Peripheral Nerve Lesions
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Hereditary Hypertrophic Neuropathy Combining Features of Tic Douloureux, Charcot- Marie-Tooth Disease, and Deafness
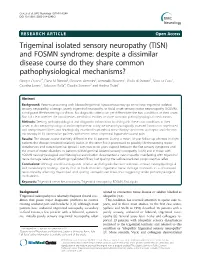
Hereditary hypertrophic neuropathy combining features of tic douloureux, Charcot- Marie-Tooth disease, and deafness Hereditary hypertrophic sensorimotor poly- neuropathy combining the features of Charcot- Marie-Tooth disease, trigeminal neuralgia, and Robert P. Cruse, D.O. deafness occurred through four generations of John P. Conomy, M.D. a family originating in Haywood County, North Asa J. Wilbourn, M.D. Carolina. Fourteen individuals had pes cavus, Maurice R. Hanson, M.D. distal muscle atrophy, depressed or absent mus- cle stretch reflexes, cutaneous sensory deficits, Department of Neurology and defective proprioception. Six family mem- bers had recurrent, lancinating, trigeminal pain, and seven were deaf. The family was brought under scrutiny when the propositus, a 60-year-old woman, was examined for treat- ment of tic douloureux. Neurologic informa- tion was ultimately obtained regarding 52 family members. No history of consanguinity could be ascertained within this kinship. The genealogy of the family we studied is presented in Figure 1. In addition to clinical neurologic examinations, electromyographic and nerve conduction stud- ies were obtained on those individuals indicated in the genealogy diagram. Audiometric studies were obtained when there was clinical indication of defective hearing. Quantitative cutaneous sensory testing was obtained in the propositus. 107 Downloaded from www.ccjm.org on October 1, 2021. For personal use only. All other uses require permission. 108 Cleveland Clinic Quarterly Vol. 44, No. 3 ' • CMT a TIC Deaf CMT He Examined MS f Died O Not Affected 0 D led before age onset (O Multiple normal d1 ond j si be. -1—i Two Marriages —Indicates number of slbs. -

(12) Patent Application Publication (10) Pub. No.: US 2007/0254315 A1 Cox Et Al
US 20070254315A1 (19) United States (12) Patent Application Publication (10) Pub. No.: US 2007/0254315 A1 Cox et al. (43) Pub. Date: Nov. 1, 2007 (54) SCREENING FOR NEUROTOXIC AMINO (60) Provisional application No. 60/494.686, filed on Aug. ACID ASSOCATED WITH NEUROLOGICAL 12, 2003. DSORDERS Publication Classification (75) Inventors: Paul A. Cox, Provo, UT (US); Sandra A. Banack, Fullerton, CA (US); Susan (51) Int. Cl. J. Murch, Cambridge (CA) GOIN 33/566 (2006.01) GOIN 33/567 (2006.01) Correspondence Address: (52) U.S. Cl. ............................................................ 435/721 PILLSBURY WINTHROP SHAW PITTMAN LLP (57) ABSTRACT ATTENTION: DOCKETING DEPARTMENT Methods for screening for neurological disorders are dis P.O BOX 105OO closed. Specifically, methods are disclosed for screening for McLean, VA 22102 (US) neurological disorders in a Subject by analyzing a tissue sample obtained from the subject for the presence of (73) Assignee: THE INSTITUTE FOR ETHNO elevated levels of neurotoxic amino acids or neurotoxic MEDICINE, Provo, UT derivatives thereof associated with neurological disorders. In particular, methods are disclosed for diagnosing a neu (21) Appl. No.: 11/760,668 rological disorder in a subject, or predicting the likelihood of developing a neurological disorder in a Subject, by deter (22) Filed: Jun. 8, 2007 mining the levels of B-N-methylamino-L-alanine (BMAA) Related U.S. Application Data in a tissue sample obtained from the subject. Methods for screening for environmental factors associated with neuro (63) Continuation of application No. 10/731,411, filed on logical disorders are disclosed. Methods for inhibiting, treat Dec. 8, 2003, now Pat. No. 7,256,002. -

