Coders' Desk Reference for ICD-10-PCS Procedures
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

(FNE) and Nasal Endoscopy in Ireland During COVID-19 Pandemic Rev 1
Royal College of Surgeons in Ireland Coláiste Ríoga na Máinleá in Éirinn Interim Clinical Guidance on Flexible Nasendoscopy (FNE) and Nasal Endoscopy in Ireland during COVID-19 pandemic Rev 1 INTERIM CLINICAL GUIDANCE ON FLEXIBLE NASENDOSCOPY (FNE) AND NASAL ENDOSCOPY IN IRELAND DURING COVID-19 PANDEMIC Rev 1 INTERIM CLINICAL GUIDANCE ON FLEXIBLE NASENDOSCOPY (FNE) AND NASAL ENDOSCOPY IN IRELAND DURING COVID-19 PANDEMIC Table of Contents 1. Overview ............................................................................................................................................................................. 2 2. Purpose ............................................................................................................................................................................... 2 3. Authorship ......................................................................................................................................................................... 2 4. Target Audience .............................................................................................................................................................. 2 5. Introduction ....................................................................................................................................................................... 2 6. Risk of infection associated with FNE .................................................................................................................. 2 7. Aerosol Generating Procedures -

Surgical Treatment of Snoring and Obstructive Sleep Apnea Syndrome
Medical Policy Surgical Treatment of Snoring and Obstructive Sleep Apnea Syndrome Table of Contents Policy: Commercial Coding Information Information Pertaining to All Policies Policy: Medicare Description References Authorization Information Policy History Policy Number: 130 BCBSA Reference Number: 7.01.101 Related Policies None Policy Commercial Members: Managed Care (HMO and POS), PPO, and Indemnity Medicare HMO BlueSM and Medicare PPO BlueSM Members Uvulopalatopharyngoplasty (UPPP) may be MEDICALLY NECESSARY for the treatment of clinically significant obstructive sleep apnea syndrome (OSAS) in appropriately selected adult patients who have failed an adequate trial of continuous positive airway pressure (CPAP) or failed an adequate trial of an oral appliance (OA). Clinically significant OSA is defined as those patients who have: Apnea/hypopnea Index (AHI) or Respiratory Disturbance Index (RDI) 15 or more events per hour, or AHI or RDI 5 or more events and 14 or less events per hour with documented symptoms of excessive daytime sleepiness, impaired cognition, mood disorders or insomnia, or documented hypertension, ischemic heart disease, or history of stroke. Hyoid suspension, surgical modification of the tongue, and/or maxillofacial surgery, including mandibular- maxillary advancement (MMA), may be MEDICALLY NECESSARY in appropriately selected adult patients with clinically significant OSA and objective documentation of hypopharyngeal obstruction who have failed an adequate trial of continuous positive airway pressure (CPAP) or failed an adequate trial of an oral appliance (OA). Clinically significant OSA is defined as those patients who have: AHI or RDI 15 or more events per hour, or AHI or RDI 5 or more events and 14 or less events per hour with documented symptoms of excessive daytime sleepiness, impaired cognition, mood disorders or insomnia, or documented hypertension, ischemic heart disease, or history of stroke. -

Management of Afferent Loop Obstruction: Reoperation Or Endoscopic and Percutaneous Interventions
See discussions, stats, and author profiles for this publication at: https://www.researchgate.net/publication/282163026 Management of afferent loop obstruction: Reoperation or endoscopic and percutaneous interventions Article in World Journal of Gastrointestinal Surgery · September 2015 DOI: 10.4240/wjgs.v7.i9.190 CITATIONS READS 32 427 2 authors, including: Konstantinos Tsalis Aristotle University of Thessaloniki 115 PUBLICATIONS 976 CITATIONS SEE PROFILE Some of the authors of this publication are also working on these related projects: Laparoscopic liver resection using ICG green visualization of hepatic structures View project Laparoscopic liver resection using ICG green visualization of hepatic structures View project All content following this page was uploaded by Konstantinos Tsalis on 26 May 2017. The user has requested enhancement of the downloaded file. Submit a Manuscript: http://www.wjgnet.com/esps/ World J Gastrointest Surg 2015 September 27; 7(9): 190-195 Help Desk: http://www.wjgnet.com/esps/helpdesk.aspx ISSN 1948-9366 (online) DOI: 10.4240/wjgs.v7.i9.190 © 2015 Baishideng Publishing Group Inc. All rights reserved. MINIREVIEWS Management of afferent loop obstruction: Reoperation or endoscopic and percutaneous interventions? Konstantinos Blouhos, Konstantinos Andreas Boulas, Konstantinos Tsalis, Anestis Hatzigeorgiadis Konstantinos Blouhos, Konstantinos Andreas Boulas, Anestis Abstract Hatzigeorgiadis, Department of General Surgery, General Hospital of Drama, 66100 Drama, Greece Afferent loop obstruction is a purely mechanical comp- lication that infrequently occurs following construction Konstantinos Tsalis, D’ Surgical Department, “G. Papanikolaou” of a gastrojejunostomy. The operations most commonly Hospital, Medical School, Aristotle University of Thessaloniki, associated with this complication are gastrectomy 54645 Thessaloniki, Greece with Billroth Ⅱ or Roux-en-Y reconstruction, and pancreaticoduodenectomy with conventional loop or Author contributions: Blouhos K designed the research; Boulas Roux-en-Y reconstruction. -

