Non Part D/OTC Wrap Formulary
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
NOTE: the Following Are Shirley Ryan Abilitylab's Standard Charges As of Jan. 1, 2019. These Standard Charges Often Do Not
NOTE: The following are Shirley Ryan AbilityLab's standard charges as of Jan. 1, 2019. These standard charges often do not reflect what a patient or their insurance company/payer may be required to pay. Contact Patient Financial Services at 312-238-6039 for more information. Description Price 11-Deoxycortisol, Urine Random $531 12 Lead Ekg, Tracing Only $245 17 Hydroxycorticosteroids, Urine Timed $363 17 Hydroxyprogesterone, Serum $172 17 Ketosteroids, Urine Timed $273 17-Ketosteroids with Creatinine, Urine Random $273 2D Gait Analysis Charge(95999) $2,174 5' Nucleotidase, Serum $269 5.5 PDC PEDS CUFFED TRACH $226 5-HIAA-24 Hr Urine $99 A4566 Shoulder sling or vest design, abduction res $226 A4595 FES Electrode, each $38 A6545 Gradient Compression Wrap, Non-Elastic, Belo $171 ABO Rh Type $106 Above Knee Nylon Hose PR $83 Above Knee Suction Sheath $131 Above knee, for proximal femoral focal deficiency, $14,344 Above knee, molded socket, open end, SACH foot, en $10,751 Above knee, molded socket, single axis constant fr $10,935 Above knee, short prosthesis, no knee joint (""stu_L5210 $8,682 Above knee, short prosthesis, no knee joint (""stu_L5220 $7,429 ACAPELLA DH GREEN VIBRATORY PEP W/MOUTHPIECE DEVIC $181 Acetabuloplasty (27120) $4,493 Acetone, Serum $27 Acetylcholine Receptor Binding Antibody $405 Acid Phosphatase $66 Acid Phosphatase, Prostatic fraction $66 ACNE SURGERY MILIA CYSTS (10040) $530 Acorn Nebulizer $174 Activated PTT/Partial Thromboplastin Time $109 Active Wound Care > 20 cm Units $171 Active Wound Care/20 cm or < Units $171 Acupuncture with E-Stim. Each additional 15 minute $65 Acupuncture with E-Stim. -

Smoking Cessationreview Smoking Cessation YEARS Research Review MAKING EDUCATION EASY SINCE 2006
RESEARCH Smoking CessationREVIEW Smoking Cessation YEARS Research Review MAKING EDUCATION EASY SINCE 2006 Making Education Easy Issue 24 – 2016 In this issue: Welcome to issue 24 of Smoking Cessation Research Review. Encouraging findings suggest that varenicline may increase smoking abstinence rates in light smokers Have combustible cigarettes (5–10 cigarettes per day). However, since the study was conducted in a small cohort of predominantly White met their match? cigarette smokers, it will be interesting to see whether the results can be generalised to a larger population Supporting smokers with that is more representative of the real world. depression wanting to quit Computer-generated counselling letters that target smoking reduction effectively promote future cessation, Helping smokers quit after report European researchers. Their study enrolled smokers who did not intend to quit within the next diagnosis of a potentially 6 months. At the end of this 24-month investigation, 6-month prolonged abstinence was significantly higher curable cancer amongst smokers who received individually tailored letters compared with those who underwent follow-up assessments only. Preventing postpartum return to smoking We hope you enjoy the selection in this issue, and we welcome any comments or feedback. Varenicline assists smoking Kind Regards, cessation in light smokers Brent Caldwell Natalie Walker [email protected] [email protected] Novel pMDI doubles smoking quit rates Progress towards the Smokefree 2025 goal: too slow Independent commentary by Dr Brent Caldwell. Brent Caldwell was a Senior Research Fellow at Wellington Asthma Research Group, and worked on UK data show e-cigarettes are the Inhale Study. His main research interest is in identifying and testing improved smoking cessation linked to successful quitting methods, with a particular focus on clinical trials of new smoking cessation pharmacotherapies. -
Evaluating Disinfectants for Use Against the COVID-19 Virus