Peripheral Neuropathy in Complex Inherited Diseases: an Approach To
PERIPHERAL NEUROPATHY IN COMPLEX INHERITED DISEASES: AN APPROACH TO DIAGNOSIS Rossor AM1*, Carr AS1*, Devine H1, Chandrashekar H2, Pelayo-Negro AL1, Pareyson D3, Shy ME4, Scherer SS5, Reilly MM1. 1. MRC Centre for Neuromuscular Diseases, UCL Institute of Neurology and National Hospital for Neurology and Neurosurgery, London, WC1N 3BG, UK. 2. Lysholm Department of Neuroradiology, National Hospital for Neurology and Neurosurgery, London, WC1N 3BG, UK. 3. Unit of Neurological Rare Diseases of Adulthood, Carlo Besta Neurological Institute IRCCS Foundation, Milan, Italy. 4. Department of Neurology, University of Iowa, 200 Hawkins Drive, Iowa City, IA 52242, USA 5. Department of Neurology, University of Pennsylvania, Philadelphia, PA 19014, USA. * These authors contributed equally to this work Corresponding author: Mary M Reilly Address: MRC Centre for Neuromuscular Diseases, 8-11 Queen Square, London, WC1N 3BG, UK. Email: [email protected] Telephone: 0044 (0) 203 456 7890 Word count: 4825 ABSTRACT Peripheral neuropathy is a common finding in patients with complex inherited neurological diseases and may be subclinical or a major component of the phenotype. This review aims to provide a clinical approach to the diagnosis of this complex group of patients by addressing key questions including the predominant neurological syndrome associated with the neuropathy e.g. spasticity, the type of neuropathy, and the other neurological and non- neurological features of the syndrome. Priority is given to the diagnosis of treatable conditions. Using this approach, we associated neuropathy with one of three major syndromic categories - 1) ataxia, 2) spasticity, and 3) global neurodevelopmental impairment. Syndromes that do not fall easily into one of these three categories can be grouped according to the predominant system involved in addition to the neuropathy e.g. -

Case Vignettes
“Doc, DO I Have Neuropathy?” Case Vignettes Susan, 50 Gwenn, 32 John, 52 Sally, 42 DM – 12 yrs Hypothyroidism No PMH No PMH B/N/T – 2 yrs N/T at night B/N/T – 6 days B/N/T – few months 3 months Stanley Jones P. Iyadurai, MSc, PhD, MD Hands, Hands, Arms Hands, Feet Assistant Professor of Neurology Feet Right hand Feet, Legs Burning Pain Neuromuscular Division, Department of Neurology Arms, Difficulty Pain Pain The Ohio State University Wexner Medical Center Legs Opening jars Breathing Redness Imbalance Normal gait Imbalance Normal Strength “Neuropathy” - Definition Neuropathy - General Theme • Symmetric • “Neuron” and “Pathos” (Greek) • Insidious • More prominent distally and starts in • Disease of the Peripheral Nerve legs • Involves both motor and sensory • Dysfunction of the nerves outside of components the central nervous system • May cause pain • May cause loss of balance • Progressive, but not debilitating 1 Not all that tingles is Classification - Functional neuropathy ‘numbness and tingling’ • Motor – affects the motor nerves Weakness • not all numbness and tingling is • Sensory peripheral nerve ‒ Pain • RLS ‒ Small Fiber ‒ Large Fiber • edema ‒ Large and Small Fiber • deconditioning ‒ Neuronopathy (ganglionopathy) • central nervous system • Autonomic • Sweating Changes, Blood Pressure Changes • nerve root [‘sciatica’] Classification – Time-course Classification – Time-course • Acute Immune-mediated • Congenital/Hereditary • Infantile Weakness • Childhood-onset • Acquired • Relapsing ‒ Reversible? • Hereditary ‒ Demyelinating? -

Ataxia with Loss of Purkinje Cells in a Mouse Model for Refsum Disease
