Visual Impairment Age-Related Macular
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Screening Guide for Usher Syndrome
Screening Guide for Usher Syndrome Florida Outreach Project for Children and Young Adults Who Are Deaf-Blind Bureau of Exceptional Education and Student Services Florida Department of Education 2012 This publication was produced through the Bureau of Exceptional Education and Student Services (BEESS) Resource and Information Center, Division of Public Schools, Florida Department of Education, and is available online at http://www.fldoe.org/ese/pub-home.asp. For information on available resources, contact the BEESS Resource and Information Center (BRIC). BRIC website: http://www.fldoe.org/ese/clerhome.asp Bureau website: http://fldoe.org/ese/ Email: [email protected] Telephone: (850) 245-0475 Fax: (850) 245-0987 This document was developed by the Florida Instructional Materials Center for the Visually Impaired, Outreach Services for the Blind/Visually Impaired and Deaf/Hard-of-Hearing, and the Resource Materials and Technology Center for the Deaf/Hard-of-Hearing, special projects funded by the Florida Department of Education, Division of Public Schools, BEESS, through federal assistance under the Individuals with Disabilities Education Act (IDEA), Part B, in conjunction with the Florida Outreach Project for Children and Young Adults Who Are Deaf- Blind, H326C990032, which is funded by the Office of Special Education Programs, U.S. Department of Education. Information contained within this publication does not necessarily reflect the views of the U.S. Department of Education. Edited by: Susan Lascek, Helen Keller National Center Emily Taylor-Snell, Florida Project for Children and Young Adults Who Are Deaf-Blind Dawn Saunders, Florida Department of Education Leanne Grillot, Florida Department of Education Adapted with permission from the Nebraska Usher Syndrome Screening Project (2002) Copyright State of Florida Department of State 2012 Authorization for reproduction is hereby granted to the state system of public education consistent with section 1006.03(2), Florida Statutes. -

Blue Cone Monochromacy: Visual Function and Efficacy Outcome Measures for Clinical Trials
RESEARCH ARTICLE Blue Cone Monochromacy: Visual Function and Efficacy Outcome Measures for Clinical Trials Xunda Luo1☯‡, Artur V. Cideciyan1☯‡*, Alessandro Iannaccone2, Alejandro J. Roman1, Lauren C. Ditta2, Barbara J. Jennings2, Svetlana A. Yatsenko3, Rebecca Sheplock1, Alexander Sumaroka1, Malgorzata Swider1, Sharon B. Schwartz1, Bernd Wissinger4, Susanne Kohl4, Samuel G. Jacobson1* 1 Scheie Eye Institute, Department of Ophthalmology, Perelman School of Medicine, University of Pennsylvania, Philadelphia, Pennsylvania, United States of America, 2 Hamilton Eye Institute, Department of Ophthalmology, University of Tennessee Health Science Center, Memphis, Tennessee, United States of America, 3 Pittsburgh Cytogenetics Laboratory, Center for Medical Genetics and Genomics, University of Pittsburgh School of Medicine, Pittsburgh, Pennsylvania, United States of America, 4 Molecular Genetics Laboratory, Institute for Ophthalmic Research, Centre for Ophthalmology, University of Tuebingen, Tuebingen, Germany ☯ These authors contributed equally to this work. ‡ OPEN ACCESS These authors are joint first authors on this work. * [email protected] (SGJ); [email protected] (AVC) Citation: Luo X, Cideciyan AV, Iannaccone A, Roman AJ, Ditta LC, Jennings BJ, et al. (2015) Blue Cone Monochromacy: Visual Function and Efficacy Abstract Outcome Measures for Clinical Trials. PLoS ONE 10(4): e0125700. doi:10.1371/journal.pone.0125700 Academic Editor: Dror Sharon, Hadassah-Hebrew University Medical Center, ISRAEL Background Blue Cone Monochromacy (BCM) is an X-linked retinopathy caused by mutations in the Received: December 29, 2014 OPN1LW / OPN1MW gene cluster, encoding long (L)- and middle (M)-wavelength sensitive Accepted: March 21, 2015 cone opsins. Recent evidence shows sufficient structural integrity of cone photoreceptors in Published: April 24, 2015 BCM to warrant consideration of a gene therapy approach to the disease. -

Hereditary Reversion Pigmentation of the Eyelids with Heterochromia of the Iris
