Computational Neuroimaging Strategies for Single Patient Predictions
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Steglitz-Zehlendorf
Bezirksamt Steglitz-Zehlendorf Steglitz-Zehlendorf Ein Wegweiser durch den Bezirk Sie fi nden uns 4x in Berlin Steglitz- Zehlendorf HIER SIND WIR ZUHAUSE · Versorgung aller Pfl egegrade · Abwechslungsreiches Beschäftigungs- · Spezielle Wohnbereiche für und Veranstaltungsangebot Menschen mit Demenz · Persönliche Möblierung ist gerne möglich Rufen Sie uns an oder kommen Sie vorbei, wir beraten Sie gerne persönlich und individuell. Infos zu unseren Veranstaltungen erhalten Sie im jeweiligen Haus. Vitanas Senioren Centrum Am Bäkepark Vitanas Senioren Centrum Schäferberg Bahnhofstraße 29 | 12207 Berlin Königstraße 25 – 27 | 14109 Berlin (030) 754 44 - 0 (030) 80 10 58 - 0 Vitanas Senioren Centrum Am Stadtpark Vitanas Senioren Centrum Rosengarten Stindestraße 31 | 12167 Berlin Preysingstraße 40 – 46 | 12249 Berlin (030) 92 90 16 - 0 (030) 766 85 - 5 www.vitanas.de Interview mit der Bezirksbürgermeisterin Cerstin Richter-Kotowski „Ich möchte den Menschen auf Augenhöhe begegnen!“ Athene-Grundschule angesprochen wurde, im Bürgertreffpunkt eine Ausstellung zu IM GESPRÄCH machen, habe ich mir Gedanken darüber gemacht, was ich als Lebenskundelehrerin mit meiner Klasse dazu beitragen kann. Ich habe mich gefragt, was ein Bürgertreff ist und nach einem Synonym dafür gesucht und bin auf den Begriff „Nachbarschaft“ ge- stoßen. Die Kinder sammelten zum Thema Nachbarschaft Wörter wie Toleranz, Hilfe, Unterstützung, Rücksichtnahme, Kommuni- kation, Alt und Jung zusammen, Sicherheit. Dabei war es wichtig, mit den Kindern die Unterschiede heraus zu arbeiten zwischen der Nachbarschaft, dort wo sie leben, und die der Schule. Damit die Kinder eine Vor- Eröffnung der Dahlem Route am 29.06.2018: stellung davon entwickeln konnten, was ein Henner Bunde, Staatssekretär der Senatsver- Bürgertreff ist, haben wir diesen im Bahn- waltung für Wirtschaft, Energie und Betriebe, Bezirksbürgermeisterin Cerstin Richter-Ko- hof Lichterfelde West besucht und dort Fo- towski und Marit Schützendübel, Direktorin tos gemacht. -

Und Informations-Dialog 2018 Baumaßnahmen Im Netz Der Berliner S-Bahn 2018 - 2020
2. Bau- und Informations-Dialog 2018 Baumaßnahmen im Netz der Berliner S-Bahn 2018 - 2020 DB Netz AG | I.NP-O-D-BLN(BS) + I.NM-O-F(S) | Berlin | 17.07.2018 Übersicht Regionalbereich Ost – Netz Berliner S-Bahn Bauschwerpunkte 2018 Ersatzneubau SÜ Rhinstraße + ESTW+ZBS S7 Ost SEV Lichtenberg–Springpfuhl/ Wuhletal Wochenenden April bis Juni + Dezember 2018 Brückenarbeiten S2 Nord + Neubau SÜ BAB114 SEV Lichtenberg–Ahrensfelde/ Wartenberg SEV Blankenburg–Karow + Blankenburg- 19.10.–25.10.2018 Schönfließ SEV Sprinpfuhl–Wartenberg/ Ahrensfelde 26.06.–16.07.2018 20.07.–23.07.2018 SEV Blankenburg–Buch + Blankenburg- Schönfließ 16.07.–23.07.2018 SEV Blankenburg–Buch Ersatzneubau 23.07.–17.08.2018 EÜ Thälmannstr. + Entflechtung S-/F- ZBS S5 West Schienenauswechslung Bahn Bf Strausberg SEV Westkreuz–Spandau SEV Tiergarten–Charlottenburg SEV Mahlsdorf– 13.08.