Ataxia with loss of Purkinje cells in a mouse model for Refsum disease Sacha Ferdinandussea,1,2, Anna W. M. Zomerb,1, Jasper C. Komena, Christina E. van den Brinkb, Melissa Thanosa, Frank P. T. Hamersc, Ronald J. A. Wandersa,d, Paul T. van der Saagb, Bwee Tien Poll-Thed, and Pedro Britesa Academic Medical Center, Departments of aClinical Chemistry (Laboratory of Genetic Metabolic Diseases) and dPediatrics, Emma’s Children Hospital, University of Amsterdam, 1105 AZ Amsterdam, The Netherlands; bHubrecht Institute, Royal Netherlands Academy of Arts and Sciences 3584 CT Utrecht, The Netherlands; and cRehabilitation Hospital ‘‘De Hoogstraat’’ Rudolf Magnus Institute of Neuroscience, 3584 CG Utrecht, The Netherlands Edited by P. Borst, The Netherlands Cancer Institute, Amsterdam, The Netherlands, and approved October 3, 2008 (received for review June 23, 2008) Refsum disease is caused by a deficiency of phytanoyl-CoA hy- Clinically, Refsum disease is characterized by cerebellar droxylase (PHYH), the first enzyme of the peroxisomal ␣-oxidation ataxia, polyneuropathy, and progressive retinitis pigmentosa, system, resulting in the accumulation of the branched-chain fatty culminating in blindness, (1, 3). The age of onset of the symptoms acid phytanic acid. The main clinical symptoms are polyneuropathy, can vary from early childhood to the third or fourth decade of cerebellar ataxia, and retinitis pigmentosa. To study the patho- life. No treatment is available for patients with Refsum disease, genesis of Refsum disease, we generated and characterized a Phyh but they benefit from a low phytanic acid diet. Phytanic acid is knockout mouse. We studied the pathological effects of phytanic derived from dietary sources only, specifically from the chloro- acid accumulation in Phyh؊/؊ mice fed a diet supplemented with phyll component phytol. -

Molecular Diagnostics of Charcot-Marie-Tooth Disease and Related Peripheral Neuropathies
17_Lupski 3/30/06 1:47 PM Page 243 NeuroMolecular Medicine Copyright © 2006 Humana Press Inc. All rights of any nature whatsoever reserved. ISSN0895-8696/06/08:243–254/$30.00 doi: 10.1385/NMM:8:1:243 REVIEW ARTICLE Molecular Diagnostics of Charcot-Marie-Tooth Disease and Related Peripheral Neuropathies Kinga Szigeti,1 Eva Nelis,2,3 and James R. Lupski*,1,4 1Departments of Molecular and Human Genetics, Baylor College of Medicine, Houston, TX; 2Molecular Genetics, Flanders Interuniversity Institute for Biotechnology, Institute Born-Bunge, University of Antwerp, Antwerpen, Belgium; 3Laboratory of Neurogenetics, Institute Born-Borge, University of Antwerp, Antwerpen, Belgium; and 4Pediatrics, Baylor College of Medicine, and Texas Children Hospital, Houston, TX 77030 Received January 10, 2006; Revised January 13, 2006; Accepted January 13, 2006 Abstract DNAdiagnostics plays an important role in the characterization and management of patients manifesting inherited peripheral neuropathies. We describe the clinical integration of molecular diagnostics with medical history, physical examination, and electrophysiological studies. Mole- cular testing can help establish a secure diagnosis, enable genetic counseling regarding recurrence risk, potentially provide prognostic information, and in the near future may be important for the choice of therapies. doi: 10.1385/NMM:8:1:243 Index Entries:Molecular diagnostics; Charcot-Marie-Tooth disease; CMT; hereditary neuropathy with liability to pressure palsies; HNPP; Dejerine-Sottas neuropathy; DSN; congenital hypomyelinating neuropathy; CHN; CMT1A duplication; HNPP deletion. Introduction genetic testing, one needs to be familiar with the diagnostic tests available, choose the appropriate Molecular genetic diagnosis has become an inte- patients for testing, and utilize the diagnostic tools gral part of the evaluation of patients with hered- in a logical fashion to optimize the use of resources. -