When it comes to choosing a disinfectant to combat the COVID-19 virus, research and health authorities suggest not all disinfectants are equally effective. The difference is in their active ingredient(s). HEALTH CANADA AND U.S. EPA ASSESSMENTS The work to evaluate disinfectants perhaps best starts with lists of approved disinfectants compiled by government health authorities. Health Canada has compiled a list of 85 hard surface disinfectant products (as of March 20, 2020) that meet their requirements for disinfection of emerging pathogens, including the virus that causes COVID-19. It can be accessed here. You can wade through the entire list. But if you locate the Drug Identification Number (DIN) on the disinfectant product label or the safety data sheet (SDS), then you can use the search function to quickly see if the product meets Health Canada requirements. A second list, updated on March 19, 2020, provides 287 products that meet the U.S. Environmental Protection Agency’s (EPA) criteria for use against SARS-CoV-2, the novel coronavirus that causes the disease COVID-19. This list can be found here. Like the Health Canada list, you can wade through this one too. However, to best use this list, you should locate the U.S. EPA registration number on the product label or SDS, and use that number to search the list. The U.S. EPA registration number of a product consists of two sets of numbers separated by a hyphen. The first set of numbers refers to the company identification number, and the second set of numbers following the hyphen represents the product number. -

FDA-2015-N-0101; and FDA-2016-N-0124
DE PARTMENT OF HEALTH AND HUMAN SERVICES Food and Drug Administration Silver Spring MD 20993 November 18, 2020 Docket Nos. FDA-1975-N-0012; FDA-2015-N-0101; and FDA-2016-N-0124 The American Cleaning Institute Attention: James Kim, PhD Vice President, Science and Regulatory Affairs 1401 H Street, N.W. Suite 700 Washington, D.C. 20005 Re: Benzalkonium Chloride, Benzethonium Chloride, Chloroxylenol, Ethanol, and Povidone-Iodine Dear Dr. Kim: This letter responds to The American Cleaning Institute’s (ACI’s) July 14, 2020 communication regarding the deferral from final rulemaking under the over-the-counter (OTC) Drug Review on benzalkonium chloride, benzethonium chloride, chloroxylenol, ethanol, and povidone-iodine for use in nonprescription (often referred to as over-the-counter or OTC) consumer antiseptic wash, health care antiseptic, and consumer antiseptic rub drug products. In March 2016, FDA issued letters granting requests to defer three active ingredients— benzalkonium chloride, benzethonium chloride, and chloroxylenol—from inclusion in the final rulemaking for the December 2013 proposed rule for OTC consumer antiseptic washes (78 FR 76444). Similarly, in January 2017, FDA issued letters granting requests to defer six active ingredients—benzalkonium chloride, benzethonium chloride, chloroxylenol, ethanol, povidone- iodine, and isopropyl alcohol—from inclusion in the final rulemaking for the May 2015 proposed rule for OTC health care antiseptics (80 FR 25166). In October 2017, FDA issued letters granting requests to defer three active -

Healthy Mouth, Healthy You the Connection Between Oral and Overall Health
Healthy Mouth, Healthy You The connection between oral and overall health Your dental health is part of a bigger picture: whole-body wellness. Learn more about the relationship between your teeth, gums and the rest of your body. We keep you smiling® deltadentalins.com/enrollees Pregnancy Pregnancy is a crucial time to take care of your oral health. Hormonal changes may increase the risk of gingivitis, or inflammation of the gums. Symptoms include tenderness, swelling and bleeding of the gums. Without proper care, these problems may become more serious and can lead to gum disease. Gum disease is linked to premature birth and low birth weight. If you notice any changes in your mouth during pregnancy, see your dentist. WHAT YOU CAN DO • Be vigilant about your oral health. Brush twice daily and floss at least once a day — these basic oral health practices will help reduce plaque buildup and keep your mouth healthy. • Talk to your dentist. Always let your dentist know that you are pregnant. • Eat well. Choose nutritious, well-balanced meals, including fresh fruits, raw vegetables and dairy products. Athletics Sports and exercise are great ways to build muscle and improve cardiovascular health, but they can also increase risks to your oral health. Intense exercise can dry out the mouth, leading to a greater chance of tooth decay. If you play a high-impact sport without proper protection, you risk knocking out a tooth or dislocating your jaw. WHAT YOU CAN DO • Hydrate early. Prevent dehydration by drinking water during your workout — and several hours beforehand. • Skip the sports drinks. -