–16.08.2018 (in Prüfung 23.07.-03.08.2017 Strausberg Nord Verschiebung IBN nach 01/2019) 23.11.–29.11.2018 Umbau Ostkreuz – Neubau Bahnsteig Karlshorst Ibn Endzustand 4-gleisigkeit SEV Rummelsburg–Wuhlheide ZBS S7 West + Begegnungsabschn. Potsdam SEV Ostkreuz–Karlshorst 06.07.–16.07.2018 SEV Wannsee–Potsdam 02.11.–12.11.2018 kein Verkehrshalt Karlshorst 03.08.–06.08. + 10.08.–13.08. + 14.12.–17.12.2018 SEV Alexanderplatz–Lichtenberg 06.07. – 06.08.2018 SEV Westkreuz–Wannsee + Babelsberg–Potsdam 02.11.–05.11. + 09.11.–12.11.2018 eingleisig Wuhlheide – Karlshorst 31.08.–03.09.2018 06.08. – 15.08.2018 SEV Westkreuz–Grunewald 16.11.–19.11.2018 Ende Neubau EÜ Sterndamm + Neubau PT Schöneweide bis 2021 bis 20.08.2018 halbseitg. -

Arbeitsgruppe „Stadtentwicklung Blankenburg“
Arbeitsgruppe „Stadtentwicklung Blankenburg“ Arbeitsgruppe „Stadtentwicklung Blankenburg“ Herr Regierender Bürgermeister von Berlin Michael Müller persönlich übergeben Offener Brief der Arbeitsgruppe „Stadtentwicklung Blankenburg“ _ Berlin, den 9. Februar 2017 Sehr geehrter Herr Regierender Bürgermeister von Berlin Michael Müller, sehr geehrter Herr Senator Geisel, sehr geehrter Herr Bezirksbürgermeister Köhne, sehr geehrte Bezirkstadträte, sehr geehrte Fraktionsvorsitzende der BVV Pankow, aus den Reihen des „Runden Tisches Blankenburg“ – einer bewährten Institution im Ortsteil Blankenburg, die die verschiedenen Interessen der Bewohner bündelt und auch dem Bezirksamt als kompetenter Ansprechpartner gilt – hat sich die Arbeitsgruppe „Stadtentwicklung Blankenburg“ konstituiert. Die Arbeitsgruppe hat sich zum Ziel gesetzt, den Entwicklungsprozess zur geplanten Erweiterung des Ortsteils Blankenburg auf den unbebauten Flächen entlang des Blankenburger Pflasterwegs bis hin zu den Ortsteilen Heinersdorf im Süden und Malchow (Bezirk Lichtenberg) konstruktiv zu begleiten und folgend Thesen und Forderungen formuliert. In den zur Zeit auf Senats- und Bezirksebene stattfindenden Diskussionen differieren die Angaben über die Bebauungsdichte, die Art der Bebauung und den Anteil der zukünftig in Anspruch genommenen Flächen ungemein. Zur Diskussion stehen Größenordnungen von 5.000 Wohneinheiten bis hin zu 15.000 Wohneinheiten. Der Ortsteil hat heute eine Einwohnerzahl von gut 6.000 Bewohnern – selbst die gedachte Untergrenze von 5.000 Wohneinheiten würde -

KLIMAVERANSTALTUNG Berlin – Die Grüne
Podiumsdiskussion Podiumsdiskussion KLIMAVERANSTALTUNG KLIMAVERANSTALTUNG Thema Thema Berlin – die Grüne Stadt der Zukunft? Berlin – die Grüne Stadt der Zukunft? Zeit und Ort Zeit und Ort Freitag, 16.04., 19.15 Uhr Freitag, 16.04., 19.15 Uhr Haus Berlin der Albert-Schweitzer-Stiftung Wohnen und Betreuen Haus Berlin der Albert-Schweitzer-Stiftung Wohnen und Betreuen Bahnhofstraße 32 Bahnhofstraße 32 13129 Berlin-Blankenburg 13129 Berlin-Blankenburg Städte und urbane Zentren verbrauchen 75% der weltweiten Energie und Städte und urbane Zentren verbrauchen 75% der weltweiten Energie und sind für 75% der globalen