Program PDF Saturday, March 28, 2020 Updated: 02-14-20
Program PDF Saturday, March 28, 2020 Updated: 02-14-20 Special ‐ Events and Meetings Congenital Heart Disease ‐ Scientific Session #5002 Session #602 Fellowship Administrators in Cardiovascular Education and ACHD Cases That Stumped Me Training Meeting, Day 2 Saturday, March 28, 2020, 8:00 a.m. ‐ 9:30 a.m. Saturday, March 28, 2020, 7:30 a.m. ‐ 5:30 p.m. Room S105b Marriott Marquis Chicago, Great Lakes Ballroom A CME Hours: 1.5 / CNE Hours: CME Hours: / CNE Hours: Co‐Chair: C. Huie Lin 7:30 a.m. Co‐Chair: Karen K. Stout Fellowship Administrators in Cardiovascular Education and Training Meeting, Day 2 8:00 a.m. LTGA, Severe AV Valve Regurgitation, Moderately Reduced EF, And Atrial Acute and Stable Ischemic Heart Disease ‐ Scientific Arrhythmia Session #601 Elizabeth Grier Treating Patients With STEMI: What They Didn't Teach You in Dallas, TX Fellowship! Saturday, March 28, 2020, 8:00 a.m. ‐ 9:30 a.m. 8:05 a.m. Room S505a ARS Questions (Pre‐Panel Discussion) CME Hours: 1.5 / CNE Hours: Elizabeth Grier Dallas, TX Co‐Chair: Frederick G. Kushner Co‐Chair: Alexandra J. Lansky 8:07 a.m. Panelist: Alvaro Avezum Panel Discussion: LTGA With AVVR And Reduced EF Panelist: William W. O'Neill Panelist: Jennifer Tremmel Panelist: Jonathan Nathan Menachem Panelist: Joseph A. Dearani 8:00 a.m. Panelist: Michelle Gurvitz Case of a Young Women With STEMI Panelist: David Bradley Jasjit Bhinder Valhalla, NY 8:27 a.m. ARS Questions (Post‐Panel Discussion) 8:05 a.m. Elizabeth Grier Young Women With STEMI: Something Doesn't Make Sense... -

Deep Venous Thrombosis with Suspected Pulmonary Embolism
Thoracic Imaging Peter A. Loud, MD Deep Venous Thrombosis Douglas S. Katz, MD Dennis A. Bruce, MD with Suspected Pulmonary Donald L. Klippenstein, MD Zachary D. Grossman, MD Embolism: Detection with Combined CT Venography Index terms: Computed tomography (CT), 1 angiography, 9*.129142, and Pulmonary Angiography 9*.12915, 9*.12916 Embolism, pulmonary, 60.72 Pulmonary angiography, 944.12914, 944.12915, 944.12916 PURPOSE: To determine the frequency and location of deep venous thrombosis at Veins, thrombosis, 9*.751, 9*.12914 computed tomographic (CT) venography after CT pulmonary angiography in a large series of patients clinically suspected of having pulmonary embolism and to Radiology 2001; 219:498–502 compare the accuracy of CT venography with lower-extremity venous sonography. Abbreviation: MATERIALS AND METHODS: Venous phase images were acquired from the DVT ϭ deep venous thrombosis diaphragm to the upper calves after completion of CT pulmonary angiography in 650 patients (373 women, 277 men; age range, 18–99 years; mean age, 63 years) 1 From the Department of Radiology, to determine the presence and location of deep venous thrombosis. Results of CT Roswell Park Cancer Institute, Elm and Carlton Sts, Buffalo, NY 14263 (P.A.L., venography were compared with those of bilateral lower-extremity venous sonog- D.L.K., Z.D.G.), and the Department raphy in 308 patients. of Radiology, Winthrop University Hospital, Mineola, NY (D.S.K., D.A.B.). RESULTS: A total of 116 patients had pulmonary embolism and/or deep venous From the 1999 RSNA scientific assem- thrombosis, including 27 patients with pulmonary embolism alone, 31 patients with bly. -