July 2021 L.A. Care Health Plan Medi-Cal Dual Formulary
L.A. Care Health Plan Medi-Cal Dual Formulary Formulary is subject to change. All previous versions of the formulary are no longer in effect. You can view the most current drug list by going to our website at http://www.lacare.org/members/getting-care/pharmacy-services For more details on available health care services, visit our website: http://www.lacare.org/members/welcome-la-care/member-documents/medi-cal LA1308E 02/20 EN lacare.org Last Updated: 07/01/2021 INTRODUCTION Foreword Te L.A. Care Health Plan (L.A. Care) Medi-Cal Dual formulary is a preferred list of covered drugs, approved by the L.A. Care Health Plan Pharmacy Quality Oversight Committee. Tis formulary applies only to outpatient drugs and self-administered drugs not covered by your Medicare Prescription Drug Beneft. It does not apply to medications used in the inpatient setting or medical ofces. Te formulary is a continually reviewed and revised list of preferred drugs based on safety, clinical efcacy, and cost-efectiveness. Te formulary is updated on a monthly basis and is efective the frst of every month. Tese updates may include, and are not limited to, the following: (i) removal of drugs and/or dosage forms, (ii) changes in tier placement of a drug that results in an increase in cost sharing, and (iii) any changes of utilization management restrictions, including any additions of these restrictions. Updated documents are available online at: lacare.org/members/getting-care/pharmacy-services. If you have questions about your pharmacy coverage, call Customer Solutions Center at 1-888-839-9909 (TTY 711), available 24 hours a day, 7 days a week. -

Which Disinfectants Work Best Against C. Difficile?
Science at Your Doorstep WHICH DISINFECTANTS WORK BEST AGAINST C. DIFFICILE? Summary: In healthcare facilities, Clostridium difficile infections spread by transmission of bacterial spores. Appropriate sporicidal disinfectants are needed to prevent development of clusters and outbreaks. In this study, researchers in The Netherlands compared the effectiveness of 4 different disinfectant classes on killing distinctive C. difficile spores. They published their results in the respected journal, Antimicrobial Resistance & Infection Control. Hydrogen peroxide disinfectant wipes showed the highest bactericidal activity. Publication Description: According to the study, a dilution of sodium hypochlorite (chlorine bleach) has historically been used in hospitals to disinfect areas contaminated with C. difficile spores. But the authors state that “hypochlorite has to be used in excessive concentrations to be effective, thereby increasing its toxic and corrosive properties.” So the authors searched for alternative disinfectant types to eliminate C. difficile spores. The 4 different disinfectant compounds tested were: 1. Glucoprotamin 2. Hydrogen peroxide 3. Ethanol/propane/amino propyl glycine 4. Didecyldimonium chloride/benzalkonium chloride/biguanide (quat) Tiles were contaminated with a solution containing 5x106 CFU/ml spores of C. difficile. The tiles were left to dry for an hour and then wiped or sprayed with one of the sprays or wipes as intended by the manufacturers. After 5 minutes, microbiological cultures were performed. Conclusion: The authors concluded that for each active ingredient, the wipes performed better than the sprays. In general, impregnated cleaning/disinfection wipes performed better than ready-to-use sprays. Wipes with hydrogen peroxide showed the highest bactericidal activity. Reference: See article at: Antimicrobial Resistance & Infection Control; Volume 6, No. -

Chewable Lozenge Formulation