CO2-Emissionen verantwortlich. Was kann sind für 75% der globalen CO2-Emissionen verantwortlich. Was kann Berlin zur Reduzierung der Klimafolgen beitragen? Welche Auswirkun- Berlin zur Reduzierung der Klimafolgen beitragen? Welche Auswirkun- gen hat der Klimawandel für unser Leben in der Stadt? gen hat der Klimawandel für unser Leben in der Stadt? Es diskutieren: Es diskutieren: CHRISTOPH BALS (Germanwatch), KATRIN LOMPSCHER (Senatorin CHRISTOPH BALS (Germanwatch), KATRIN LOMPSCHER (Senatorin für Gesundheit, Umwelt und Verbraucherschutz), ULF SIEBERG für Gesundheit, Umwelt und Verbraucherschutz), ULF SIEBERG (BUND) und PROF. ANDREAS KNIE (Wissenschaftszentrum Berlin). (BUND) und PROF. ANDREAS KNIE (Wissenschaftszentrum Berlin). Moderation: DARIA CZARLINSKA. Moderation: DARIA CZARLINSKA. Die Podiumsdiskussion ist eine gemeinsame Veranstaltung der Zukunfts- Die Podiumsdiskussion ist eine gemeinsame Veranstaltung der Zukunfts- werkstatt -

Drucksache 19/16016 19
Deutscher Bundestag Drucksache 19/16016 19. Wahlperiode 17.12.2019 Antwort der Bundesregierung auf die Kleine Anfrage der Abgeordneten Stefan Gelbhaar, Daniela Wagner, Matthias Gastel, Stephan Kühn (Dresden) und der Fraktion BÜNDNIS 90/DIE GRÜNEN – Drucksache 19/15575 – Lärmschutzmaßnahmen der Deutschen Bahn entlang des Berliner Außenrings Vorbemerkung der Fragesteller Der östliche Berliner Außenring zwischen Karower und Grünauer Kreuz ge- hört laut Lärmkartierung durch das Eisenbahn-Bundesamt zu den Lärmbrenn- punkten des Schienenverkehrs in Berlin. Diese Bahntrasse ist insbesondere durch den nächtlichen Schienengüterverkehr belastet. Mit der Lärmsanierung an bestehenden Schienenwegen wurde 1999 ein Pro- gramm aufgelegt, welches den Lärm an hochbelasteten Streckenabschnitten deutlich reduzieren soll. Nach Absenkung der für die Lärmsanierung relevan- ten Pegel (Auslösewert) gilt seit Anfang 2019 ein aktualisiertes Gesamtkon- zept der Lärmsanierung, für das die Lärmsanierungsbedarfe neu berechnet wurden. Ferner wurde die zugehörige Förderrichtlinie fortgeschrieben (www. bmvi.de/SharedDocs/DE/Artikel/E/laermvorsorge-und-laermsanierung.html). Voraussetzung dafür, dass Maßnahmen durchgeführt werden, ist die Aufnah- me der entsprechenden Strecke in die Gesamtkonzeption der Lärmsanierung des Bundes. Dort, wo die Belastung besonders hoch ist und viele Anwohne- rinnen und Anwohner betroffen sind, sollen die Streckenabschnitte laut Eisenbahn-Bundesamt bevorzugt saniert werden. 1. Welche Projekte sind im aktuellen Lärmsanierungsprogramm des Bundes -

Übersicht Der Betriebsstellen Und Deren Abkürzungen Aus Der Richtlinie 100