ICD9 & ICD10 Neuromuscular Codes
ICD-9-CM and ICD-10-CM NEUROMUSCULAR DIAGNOSIS CODES ICD-9-CM ICD-10-CM Focal Neuropathy Mononeuropathy G56.00 Carpal tunnel syndrome, unspecified Carpal tunnel syndrome 354.00 G56.00 upper limb Other lesions of median nerve, Other median nerve lesion 354.10 G56.10 unspecified upper limb Lesion of ulnar nerve, unspecified Lesion of ulnar nerve 354.20 G56.20 upper limb Lesion of radial nerve, unspecified Lesion of radial nerve 354.30 G56.30 upper limb Lesion of sciatic nerve, unspecified Sciatic nerve lesion (Piriformis syndrome) 355.00 G57.00 lower limb Meralgia paresthetica, unspecified Meralgia paresthetica 355.10 G57.10 lower limb Lesion of lateral popiteal nerve, Peroneal nerve (lesion of lateral popiteal nerve) 355.30 G57.30 unspecified lower limb Tarsal tunnel syndrome, unspecified Tarsal tunnel syndrome 355.50 G57.50 lower limb Plexus Brachial plexus lesion 353.00 Brachial plexus disorders G54.0 Brachial neuralgia (or radiculitis NOS) 723.40 Radiculopathy, cervical region M54.12 Radiculopathy, cervicothoracic region M54.13 Thoracic outlet syndrome (Thoracic root Thoracic root disorders, not elsewhere 353.00 G54.3 lesions, not elsewhere classified) classified Lumbosacral plexus lesion 353.10 Lumbosacral plexus disorders G54.1 Neuralgic amyotrophy 353.50 Neuralgic amyotrophy G54.5 Root Cervical radiculopathy (Intervertebral disc Cervical disc disorder with myelopathy, 722.71 M50.00 disorder with myelopathy, cervical region) unspecified cervical region Lumbosacral root lesions (Degeneration of Other intervertebral disc degeneration, -
Trigeminal Isolated Sensory Neuropathy (TISN) and FOSMN
Cruccu et al. BMC Neurology (2014) 14:248 DOI 10.1186/s12883-014-0248-2 RESEARCH ARTICLE Open Access Trigeminal isolated sensory neuropathy (TISN) and FOSMN syndrome: despite a dissimilar disease course do they share common pathophysiological mechanisms? Giorgio Cruccu1*, Elena M Pennisi2, Giovanni Antonini3, Antonella Biasiotta1, Giulia di Stefano1, Silvia La Cesa1, Caterina Leone1, Salvatore Raffa4, Claudia Sommer5 and Andrea Truini1 Abstract Background: Patients presenting with bilateral trigeminal hypoesthesia may go on to have trigeminal isolated sensory neuropathy, a benign, purely trigeminal neuropathy, or facial-onset sensory motor neuronopathy (FOSMN), a malignant life-threatening condition. No diagnostic criteria can yet differentiate the two conditions at their onset. Nor is it clear whether the two diseases are distinct entities or share common pathophysiological mechanisms. Methods: Seeking pathophysiological and diagnostic information to distinguish these two conditions at their onset, in this neurophysiological and morphometric study we neurophysiologically assessed function in myelinated and unmyelinated fibres and histologically examined supraorbital nerve biopsy specimens with optic and electron microscopy in 13 consecutive patients with recent onset trigeminal hypoesthesia and pain. Results: The disease course distinctly differed in the 13 patients. During a mean 10 year follow-up whereas in eight patients the disease remained relatively stable, in the other five it progressed to possibly life-threatening motor disturbances and extra-trigeminal spread. From two to six years elapsed between the first sensory symptoms and the onset of motor disorders. In patients with trigeminal isolated sensory neuropathy (TISN) and in those with FOSMN neurophysiological and histological examination documented a neuronopathy manifesting with trigeminal nerve damage selectively affecting myelinated fibres, but sparing the Ia-fibre-mediated proprioceptive reflex. -

Come to Your Senses: Atypical Polyneuropathy