Umashankar M S et al. Int. Res. J. Pharm. 2016, 7 (4) INTERNATIONAL RESEARCH JOURNAL OF PHARMACY www.irjponline.com ISSN 2230 – 8407 Review Article CHEWABLE LOZENGE FORMULATION- A REVIEW Umashankar M S *, Dinesh S R, Rini R, Lakshmi K S, Damodharan N SRM College of Pharmacy, SRM University, Kattankulathur, India *Corresponding Author Email: [email protected] Article Received on: 11/02/16 Revised on: 13/03/16 Approved for publication: 28/03/16 DOI: 10.7897/2230-8407.07432 ABSTRACT Development of lozenges dated back to 20thcentury and is still remain popular among the consumer and hence it has continued commercial production. Lozenges are palatable solid unit dosage form administrated in the oral cavity. They meant to be dissolved in mouth or pharynx for its local or systemic effect. Lozenge tablets provide several advantages as pharmaceutical formulations however with some disadvantages. Lozenge as a dosage form can be adopted for drug delivery across buccal route, labial route, gingival route and sublingual route. Multiple drugs can also be incorporated in them for chronic illness treatments. Lozenge enables loading of wide range of active ingredients for oral systemic delivery of drugs. Lozenges are available as over the counter medications in the form of caramel based soft lozenges, hard candy lozenges and compressed tablet lozenges containing drugs for sore throat, mouth infection and as mouth fresheners. The rationale behind the use of medicated lozenges as one of the most favored dosage form for the delivery of antitussive drugs. This review focuses various aspects of lozenge formulation providing an insight to the formulation scientist on novel application of lozenge drug delivery system. -
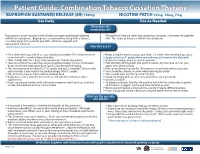
Bupropion + Patch
Patient Guide: Combination Tobacco Cessation Therapy BUPROPION SUSTAINED RELEASE (SR) 150mg NICOTINE PATCH 21mg, 14mg, 7mg Use Daily Use As Needed What does this medication do? Bupropion is a non-nicotine aid that helps you quit smoking by reducing The patch will release small, but continuous amounts of nicotine through the withdrawal symptoms. Bupropion is recommended along with a tobacco skin. This helps to decrease withdrawal symptoms. cessation program to provide you with additional support and educational materials. How do I use it? BUPROPION SUSTAINED RELEASE (SR) 150mg NICOTINE PATCH 21mg, 14mg, 7mg Set a date when you intend to stop smoking (quit date). The medicine needs Begin using the patch on your quit date, 1-2 weeks after starting bupropion. to be started 1-2 weeks before that date. Apply only one (1) patch when you wake up and remove the old patch. Take 1 tablet daily for 3 days, then increase to 1 tablet twice daily. If you miss a dose, use it as soon as you can. Take at a similar time each day, allowing approximately 8 hours in between Peel the back off the patch and put it on clean, dry, hair-free skin on your doses. Don’t take bupropion past 5pm to avoid trouble sleeping. upper arm, chest or back. This medicine may be taken for 7-12 weeks and up to 6 months. Discuss with Press patch firmly in place for 10 seconds so it will stick well to your skin. your provider if you need to be treated longer than 12 weeks. -

Clinical Excellence Series Volume VI an Evidence-Based Approach to Infectious Disease
Clinical Excellence Series n Volume VI An Evidence-Based Approach To Infectious Disease Inside The Young Febrile Child: Evidence-Based Diagnostic And Therapeutic Strategies Pharyngitis In The ED: Diagnostic Challenges And Management Dilemmas HIV-Related Illnesses: The Challenge Of Emergency Department Management Antibiotics In The ED: How To Avoid The Common Mistake Of Treating Not Wisely, But Too Well Brought to you exclusively by the publisher of: An Evidence-Based Approach To Infectious Disease CEO: Robert Williford President & Publisher: Stephanie Ivy Associate Editor & CME Director: Jennifer Pai • Associate Editor: Dorothy Whisenhunt Director of Member Services: Liz Alvarez • Marketing & Customer Service Coordinator: Robin Williford Direct all questions to EB Medicine: 1-800-249-5770 • Fax: 1-770-500-1316 • Non-U.S. subscribers, call: 1-678-366-7933 EB Medicine • 5550 Triangle Pkwy Ste 150 • Norcross, GA 30092 E-mail: [email protected] • Web Site: www.ebmedicine.net The Emergency Medicine Practice Clinical Excellence Series, Volume Volume VI: An Evidence-Based Approach To Infectious Disease is published by EB Practice, LLC, d.b.a. EB Medicine, 5550 Triangle Pkwy Ste 150, Norcross, GA 30092. Opinions expressed are not necessarily those of this publication. Mention of products or services does not constitute endorsement. This publication is intended as a general guide and is intended to supplement, rather than substitute, professional judgment. It covers a highly technical and complex subject and should not be used for making specific medical decisions. The materials contained herein are not intended to establish policy, procedure, or standard of care. Emergency Medicine Practice, The Emergency Medicine Practice Clinical Excellence Series, and An Evidence-Based Approach To Infectious Disease are trademarks of EB Practice, LLC, d.b.a. -