Übersicht der Betriebsstellen und deren Abkürzungen aus der Richtlinie 100 XNTH `t Harde HADB Adelebsen KAHM Ahrweiler Markt YMMBM 6,1/60,3 Bad MGH HADH Adelheide MAIC Aich/Nbay KA Aachen Hbf MAD Adelschlag MAI Aichach KASZ Aachen Schanz NADM Adelsdf/Mittelfr TAI Aichstetten KAS Aachen Süd RADN Adelsheim Nord XCAI Aidyrlia KXA Aachen Süd Gr TAD Adelsheim Ost XSAL Aigle KAW Aachen West AADF Adendorf XFAB Aigueblanche KAW G Aachen West Gbf XUAJ Adjud XFAM Aime-la-Plagne KXAW Aachen West Gr XCAD Adler MAIN Ainring KAW P Aachen West Pbf DADO Adorf (Erzg) MAIL Aipl KAW W Aachen West Wk DADG Adorf (V) DB-Gr XIAE Airole KAG Aachen-Gemmenich DAD Adorf (Vogtl) XSAI Airolo XDA Aalborg TAF Affaltrach TAIB Aischbach XDAV Aalborg Vestby XSAA Affoltern Albis MAIT Aitrang TA Aalen XSAW Affoltern-Weier XFAX Aix-en-Prov TGV XBAAL Aalter MAGD Agatharied XFAI Aix-les-Bains XSA Aarau AABG Agathenburg XMAJ Ajka XSABO Aarburg-Oftring XFAG Agde XMAG Ajka-Gyartelep XDAR Aarhus H RAG Aglasterhausen LAK Aken (Elbe) XDARH Aarhus Havn XIACC Agliano-C C XOA Al XMAA Abaliget XIAG Agrigento Centr. XIAL Ala XCAB Abdulino RA Aha XIAO Alassio HABZ Abelitz EAHS Ahaus XIALB Alba KAB Abenden HAHN Ahausen XIALA Alba Adriatica MABG Abensberg WABG Ahlbeck Grenze XUAI Alba Iulia XMAH Abrahamhegy WABO Ahlbeck Ostseeth XIAT Albate Camerlata NAHF Aburg Hochschule HAHM Ahlem RAL Albbruck NAH G Aburg-Goldbach EAHL Ahlen (Westf) XIAB Albenga EDOBZ Abzw Dbw EAHLG Ahlen Gbf AAL Albersdorf HACC Accum EAHLH Ahlen Notbstg EABL Albersloh XFAC Acheres Triage HAHO Ahlhorn RAR Albersweiler(Pf) RAH Achern HAH Ahlshausen XFAL Albertville RAH H Achern Bstg HALT Ahlten FAG Albig RAH F Achern (F) FATC Ahnatal-Casselbr LALB Albrechtshaus RAHG Achern DB/SWEG FHEH Ahnatal-Heckersh FALS Albshausen XFAH Achiet FWEI Ahnatal-Weimar RAM Albsheim(Eis) HACH Achim MAHN Ahrain TAOM Albst.-Onstmett. -

Internet-Based Hedonic Indices of Rents and Prices for Flats: Example of Berlin
A Service of Leibniz-Informationszentrum econstor Wirtschaft Leibniz Information Centre Make Your Publications Visible. zbw for Economics Kholodilin, Konstantin A.; Mense, Andreas Working Paper Internet-based hedonic indices of rents and prices for flats: Example of Berlin DIW Discussion Papers, No. 1191 Provided in Cooperation with: German Institute for Economic Research (DIW Berlin) Suggested Citation: Kholodilin, Konstantin A.; Mense, Andreas (2012) : Internet-based hedonic indices of rents and prices for flats: Example of Berlin, DIW Discussion Papers, No. 1191, Deutsches Institut für Wirtschaftsforschung (DIW), Berlin This Version is available at: http://hdl.handle.net/10419/61399 Standard-Nutzungsbedingungen: Terms of use: Die Dokumente auf EconStor dürfen zu eigenen wissenschaftlichen Documents in EconStor may be saved and copied for your Zwecken und zum Privatgebrauch gespeichert und kopiert werden. personal and scholarly purposes. Sie dürfen die Dokumente nicht für öffentliche oder kommerzielle You are not to copy documents for public or commercial Zwecke vervielfältigen, öffentlich ausstellen, öffentlich zugänglich purposes, to exhibit the documents publicly, to make them machen, vertreiben oder anderweitig nutzen. publicly available on the internet, or to distribute or otherwise use the documents in public. Sofern die Verfasser die Dokumente unter Open-Content-Lizenzen (insbesondere CC-Lizenzen) zur Verfügung gestellt haben sollten, If the documents have been made available under an Open gelten abweichend von diesen Nutzungsbedingungen die in der dort Content Licence (especially Creative Commons Licences), you genannten Lizenz gewährten Nutzungsrechte. may exercise further usage rights as specified in the indicated licence. www.econstor.eu 1191 Discussion Papers Deutsches Institut für Wirtschaftsforschung 2012 Internet-Based Hedonic Indices of Rents and Prices for Flats Example of Berlin Konstantin A. -