Come To Your Senses: Atypical Polyneuropathy Damian Campbell, DO; Joshua Lovell, DO; Krishna Pokala, MD; Yessar Hussain, MD The University of Texas at Austin, Department of Neurology, Dell Medical School Clinical History Workup Diagnosis and Discussion Pathophysiology 35 year old female was referred to the neurology clinic for evaluation of an Electrodiagnostics Our patients clinical history and genetic testing results were consistent and There is a great deal of variability in the presentation of symptoms; as there is abnormal gait. She reported slow but progressive changes in her gait over the she was diagnosed with PHARC: Polyneuropathy, Hearing Loss, Ataxia, variability amongst the gene mutations leading to inactive ABHD12. Despite the course of the last ten years. Her changes ranged from a sense of feeling off- Nerve Conductions Retinitis Pigmentosa, Cataracts. variability that exists within gene mutations, it is posited that all of the balanced to shooting pain down each leg She felt that her pain originated in her Distal Latency Peak Amplitude Conduction Velocity homozygous mutations result in complete loss-of-function of the ABHD12 low back and radiated posteriorly down each leg without any accompanying Latency (m/sec) PHARC was first described by Fiskerstrand et al in 2008.(1) At that time they enzyme. Reduction in ABHD12 results in increased levels of endocannabinoid Right Median CMAP 4.3 7.8 numbness, weakness, or bowel and bladder involvement. Of significance is her were attempting to genetically characterize a neurological disorder that arachidonoyl glycerol 2-AG, which has important functions in synaptic plasticity 11.6 5.8 26 resembled Refsum disease in a Norwegian family. -

Retinitis Pigmentosa, Ataxia, and Peripheral Neuropathy
J Neurol Neurosurg Psychiatry: first published as 10.1136/jnnp.46.3.206 on 1 March 1983. Downloaded from Journal of Neurology, Neurosurgery, and Psychiatry 1983;46:206-213 Retinitis pigmentosa, ataxia, and peripheral neuropathy RR TUCK, JG McLEOD From the Department ofMedicine, University ofSydney, Australia SUMMARY The clinical features of four patients with retinitis pigmentosa, ataxia and peripheral neuropathy but with no increase in serum phytanic acid are reported. Three patients also had sensorineural deafness and radiological evidence of cerebellar atrophy. Nerve conduction studies revealed abnormalities of sensory conduction and normal or only mild slowing of motor conduc- tion velocity. Sural nerve biopsy demonstrated a reduction in the density of myelinated fibres. There were no onion bulb formations. These cases clinically resemble Refsum's disease, but differ in having no detectable biochemical abnormality, and a peripheral neuropathy which is not hypertrophic in type. They may represent unusual cases of spinocerebellar degeneration. Retinitis pigmentosa occurs infrequently as an iso- (WAIS). He had a speech impediment but was not dysar- Protected by copyright. lated finding in otherwise healthy individuals and thric. He was of short stature, had a small head and pes families. Its association with deafness, with or with- cavus but no kyphoscoliosis. His visual acuity in the right eye was 6/60 while in the left he could count fingers only. out other neurological abnormalities is much less The right visual field was constricted but the left could not common but nevertheless well recognised.1 In be tested. The optic discs were pale, the retinal vessels heredopathia atactica polyneuritiformis (Refsum's small in diameter and throughout the retinae there was disease), abetalipoproteinaemia, and the Keams- scattered "bone corpuscle" pigmentation. -

Neuropathic Orofacial Pain the Brochure Is Provided Compliments Of