Home Care After Sleep Surgery-Uvulopalatopharyngoplasty (UP3) And/Or Tonsillectomy
Home Care after Sleep Surgery-Uvulopalatopharyngoplasty (UP3) and/or Tonsillectomy The above surgeries are all performed on patients to help relieve or lessen the symptoms of sleep apnea. All address the palate, or the upper part of your throat. General Information You may lack energy for several days, and may also be restless at night. This will improve over the next 10 to 14 days. It is quite common to feel progressively worse during the first five to six days after surgery. You may also become constipated during this time for three reasons: you will not be eating a regular diet, you will be taking pain medications, and you may be less active. Wound Care All of the above surgeries are performed within the mouth on the upper throat. No external incisions are made, all are internal. Depending on the surgery, you may feel and/or see some suture on your palate (upper throat). This is normal and will dissolve over the next two weeks. No specific wound care is necessary for these procedures. Diet It is important for you to drink plenty of fluids after surgery. Drink every hour while awake. A soft diet is recommended for the first 14 days (anything that you may eat without teeth constitutes as a soft diet). Avoid hot liquids/solids. It is alright if you don’t feel like eating much, as long as you drink lots of fluids. Signs that you need to drink more are when the urine is darker in color (urine should be pale yellow). A high fever that persists may also be a sign that you are not taking in enough fluids. -

Urology Services in the ASC
Urology Services in the ASC Brad D. Lerner, MD, FACS, CASC Medical Director Summit ASC President of Chesapeake Urology Associates Chief of Urology Union Memorial Hospital Urologic Consultant NFL Baltimore Ravens Learning Objectives: Describe the numerous basic and advanced urology cases/lines of service that can be provided in an ASC setting Discuss various opportunities regarding clinical, operational and financial aspects of urology lines of service in an ASC setting Why Offer Urology Services in Your ASC? Majority of urologic surgical services are already outpatient Many urologic procedures are high volume, short duration and low cost Increasing emphasis on movement of site of service for surgical cases from hospitals and insurance carriers to ASCs There are still some case types where patients are traditionally admitted or placed in extended recovery status that can be converted to strictly outpatient status and would be suitable for an ASC Potential core of fee-for-service case types (microsurgery, aesthetics, prosthetics, etc.) Increasing Population of Those Aged 65 and Over As of 2018, it was estimated that there were 51 million persons aged 65 and over (15.63% of total population) By 2030, it is expected that there will be 72.1 million persons aged 65 and over National ASC Statistics - 2017 Urology cases represented 6% of total case mix for ASCs Urology cases were 4th in median net revenue per case (approximately $2,400) – behind Orthopedics, ENT and Podiatry Urology comprised 3% of single specialty ASCs (5th behind -

Congenital Heart Disease
GUEST EDITORIAL Congenital heart disease Pediatric Anesthesia is the only anesthesia journal ded- who developed hypoglycemia were infants. (9). Steven icated exclusively to perioperative issues in children and Nicolson take the opposite approach of ‘first do undergoing procedures under anesthesia and sedation. no harm’ (10). If we do not want ‘tight glycemic con- It is a privilege to be the guest editor of this special trol’ because of concern about hypoglycemic brain issue dedicated to the care of children with heart dis- injury, when should we start treating blood sugars? ease. The target audience is anesthetists who care for There are no clear answers based on neurological out- children with heart disease both during cardiac and comes in children. non-cardiac procedures. The latter takes on increasing Williams and Cohen (11) discuss the care of low importance as children with heart disease undergoing birth weight (LBW) infants and their outcomes. Pre- non-cardiac procedures appear to be at a higher risk maturity and LBW are independent risk factors for for cardiac arrest under anesthesia than those without adverse outcomes after cardiac surgery. Do the anes- heart disease (1). We hope the articles in this special thetics we use add to this insult? If prolonged exposure issue will provide guidelines for management and to volatile anesthetics is bad for the developing neona- spark discussions leading to the production of new tal brain, would avoiding them make for improved guidelines. outcomes? Wise-Faberowski and Loepke (12) review Over a decade ago Austin et al. (2) demonstrated the current research in search of a clear answer and the benefits of neurological monitoring during heart conclude that there isn’t one. -