Kleine Anfrage
Drucksache 16 / 13 357 Kleine Anfrage 16. Wahlperiode Kleine Anfrage der Abgeordneten Claudia Hämmerling (Bündnis 90/Die Grünen) vom 06. Mai 2009 (Eingang beim Abgeordnetenhaus am 07. Mai 2009) und Antwort Abwassererschließung im Raum Blankenburg Im Namen des Senats von Berlin beantworte ich Ihre Zu 2.: Verzögerungen haben sich insbesondere beim Kleine Anfrage wie folgt: Erwerb der Pumpwerksgrundstücke für die Gebiete Blan- kenburg, Stadtrandsiedlung Blankenfelde, Altsiedlung 1. Haben die vor zwei Jahren vorgestellten Planungen Heinersdorf und durch den Umgang mit vorhandenen zur weiteren Abwassererschließung im Raum Blanken- privaten Flurstücken innerhalb öffentlich gewidmeter burg und in den übrigen noch nicht kanalisierten Orts- Straßen ergeben. Für die Klärung der entsprechenden teilen Berlins weiterhin Bestand? Eigentumsverhältnisse ist ein hoher Zeitaufwand erforder- lich. Sind die Grundstückseigentümer festgestellt und Zu 1.: Das dem Abgeordnetenhaus von Berlin mit angeschrieben, gehen die Zustimmungen zur Benutzung Drucksache 16/1309 vom 18.03.2008 vorgelegte Erschlie- nur zögerlich bei den Berliner Wasserbetrieben ein. In ßungskonzept hat weiterhin Bestand und ist Grundlage den Gebieten Buchholz-West II, Altsiedlung Blankenburg der Objektplanung der Berliner Wasserbetriebe. und der Stadtrandsiedlung Blankenfelde sind hierdurch bereits Verzögerungen in der Objektplanung eingetreten, die zu veränderten Zeiten für den Baubeginn führen. Bis 2. Falls es Änderungen in der Zeitplanung gibt, zum Zeitpunkt der Ausschreibung der Bauleistungen welches sind die Gründe und wie ist die aktuelle Zeit- muss mit allen betroffenen Flurstückseigentümern Ein- planung? vernehmen zur Flurstücksinanspruchnahme bestehen. Im Siedlungsgebiet Blankenburg erhöhen sich die Er- schließungsaufwendungen infolge komplizierter Bau- grundverhältnisse erheblich. Die aktuelle Zeitplanung der Berliner Wasserbetriebe für die schmutzwassertechnische Erschließung der Alt- siedlungsgebiete ist der folgenden Tabelle zu entnehmen. -
02.07 Depth to the Water Table (Edition 2007)
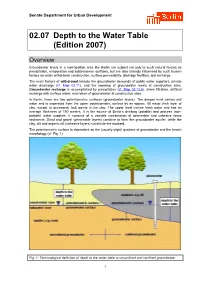
Senate Department for Urban Development 02.07 Depth to the Water Table (Edition 2007) Overview Groundwater levels in a metropolitan area like Berlin are subject not only to such natural factors as precipitation, evaporation and subterranean outflows, but are also strongly influenced by such human factors as water withdrawal, construction, surface permeability, drainage facilities, and recharge. The main factors of withdrawal include the groundwater demands of public water suppliers, private water discharge (cf. Map 02.11), and the lowering of groundwater levels at construction sites. Groundwater recharge is accomplished by precipitation (cf. Map 02.13.5), shore filtration, artificial recharge with surface water, and return of groundwater at construction sites. In Berlin, there are two potentiometric surfaces (groundwater layers). The deeper level carries salt water and is separated from the upper potentiometric surface by an approx. 