Use of Non Cigarette Tobacco Products (NCTP) Smokeless
Non Cigarette Tobacco Products (NCTP) and Electronic cigarettes (e-cigs) Michael V. Burke EdD Asst: Professor of Medicine Nicotine Dependence Center Mayo Clinic, Rochester, MN Email: [email protected] ©2011 MFMER | slide-1 Goals & Objectives • Review NCTP definitions & products • Discuss prevalence/trends of NCTP • Discuss NCTP and addiction • Review recommended treatments for NCTP ©2011 MFMER | slide-2 NCTP Definitions & Products ©2011 MFMER | slide-3 Pipes ©2011 MFMER | slide-4 Cigars Images from www.trinketsandtrash.org ©2011 MFMER | slide-5 Cigar Definition U.S. Department of Treasury (1996): Cigar “Any roll of tobacco wrapped in leaf tobacco or any substance containing tobacco.” vs. Cigarette “Any roll of tobacco wrapped in paper or in any substance not containing tobacco.” ©2011 MFMER | slide-6 NCI Monograph 9. Cigars: Health Effects and Trends. ©2011 MFMER | slide-7 ©2011 MFMER | slide-8 Smokeless Tobacco Chewing tobacco • Loose leaf (i.e., Redman) • Plugs • Twists Snuff • Moist (i.e., Copenhagen, Skoal) • Dry (i.e., Honest, Honey bee, Navy, Square) ©2011 MFMER | slide-9 “Chewing Tobacco” = Cut tobacco leaves ©2011 MFMER | slide-10 “Snuff” = Moist ground tobacco ©2011 MFMER | slide-11 Type of ST Used in U.S. Chewing Tobacco Snuff National Survey on Drug Use and Health (NSDUH) ©2011 MFMER | slide-12 “Spitless Tobacco” – Star Scientific ©2011 MFMER | slide-13 RJ Reynold’s ©2011 MFMER | slide-14 “Swedish Style” ST ©2011 MFMER | slide-15 Phillip Morris (Altria) ©2011 MFMER | slide-16 New Product: “Fully Dissolvables” ©2011 MFMER -

Transdermal Nicotine Maintenance Attenuates the Subjective And
Neuropsychopharmacology (2004) 29, 991–1003 & 2004 Nature Publishing Group All rights reserved 0893-133X/04 $25.00 www.neuropsychopharmacology.org Transdermal Nicotine Maintenance Attenuates the Subjective and Reinforcing Effects of Intravenous Nicotine, but not Cocaine or Caffeine, in Cigarette-Smoking Stimulant Abusers 1 1 ,1,2 Bai-Fang X Sobel , Stacey C Sigmon and Roland R Griffiths* 1Department of Psychiatry and Behavioral Science, Johns Hopkins University School of Medicine, Baltimore, MD, USA; 2Department of Neuroscience, Johns Hopkins University School of Medicine, Baltimore, MD, USA The effects of transdermal nicotine maintenance on the subjective, reinforcing, and cardiovascular effects of intravenously administered cocaine, caffeine, and nicotine were examined using double-blind procedures in nine volunteers with histories of using tobacco, caffeine, and cocaine. Each participant was exposed to two chronic drug maintenance phases (21 mg/day nicotine transdermal patch and placebo transdermal patch). Within each drug phase, the participant received intravenous injections of placebo, cocaine (15 and 30 mg/70 kg), caffeine (200 and 400 mg/70 kg), and nicotine (1.0 and 2.0 mg/70 kg) in mixed order across days. Subjective and cardiovascular data were collected before and repeatedly after drug or placebo injection. Reinforcing effects were also assessed after each injection with a Drug vs Money Multiple-Choice Form. Intravenous cocaine produced robust dose-related increases in subjective and reinforcing effects; these effects were not altered by nicotine maintenance. Intravenous caffeine produced elevations on several subjective ratings; nicotine maintenance did not affect these ratings. Under the placebo maintenance condition, intravenous nicotine produced robust dose-related subjective effects, with maximal increases similar to the high dose of cocaine; nicotine maintenance significantly decreased the subjective and reinforcing effects of intravenous nicotine.