Use of Non Cigarette Tobacco Products (NCTP) Smokeless
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Concurrent Alcohol and Tobacco Dependence
Concurrent Alcohol and Tobacco Dependence Mechanisms and Treatment David J. Drobes, Ph.D. People who drink alcohol often also smoke and vice versa. Several mechanisms may contribute to concurrent alcohol and tobacco use. These mechanisms include genes that are involved in regulating certain brain chemical systems; neurobiological mechanisms, such as cross-tolerance and cross-sensitization to both drugs; conditioning mechanisms, in which cravings for alcohol or nicotine are elicited by certain environmental cues; and psychosocial factors (e.g., personality characteristics and coexisting psychiatric disorders). Treatment outcomes for patients addicted to both alcohol and nicotine are generally worse than for people addicted to only one drug, and many treatment providers do not promote smoking cessation during alcoholism treatment. Recent findings suggest, however, that concurrent treatment for both addictions may improve treatment outcomes. KEY WORDS: comorbidity; AODD (alcohol and other drug dependence); alcoholic beverage; tobacco in any form; nicotine; smoking; genetic linkage; cross-tolerance; AOD (alcohol and other drug) sensitivity; neurotransmitters; brain reward pathway; cue reactivity; social AODU (AOD use); cessation of AODU; treatment outcome; combined modality therapy; literature review lcohol consumption and tobacco ers who are dependent on nicotine Department of Health and Human use are closely linked behaviors. have a 2.7 times greater risk of becoming Services 1989). The concurrent use of A Thus, not only are people who alcohol dependent than nonsmokers both drugs by pregnant women can drink alcohol more likely to smoke (and (e.g., Breslau 1995). Finally, although also result in more severe prenatal dam- vice versa) but also people who drink the smoking rate in the general popula age and neurocognitive deficits in their larger amounts of alcohol tend to smoke tion has gradually declined over the offspring than use of either drug alone more cigarettes. -

Smoking Cessationreview Smoking Cessation YEARS Research Review MAKING EDUCATION EASY SINCE 2006
RESEARCH Smoking CessationREVIEW Smoking Cessation YEARS Research Review MAKING EDUCATION EASY SINCE 2006 Making Education Easy Issue 24 – 2016 In this issue: Welcome to issue 24 of Smoking Cessation Research Review. Encouraging findings suggest that varenicline may increase smoking abstinence rates in light smokers Have combustible cigarettes (5–10 cigarettes per day). However, since the study was conducted in a small cohort of predominantly White met their match? cigarette smokers, it will be interesting to see whether the results can be generalised to a larger population Supporting smokers with that is more representative of the real world. depression wanting to quit Computer-generated counselling letters that target smoking reduction effectively promote future cessation, Helping smokers quit after report European researchers. Their study enrolled smokers who did not intend to quit within the next diagnosis of a potentially 6 months. At the end of this 24-month investigation, 6-month prolonged abstinence was significantly higher curable cancer amongst smokers who received individually tailored letters compared with those who underwent follow-up assessments only. Preventing postpartum return to smoking We hope you enjoy the selection in this issue, and we welcome any comments or feedback. Varenicline assists smoking Kind Regards, cessation in light smokers Brent Caldwell Natalie Walker [email protected] [email protected] Novel pMDI doubles smoking quit rates Progress towards the Smokefree 2025 goal: too slow Independent commentary by Dr Brent Caldwell. Brent Caldwell was a Senior Research Fellow at Wellington Asthma Research Group, and worked on UK data show e-cigarettes are the Inhale Study. His main research interest is in identifying and testing improved smoking cessation linked to successful quitting methods, with a particular focus on clinical trials of new smoking cessation pharmacotherapies. -