874 LEE MASTEN FRANCIS enucleated. The following report on the Other cells were round with hyper- specimen was submitted from the New chromatic nuclei; while scattered thruout York State Institute for the Study of the tumor were large deeply staining Malignant Diseases: cells with one or two nuclei but free from The gross appearance of a cross sec- pigment. There were apparently two tion of the eye shows a tumor lying in types of pigmented cells, the one a large the lower temporal quadrant of the eye, irregular cell with long protoplasmic evidently springing from the choroid processes densely filled with fine yellow- near the margin of the optic disc. This ish granules, evidently chromatophores. tumor measured 15x10 mm. and was The other type of pigmented cell was a slightly nodular irregular ovoid tumor. evidently a tumor cell of the type men- The surface appeared smooth, was dark tioned above but containing fewer gran- gray in color and was of a soft consist- ules than the chromatophores. Thruout ency. The retina was markedly detached the tumor were small areas of hemor- and contained a clear serous fluid. Cross rhage and between the cells could be section of the tumor mass showed a demonstrated here and there, free pig- deeply pigmented homogeneous surface. ment granules. Microscopically, the tumor varied as From this picture, we would make a to the cellular constituents. There were diagnosis of malignant melanoma, fre- areas showing many pigment cells and quently called melanosarcoma, but by other areas almost free from the same. some authorities considered as melanotic The tumor was very vascular showing many fine capillaries around which in carcinoma. -
Genetic Defects of CHM and Visual Acuity Outcome in 24 Choroideremia
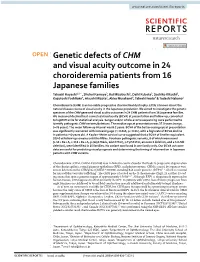
www.nature.com/scientificreports OPEN Genetic defects of CHM and visual acuity outcome in 24 choroideremia patients from 16 Japanese families Takaaki Hayashi1,2*, Shuhei Kameya3, Kei Mizobuchi2, Daiki Kubota3, Sachiko Kikuchi3, Kazutoshi Yoshitake4, Atsushi Mizota5, Akira Murakami6, Takeshi Iwata4 & Tadashi Nakano2 Choroideremia (CHM) is an incurable progressive chorioretinal dystrophy. Little is known about the natural disease course of visual acuity in the Japanese population. We aimed to investigate the genetic spectrum of the CHM gene and visual acuity outcomes in 24 CHM patients from 16 Japanese families. We measured decimal best-corrected visual acuity (BCVA) at presentation and follow-up, converted to logMAR units for statistical analysis. Sanger and/or whole-exome sequencing were performed to identify pathogenic CHM variants/deletions. The median age at presentation was 37.0 years (range, 5–76 years). The mean follow-up interval was 8.2 years. BCVA of the better-seeing eye at presentation was signifcantly worsened with increasing age (r = 0.515, p < 0.01), with a high rate of BCVA decline in patients > 40 years old. A Kaplan–Meier survival curve suggested that a BCVA of Snellen equivalent 20/40 at follow-up remains until the ffties. Fourteen pathogenic variants, 6 of which were novel [c.49 + 5G > A, c.116 + 5G > A, p.(Gly176Glu, Glu177Ter), p.Tyr531Ter, an exon 2 deletion, and a 5.0-Mb deletion], were identifed in 15 families. No variant was found in one family only. Our BCVA outcome data are useful for predicting visual prognosis and determining the timing of intervention in Japanese patients with CHM variants. -
Neuroophthalmology
Neuroophthalmology MAREK MICHALEC, MD PHD Clinic of Ophthalmology Faculty Hospital Brno and Masaryk University Version 12/2019 Content • Visual pathway affection • Diseases and affections of optic nerve • Optic chiasm pathology • Pathology of retrochiasmic part • Eye movement disorders • Binocular diplopia • Pupillary reaction abnormalities • Anisocoria • Combined disorders Examination - part I • Medical history • subjective (visual loss, diplopia) • When it started/ how long lasts it? • Does it change in time/ during the day? • Any progression? • What about the fellow eye? • Other signs? • Personal medical history? • Pharmacological history? • objective (pupillary dysfunction, eye movement disorders, ptosis of upper eyelid, red eye) Examination - part II • Visual acuity • Without and with correction • Monocular vision / binocular vision • Basic ophthalmological examination • Anterior segment (by slit lamp) • Posterior segment - arteficial mydriasis is essential (indirect ophthalmoscopy) • Visual field examination (static / kinetic perimetry) Examination - part III • Basic examination (GP) • Neurological examination • Intracranial conditions (including MRI) • neurological signs • Endocrinology • Thyroid associated orbitopathy / ophthalmopathy • Pituitary dysfunction Examination - part IV • Imaging techniques • Ultrasonography (eye bulb, orbit) • X-ray of skull (orbit, paranasal cavities) • Computerised Tomography of head (brain, skull bones, orbital bones) • MRI of head (brain, orbital structures) Optic nerve disorders Clinical signs • -