Neuropathic_Pain_Brochure_Neuropathic_Pain_Brochure 6/9/2010 11:41 AM Page 1 Neuropathic orofacial paiN The brochure is provided compliments of This brochure in intended for informational purposes only and should be considered a replacement for a professional treatment for a health care professional. To locate knowledgeable and experienced expert in orofacial pain, contact: The American Academy of Orofacial Pain 174 S. New York Ave. POB 478 Oceanville, NJ 08231 P: 609-504-1311 E: [email protected] W: www.aaop.org To locate knowledgeable and experienced expert in Trigeminal Neuralgia, contact: Trigeminal Neuralgia Association 2801 SW Archer Road Gainesville, FL 32608 P: 352-376-9955 E: [email protected] W: www.tna-support.org Neuropathic_Pain_Brochure_Neuropathic_Pain_Brochure 6/9/2010 11:41 AM Page 3 coNteNts 1-Neuropathic orofacial paiN 4-GettiNG help/What to expect 6-commoN Neuropathic orofacial paiN DisorDers aND their treatmeNt 6 - triGem iNal NeuralGia 8 - pre-triGem iNal NeuralGia 9 - atypical oDoNtalGia (phaNtom tooth paiN) 10 - chroNic reGioNal paiN syNDrome 12 - iN coNclusioN Neuropathic_Pain_Brochure_Neuropathic_Pain_Brochure 6/9/2010 11:41 AM Page 4 Neuropathic orofacial paiN Of the many pains that can effect the head and neck, perhaps the most confusing and difficult to diagnose are a group of maladies called Neuropathic Orofacial Pain Disorders. These neuropathic pain disorders are often chronic and arise from the brain and nerves of the head, face and neck. If you have experienced the frustration of having a toothache or face pain and, after seeing many doctors, still don't know where the pain is coming from, Brain you may be suffering from a neuropathic pain Spinal Cord disorder. -

Trigeminal Neuralgia – Diagnosis and Treatment
View metadata, citation and similar papers at core.ac.uk brought to you by CORE provided by Archivio della ricerca- Università di Roma La Sapienza Review Cephalalgia 2017, Vol. 37(7) 648–657 ! International Headache Society 2017 Trigeminal neuralgia – Reprints and permissions: sagepub.co.uk/journalsPermissions.nav diagnosis and treatment DOI: 10.1177/0333102416687280 journals.sagepub.com/home/cep Stine Maarbjerg1, Giulia Di Stefano2, Lars Bendtsen1 and Giorgio Cruccu2 Abstract Introduction: Trigeminal neuralgia (TN) is characterized by touch-evoked unilateral brief shock-like paroxysmal pain in one or more divisions of the trigeminal nerve. In addition to the paroxysmal pain, some patients also have continuous pain. TN is divided into classical TN (CTN) and secondary TN (STN). Etiology and pathophysiology: Demyelination of primary sensory trigeminal afferents in the root entry zone is the predominant pathophysiological mechanism. Most likely, demyelination paves the way for generation of ectopic impulses and ephaptic crosstalk. In a significant proportion of the patients, the demyelination is caused by a neurovascular conflict with morphological changes such as compression of the trigeminal root. However, there are also other unknown etiological factors, as only half of the CTN patients have morphological changes. STN is caused by multiple sclerosis or a space-occupying lesion affecting the trigeminal nerve. Differential diagnosis and treatment: Important differential diagnoses include trigeminal autonomic cephalalgias, posttraumatic or postherpetic pain and other facial pains. First line treatment is prophylactic medication with sodium channel blockers, and second line treatment is neurosurgical intervention. Future perspectives: Future studies should focus on genetics, unexplored etiological factors, sensory function, the neurosurgical outcome and complications, combination and neuromodulation treatment as well as development of new drugs with better tolerability.