80 meter thick layer of clay, except at occasional fault points in the clay. The upper level carries fresh water and has an average thickness of 150 meters. It is the source of Berlin’s drinking (potable) and process (non- potable) water supplies. It consists of a variable combination of permeable and cohesive loose sediments. Sand and gravel (permeable layers) combine to form the groundwater aquifer, while the clay, silt and organic silt (cohesive layers) constitute the aquitard. The potentiometric surface is dependent on the (usually slight) gradient of groundwater and the terrain morphology (cf. Fig. 1). Fig. 1: Terminological definition of depth to the water table at unconfined and confined groundwater 1 The depth to the water table is defined as the perpendicular distance between the upper edge of the surface and the upper edge of the groundwater surface. -

Nordkreuz–Karow Zweigleisiger Ausbau
Bestandsbauwerk Istzustand Ersatzneubau Sollzustand (Visualisierung) Impressum Projektdaten 2. Baustufe Herausgeber Streckenlänge (zweigleisig) 3,1 km DB Netz AG Einbau von neuen Gleisen 7,5 km Caroline-Michaelis-Straße 5-11 Weichen Neubau 15 10115 Berlin Bauweichen 4 Telefon: 030 297 554 18 Eisenbahnüberführungen Neubau 8 Stützweite zwischen 9,80 m und 20 m Änderungen vorbehalten Nordkreuz–Karow Einzelangaben ohne Gewähr Austausch der Oberleitung 4 km Stand Februar 2017 Aufbau Oberleitungs-Maste 180 Lärmschutzwände 8491 m Foto: Zweigleisiger Ausbau Titel Frank Kniestedt DB AG, 2. Ausbaustufe ESTW-A Einbindung Stellwerk Karow 1 Seite 3 Lothar Mantel Visualisierungen: DB AG Streckengeschwindigkeit 160 km/h bis Bahnhof Karow des Abschnitts Blankenburg–Karow Bauzeit 02/2017 bis 11/2020 Druckmanagement: DB Kommunikationstechnik GmbH Karlsruhe, www.dbkt.de www.bauprojekte.deutschebahn.com/p/berlin-gesundbrunnen-bernau Gethsemane- Friedhof, Nor r dend t Schönerlinder Straße aß Fr e KGA Gartenfr anzösisch Buchholz KGA Nor 2 A 10 Nor B la dend e n e .V. k aß N dlicht e eunde ö n riftstr T r f dlich e l d e M e r r Be S ü tr h L 1135 a l e r ß A 114 l n aße iner Ring e s str tr upt aß KGA Buchholzehemalige Ha e aße ptstr Hau aße L 1135 Schö er Str Bucher S A 10 nhau aus t hönh Bucher Straße raße ser Str Sc L 1135 aß Buch e er Straße L 1135 Berline 3 Marienstr r P S a t r nkg a ß e r a aße fens A 10 t r aße B ahn Nö r h dlicher B Stra of Bahnhof Berlin Karow ße s r t aß e e Richtung Rostock rliner Ri Ersatzneubau EÜ Rhönstraße Ersatzneubau Kreuzungsbauwerk -

18/1744 13.03.2019 18