Color Blindness LEVELED BOOK • W a Reading A–Z Level W Leveled Book Word Count: 1,349 Color Blindness Connections Writing Choose Two Forms of Color Blindness
Color Blindness LEVELED BOOK • W A Reading A–Z Level W Leveled Book Word Count: 1,349 Color Blindness Connections Writing Choose two forms of color blindness. Write a report that compares the two conditions and their effects on a person’s life. Math Research the statistics about the number of people with the various forms of color blindness in your country. Organize your results in a pie chart. • W Q •T Written by Cheryl Reifsnyder Visit www.readinga-z.com for thousands of books and materials. www.readinga-z.com Words to Know Color ancestry molecules complementary photopigments cone cells prism Blindness defects retina genetic disorder rod cells hereditary wavelengths Photo Credits: Front cover, Back cover: © pretoperola/123RF; title page (Both): © shironosov/ iStock/Thinkstock; page 3: © Véronique Burger/Science Source; page 4 (Both): © Michael Shake/Dreamstime.com; page 5: © Designua/Dreamstime.com; page 6 (top): © Gunilla Elam/Science Source; page 6 (Bottom): © Steve Gschmeissner/Science Source; page 7 (Both): © Ted Kinsman/ Science Source; page 8 (left, Both): © anatchant/iStock/Thinkstock; page 8 (center, Both): © Nadezhda Bolotina/Hemera/Thinkstock; page 8 (right, Both): © iremphotography/iStock/Thinkstock; page 9 (all): © Popartic/iStock Editorial/Thinkstock; page 10: © RVN/Alamy Stock Photo; page 12: © Alexander Kaludov/123RF; page 13: © EnChroma; page 14: © Neitz LaBoratory; page 15: © Phanie/Alamy Stock Photo Written by Cheryl Reifsnyder www.readinga-z.com Focus Question Color Blindness Level W Leveled Book Correlation © Learning A–Z LEVEL W Written By Cheryl Reifsnyder What causes color blindness, and how Fountas & Pinnell S can it affect a person’s life? All rights reserved. -

An Update on Progress and the Changing Epidemiology of Causes of Childhood Blindness Worldwide
Major Articles An update on progress and the changing epidemiology of causes of childhood blindness worldwide Lingkun Kong, MD, PhD,a Melinda Fry, MPH,b Mohannad Al-Samarraie, MD,a Clare Gilbert, MD, FRCOphth,c and Paul G. Steinkuller, MDa PURPOSE To summarize the available data on pediatric blinding disease worldwide and to present current information on childhood blindness in the United States. METHODS A systematic search of world literature published since 1999 was conducted. Data also were solicited from each state school for the blind in the United States. RESULTS In developing countries, 7% to 31% of childhood blindness and visual impairment is avoidable, 10% to 58% is treatable, and 3% to 28% is preventable. Corneal opacification is the leading cause of blindness in Africa, but the rate has decreased significantly from 56% in 1999 to 28% in 2012. There is no national registry of the blind in the United States, and most schools for the blind do not maintain data regarding the cause of blindness in their students. From those schools that do have such information, the top three causes are cortical visual impairment, optic nerve hypoplasia, and retinopathy of prematurity, which have not changed in past 10 years. CONCLUSIONS There are marked regional differences in the causes of blindness in children, apparently based on socioeconomic factors that limit prevention and treatment schemes. In the United States, the 3 leading causes of childhood blindness appear to be cortical visual impairment, optic nerve hypoplasia, and retinopathy of prematurity; a national registry of the blind would allow accumulation of more complete and reliable data for accurate determination of the prevalence of each. -

