCULAR CARE AT WASHINGTON HOSPITAL CENTER Diagnosing and Treating Vascular Disease If you have symptoms of vascular disease or Peripheral Artery Disease (PAD), the best thing to do is see your physician for examination and possible testing. And, if you have the following risk factors, see your doctor to determine if you should be tested. The Center for Vascular Care at Washington Hospital Center can provide painless, risk free tests and the most complete array of treatment options for vascular disease in the region. RISK FACTORS TESTING FOR VASCULAR DISEASE FOR VASCULAR DISEASE Ankle-brachial Index: Patients with leg I Cigarette smoking artery blockage are at increased risk of I Older than age 50* heart attack and stroke. This test (ABI) is I Obesity a simple, safe, painless test for blockages. A blood pressure cuff is placed above I Diabetes the ankles and pressures are measured I Heart disease compared to arm pressures to determine I High Cholesterol the risk of cardiovascular events. It takes I High-stress lifestyle 5–10 minutes. I High blood pressure Carotid Duplex Scan: Blockage in a major I Family history of aneurysms artery increases the likelihood of a stroke. *Over age 65 if no other risk factors exist Thickening of the walls of the carotid arteries can lead to heart attack. An arterial SYMPTOMS OF VASCULAR DISEASE duplex scan is a safe, painless, highly I Leg pain that goes away with rest accu rate method of determining blockage. A sound wave device, placed lightly on the I Numbness of the legs or feet at rest skin, can tell if there is a problem.