Drucksache 18/1744 13.03.2019 18. Wahlperiode Antrag der Fraktion CDU Dauerstau beheben – Verkehrskollaps vermeiden: Entlastung der Stadt-Umland-Verkehre und der innerstädtischen Verkehre im Nordos- ten Berlins durch bedarfsgerechte ÖPNV-Angebote, den Ausbau der Verkehrsinfra- struktur und Fahrradschnellstraßen Das Abgeordnetenhaus wolle beschließen: Der Senat wird aufgefordert, den massiven aktuellen Verkehrsproblemen sowie dem drohenden vollständigen Verkehrskollaps im Berliner Nordosten unverzüglich in Zusammenarbeit mit dem Land Brandenburg durch die folgenden Maßnahmen zu begegnen: 1. Verbesserung der Leistungsfähigkeit der Verkehrswege durch: - Bau von Fahrradschnellstraßen, sogenannten "Fahrrad-Highways", ohne eine Re- duzierung der Leistungsfähigkeit bestehender Verkehrsstraßen (z.B. über die beste- henden Radialen) o Prüfung von Ebenen +1 Varianten über Greifswalder Straße /Berliner Allee, Prenzlauer Allee / Prenzlauer Promenade und -1 Varianten zur Unterquerung verkehrlich stark frequentierter Kreuzungspunkte - Optimierung des Verkehrsflusses der Stadtstraßen, insbesondere der hoch frequen- tierten Radialen Prenzlauer Allee, Schönhauser Allee, Greifswalder Straße mit ih- ren jeweiligen nord-östlichen Weiterführungen, sowie der überstark belasteten und Abgeordnetenhaus von Berlin Seite 2 Drucksache 18/1744 18. Wahlperiode deswegen täglich zugestauten Dorfdurchfahrungen, insbesondere Blankenburg, Karow, Heinersdorf und Malchow durch o verkehrsflussorientierte Schaltung von Ampelanlagen, die die aktuellen tages- zeit- und verkehrsstrombedingten -

Rahmenplanung Karow
Rahmenplanung Karow Dokumentation der zweiten öffentlichen Planungswerkstatt am 23. Februar 2019 Zweite offene Planungswerkstatt Karow – Dokumentation Impressum Auftraggeber: Bezirksamt Pankow von Berlin Abt. Stadtentwicklung und Bürgerdienste Stadtentwicklungsamt FB Stadtplanung Bearbeitet durch: nexus Institut für Kooperationsmanagement und interdisziplinäre Forschung GmbH Willdenowstraße 38 12203 Berlin Berlin, Mai 2019 Seite 1 von 51 Zweite offene Planungswerkstatt Karow – Dokumentation Inhaltsverzeichnis 1. Die Rahmenplanung Karow ............................................................................................ 3 1.1 Hintergründe und Ablauf der Rahmenplanung Karow .............................................. 3 1.2 Gemeinwohlinteresse - Beteiligungsrahmen und Rahmenbedingungen .................. 5 1.3 Öffentlichkeitsbeteiligung......................................................................................... 8 2 Die erste Beteiligungsphase ........................................................................................... 9 3 Die zweite offene Planungswerkstatt .............................................................................12 4 Ergebnisse der zweiten offenen Planungswerkstatt .......................................................16 4.1 Thema Verkehr ......................................................................................................28 4.2 Thema Freiräume ...................................................................................................41 4.3 Hinweise der