Ocular Surface Changes Associated with Ophthalmic Surgery
Journal of Clinical Medicine Review Ocular Surface Changes Associated with Ophthalmic Surgery Lina Mikalauskiene 1, Andrzej Grzybowski 2,3 and Reda Zemaitiene 1,* 1 Department of Ophthalmology, Medical Academy, Lithuanian University of Health Sciences, 44037 Kaunas, Lithuania; [email protected] 2 Department of Ophthalmology, University of Warmia and Mazury, 10719 Olsztyn, Poland; [email protected] 3 Institute for Research in Ophthalmology, Foundation for Ophthalmology Development, 61553 Poznan, Poland * Correspondence: [email protected] Abstract: Dry eye disease causes ocular discomfort and visual disturbances. Older adults are at a higher risk of developing dry eye disease as well as needing for ophthalmic surgery. Anterior segment surgery may induce or worsen existing dry eye symptoms usually for a short-term period. Despite good visual outcomes, ocular surface dysfunction can significantly affect quality of life and, therefore, lower a patient’s satisfaction with ophthalmic surgery. Preoperative dry eye disease, factors during surgery and postoperative treatment may all contribute to ocular surface dysfunction and its severity. We reviewed relevant articles from 2010 through to 2021 using keywords “cataract surgery”, ”phacoemulsification”, ”refractive surgery”, ”trabeculectomy”, ”vitrectomy” in combina- tion with ”ocular surface dysfunction”, “dry eye disease”, and analyzed studies on dry eye disease pathophysiology and the impact of anterior segment surgery on the ocular surface. Keywords: dry eye disease; ocular surface dysfunction; cataract surgery; phacoemulsification; refractive surgery; trabeculectomy; vitrectomy Citation: Mikalauskiene, L.; Grzybowski, A.; Zemaitiene, R. Ocular Surface Changes Associated with Ophthalmic Surgery. J. Clin. 1. Introduction Med. 2021, 10, 1642. https://doi.org/ 10.3390/jcm10081642 Dry eye disease (DED) is a common condition, which usually causes discomfort, but it can also be an origin of ocular pain and visual disturbances. -
RETINAL DISORDERS Eye63 (1)
RETINAL DISORDERS Eye63 (1) Retinal Disorders Last updated: May 9, 2019 CENTRAL RETINAL ARTERY OCCLUSION (CRAO) ............................................................................... 1 Pathophysiology & Ophthalmoscopy ............................................................................................... 1 Etiology ............................................................................................................................................ 2 Clinical Features ............................................................................................................................... 2 Diagnosis .......................................................................................................................................... 2 Treatment ......................................................................................................................................... 2 BRANCH RETINAL ARTERY OCCLUSION ................................................................................................ 3 CENTRAL RETINAL VEIN OCCLUSION (CRVO) ..................................................................................... 3 Pathophysiology & Etiology ............................................................................................................ 3 Clinical Features ............................................................................................................................... 3 Diagnosis ......................................................................................................................................... -

Ministry of Public Health of Ukraine Ukrainian Medical Stomatological Academy