Surgeries by STAT Category
STAT SURGICAL PROCEDURE CATEGORY ASD repair, Patch 1 AVC (AVSD) repair, Partial (Incomplete) (PAVSD) 1 PFO, Primary closure 1 ASD repair, Primary closure 1 VSD repair, Patch 1 DCRV repair 1 Aortic stenosis, Subvalvar, Repair 1 Coarctation repair, End to end 1 Vascular ring repair 1 ICD (AICD) implantation 1 ICD (AICD) ([automatic] implantable cardioverter deFibrillator) procedure 1 ASD Repair, Patch + PAPCV Repair 1 VSD repair, Primary closure 1 AVC (AVSD) repair, Intermediate (Transitional) 1 PAPVC repair 1 TOF repair, No ventriculotomy 1 TOF repair, Ventriculotomy, Nontransanular patch 1 Conduit reoperation 1 Valve replacement, Pulmonic (PVR) 1 Valve replacement, Aortic (AVR), Mechanical 1 Valve replacement, Aortic (AVR), Bioprosthetic 1 Sinus oF Valsalva, Aneurysm repair 1 Fontan, TCPC, Lateral tunnel, Fenestrated 1 Coarctation repair, Interposition graFt 1 Pacemaker procedure 1 Glenn (Unidirectional cavopulmonary anastomosis) (Unidirectional Glenn) 1 PAPVC Repair, BaFFle redirection to leFt atrium with systemic vein translocation (Warden) (SVC 1 sewn to right atrial appendage) 1 1/2 ventricular repair 2 PA, Reconstruction (Plasty), Main (Trunk) 2 Valvuloplasty, Aortic 2 Ross procedure 2 LV to aorta tunnel repair 2 Valvuloplasty, Mitral 2 Fontan, Atrio-pulmonary connection 2 PDA closure, Surgical 2 Aortopexy 2 Pacemaker implantation, Permanent 2 Arrhythmia surgery - ventricular, Surgical Ablation 2 Bilateral bidirectional cavopulmonary anastomosis (BBDCPA) (Bilateral bidirectional Glenn) 2 Superior Cavopulmonary anastomosis(es) + PA -

Pediatric Radiology
2013 RSNA (Filtered Schedule) Sunday, December 01, 2013 10:30-12:00 PM • VSPD11 • Room: S100AB • Pediatric Radiology Series: Pediatric Neuroimaging I 10:45-12:15 PM • SPOI11 • Room: E353C • Oncodiagnosis Panel: Pediatric Sarcoma (An Interactive Session) 12:30-01:00 PM • CL-PDS-SUA • Room: S101AB • Pediatric Radiology - Sunday Posters and Exhibits (12:30pm - 1:00pm) 01:00-01:30 PM • CL-PDS-SUB • Room: S101AB • Pediatric Radiology - Sunday Posters and Exhibits (1:00pm - 1:30pm) 02:00-03:30 PM • VSPD12 • Room: S102AB • Pediatric Radiology Series: Pediatric Musculoskeletal Monday, December 02, 2013 08:30-10:00 AM • RC224 • Room: E353B • Mentored Case Approach to Pediatric Cardiovascular Disease 1: Vascular Disease (An Interactive Session) 08:30-12:00 PM • VSPD21 • Room: S102AB • Pediatric Radiology Series: Fetal - Neonatal Imaging 12:15-12:45 PM • CL-PDS-MOA • Room: S101AB • Pediatric Radiology - Monday Posters and Exhibits (12:15pm - 12:45pm) 12:45-01:15 PM • CL-PDS-MOB • Room: S101AB • Pediatric Radiology - Monday Posters and Exhibits (12:45pm - 1:15pm) 03:00-04:00 PM • SSE21 • Room: S102AB • Pediatric (Neuroimaging) Tuesday, December 03, 2013 08:30-10:00 AM • RC324 • Room: S402AB • Mentored Case Approach to Pediatric Cardiovascular Disease 2: Cardiac Disease (An Interactive Session) 08:30-12:00 PM • VSPD31 • Room: S102AB • Pediatric Radiology Series: Chest/Cardiovascular Imaging I 12:15-12:45 PM • CL-PDS-TUA • Room: S101AB • Pediatric Radiology - Tuesday Scientific Posters and Exhibits (12:15pm - 12:45pm) 12:45-01:15 PM • CL-PDS-TUB • -
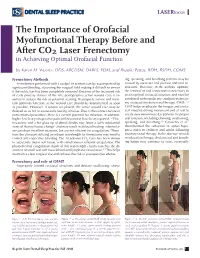
The Importance of Orofacial Myofunctional Therapy Before and After CO2 Laser Frenectomy in Achieving Optimal Orofacial Function
LASERfocus The Importance of Orofacial Myofunctional Therapy Before and After CO2 Laser Frenectomy in Achieving Optimal Orofacial Function by Karen M. Wuertz, DDS, ABCDSM, DABLS, FOM, and Brooke Pettus, RDH, BSDH, COMS Frenectomy Methods ing, speaking, and breathing patterns may be Frenotomies performed with a scalpel or scissors can be accompanied by caused by incorrect oral posture and oral re- significant bleeding, obscuring the surgical field making it difficult to ensure strictions. Therefore, in the authors’ opinion, if the restriction has been completely removed. Because of the increased risk the removal of oral restrictions is necessary to of early primary closure of the site, postoperative active wound care is es- attain optimal orofacial function, and must be sential to reduce the risk of potential scarring. To properly restore and main- combined with regular pre- and post-frenecto- tain optimum function, active wound care should be implemented as soon my orofacial myofunctional therapy (OMT).1,4 as possible. However, if sutures are placed, the active wound care may be OMT helps re-educate the tongue and orofa- delayed so as not to cause early tearing of tissue. Due to the contact nature of cial muscles during movement and at rest to conventional procedure, there is a certain potential for infection; in addition, create new neuromuscular patterns for proper higher levels of postoperative pain and discomfort have been reported.1,2 Elec- oral function, including chewing, swallowing, trocautery and a hot glass tip of dental diodes may leave a fairly substantial speaking, and breathing.5,6 Camacho et al.7 zone of thermal tissue change3 and may result in delayed healing. -
Spring Programme 2011
Faculty of Radiologists Royal College of Surgeons in Ireland Combined Spring Meeting 8th & 9 th April 2011 Venue: Castlemartyr Hotel, Co. Cork. Programme Faculty of Radiologists, Royal College of Surgeons in Ireland CPD Credits Awarded: 5 Royal College of Radiologists credits are applied for. Friday 8 th April 2011 3.30-4.30pm Registration 4.30-5.30pm Stroke in 2011, Moderator: Dr. Ian Kelly, Waterford Regional Hospital 4.30-5.00pm Acute Stoke Imaging. Dr Noel Fanning, Cork University Hospital, Cork 5.00-5.30pm Stroke: A clinical perspective. Dr. George Pope, John Radcliffe Hospitals, Oxford 5.30-6.30pm Moderator: Dr. Adrian Brady, Dean, Faculty of Radiologists Belfast to Bosnia and Autopsy to Virtopsy Dr. Jack Crane, State Pathologist, NI 8pm Dinner Saturday 9 th April 2011 8.30-9.00am Registration 9.00-10.00am Liver hour. Moderator: Dr John Feeney, AMNCH, Dublin 9.00-9.30am Liver imaging pre metastatectomy. Dr. Peter MacEneaney, Mercy University Hospital, Cork 9.30-10.00am Parenchymal and focal liver biopsy - when and how. Dr Stephen J Skehan St Vincent's University Hospital, Dublin 10.00-11.00am Paediatric Hour. Moderator: Dr. Stephanie Ryan, The Children’s University Hospital Temple Street, Dublin 10.00-10.30am Paediatric Abdominal Emergencies. Dr Eoghan Laffan, The Children’s, University Hospital Temple Street, Dublin 10.30-11.00am Non Accidental Injury. Dr Conor Bogue, Cork University Hospital, Cork 11.00-11.30am Tea/Coffee Break and Poster Exhibition 11.30-12.30pm MSK Hour. Moderator: Dr Orla Buckley, AMNCH, Dublin 11.30-12.00pm Image guided joint interventions.