Ministry of Public Health of Ukraine Ukrainian Medical Stomatological Academy Approved At the meeting of the department of neurological diseases with neurosurgery and medical genetic "__"__ ____________20___ Protocol №________ Head of department _______________ prof. Delva M.Yu. METHODICAL INSTRUCTIONS FOR THE INDEPENDENT WORK OF STUDENTS FOR PREPARATION TO PRACTICAL CLASSES AND DURING PRACTICAL CLASSES Academic subject Neurology The module № 1 General neurology Topic Syndromes of defeat oculomotor nerves. Pathology of olfactory and visual analyzers. Year of study IV Faculty Foreign Students Training (Medicine) Poltava 20___ 1.Relevance of the topic: the olfactory and visual analyzers play a role in receptor function of the nervous system. With the functions of these disorders analyzers, as well as with oculomotor disturbances faced by doctors of different specialties - neurologists, ophthalmologists, neurosurgeons, pediatricians, phthisiatricians, endocrinologists, internists. Violations of the functions of these analyzers is observed in a variety of inflammatory, demyelinating processes, tumors, trauma, endocrine disorders. The correct methodological approach to the study of functions, pathological changes of the olfactory and visual analyzers, oculomotor nerves makes it possible to deliver topical and clinical diagnosis and treatment in a timely manner. 2. Specific Objectives: To investigate the function of I, II, III, IV, VI pairs of cranial nerves, identify signs of a lesion of the nerve disorder Examine the identification functions -

Theoretical Part Eye Examinations 1
Name and Surrname number Study group Theoretical part Eye examinations 1. Astigmatism Astigmatism is an optical defect in which vision is blurred due to the inability of the optics of the eye to focus a point object into a sharp focused image on the retina. Astigmatism can sometimes be asymptomatic, while higher degrees of astigmatism may cause symptoms such as blurry vision, squinting, eye strain, fatigue, or headaches. Types Regular astigmatism: Principal meridians are perpendicular. Simple astigmatism – the first focal line is on the retina, while the second is located behind the retina, or, the first focal line is in front of the retina, while the second is on the retina. Compound astigmatism – both focal lines are located behind or before the retina. Mixed astigmatism – focal lines are on both sides of the retina (straddling the retina). Irregular astigmatism: Principal meridians are not perpendicular. This type cannot be corrected by a lens. Tests Objective Refractometer, autorefractometer Placido keratoscope – A placido keratoscope consists of a handle and a circular part with a hole in the middle. The hole with a magnifying glass is viewed from a distance of 10–15 cm to the patients cornea. In the 200 mm wide circular portion there are concentric alternating black and white circles. They reflect the patient’s cornea. In the event of astigmatism, a deformation appears at the corresponding location. Sciascope Ophthalmometry Subjective Fuchs figure – This is a tool for evaluating astigmatism where examinee stands up against a pattern of circular shape (circular or striped rectangles) and fixes his/her gaze on the center of the pattern with one open eye. -

BOSTON TERRIER EYE DISEASE Corneal Ulcers and Prevention
BOSTON TERRIER EYE DISEASE Corneal Ulcers and Prevention Corneal Ulcers are the single largest eye problem in Boston Terriers. Perhaps 1 dog in 10 will experience a corneal ulcer sometime during its life based on the l903 dogs surveyed in the 2000 Boston Terrier Health Survey. The Boston Terrier Standard for the Breed calls for eyes to be “wide apart, large and round and dark in color. The eyes are set square in the skull and the outside corners are on a line with the cheeks as viewed from the front". The ideal Boston Terrier eye does not protrude but is "set square in the skull". Unfortunately the Boston eye is fairly prone to eye injury because of its large size and prominence. Corneal ulcers are caused initially by injury to the eyes. The common practice of removing Boston Terrier whiskers may be a reason that eyes become injured due to lack of sensory feelers. Some breeders do not trim whiskers once a dog's show career is finished because they know that whiskers can prevent injury to the eye. There are a number of external reasons why an injured eye doesn't heal. These may include irritation from eyelashes or from facial hairs, infection, and lack of moisture in the eye. Some of these reasons are hereditary. Internal reasons for an eye not healing include glaucoma and infection. Corneal ulcers can be difficult and expensive to treat and often result in the loss of the eye. This is a case where an "ounce of prevention is worth a pound of cure".