Other Tobacco Products (OTP) Are Products Including Smokeless and “Non-Cigarette” Materials
Other tobacco products (OTP) are products including smokeless and “non-cigarette” materials. For more information on smoking and how to quit using tobacco products, check out our page on tobacco. A tobacco user may actually absorb more nicotine from chewing tobacco or snuff than they do from a cigarette (Mayo Clinic). The health consequences of smokeless tobacco use include oral, throat and pancreatic cancer, tooth loss, gum disease and increased risk of heart disease, heart attack and stroke. (American Cancer Society, “Smokeless Tobacco” 2010) Smokeless tobacco products contain at least 28 cancer-causing agents. The risk of certain types of cancer increases with smokeless tobacco: Esophageal cancer, oral cancer (cancer of the mouth, throat, cheek, gums, lips, tongue). Other Tobacco Products (OTP) Include: Chewing/Spit Tobacco A smokeless tobacco product consumed by placing a portion of the tobacco between the cheek and gum or upper lip teeth and chewing. Must be manually crushed with the teeth to release flavor and nicotine. Spitting is required to get rid of the unwanted juices. Loose Tobacco Loose (pipe) tobacco is made of cured and dried leaves; often a mix of various types of leaves (including spiced leaves), with sweeteners and flavorings added to create an "aromatic" flavor. The tobacco used resembles cigarette tobacco, but is more moist and cut more coarsely. Pipe smoke is usually held in the mouth and then exhaled without inhaling into the lungs. Blunt Wraps Blunt wraps are hollowed out tobacco leaf to be filled by the consumer with tobacco (or other drugs) and comes in different flavors. Flavors are added to create aromas and flavors. -

Nicotine and Methylphenidate Chornic Exposure on Adult Cannabinoid Receptor Agonist (Cp 55,940) Place Conditioning in Male Rats
California State University, San Bernardino CSUSB ScholarWorks Electronic Theses, Projects, and Dissertations Office of aduateGr Studies 6-2016 NICOTINE AND METHYLPHENIDATE CHORNIC EXPOSURE ON ADULT CANNABINOID RECEPTOR AGONIST (CP 55,940) PLACE CONDITIONING IN MALE RATS Christopher P. Plant California State University - San Bernardino Follow this and additional works at: https://scholarworks.lib.csusb.edu/etd Part of the Biological Psychology Commons, and the Clinical Psychology Commons Recommended Citation Plant, Christopher P., "NICOTINE AND METHYLPHENIDATE CHORNIC EXPOSURE ON ADULT CANNABINOID RECEPTOR AGONIST (CP 55,940) PLACE CONDITIONING IN MALE RATS" (2016). Electronic Theses, Projects, and Dissertations. 339. https://scholarworks.lib.csusb.edu/etd/339 This Thesis is brought to you for free and open access by the Office of aduateGr Studies at CSUSB ScholarWorks. It has been accepted for inclusion in Electronic Theses, Projects, and Dissertations by an authorized administrator of CSUSB ScholarWorks. For more information, please contact [email protected]. NICOTINE AND METHYLPHENIDATE CHRONIC EXPOSURE ON ADULT CANNABINOID RECEPTOR AGONIST (CP 55,940) PLACE CONDITIONING IN MALE RATS A Thesis Presented to the Faculty of California State University, San Bernardino In Partial Fulfillment of the Requirements for the Degree Master of Arts in General-Experimental Psychology by Christopher Philip Plant June 2016 NICOTINE AND METHYLPHENIDATE CHRONIC EXPOSURE ON ADULT CANNABINOID RECEPTOR AGONIST (CP 55,940) PLACE CONDITIONING IN MALE -

Model Ordinance Prohibiting Smoking in All Workplaces and Public Places (100% Smokefree)
Model Ordinance Prohibiting Smoking in All Workplaces and Public Places (100% Smokefree) Sec. 1000. Title This Article shall be known as the _______________ [name of City or County] Smokefree Air Ordinance of ______ [year]. Sec. 1001. Findings and Intent The _______________ [City or County Governing Body] does hereby find that: The 2006 U.S. Surgeon General's Report, The Health Consequences of Involuntary Exposure to Tobacco Smoke, has concluded that (1) secondhand smoke exposure causes disease and premature death in children and adults who do not smoke; (2) children exposed to secondhand smoke are at an increased risk for sudden infant death syndrome (SIDS), acute respiratory problems, ear infections, and asthma attacks, and that smoking by parents causes respiratory symptoms and slows lung growth in their children; (3) exposure of adults to secondhand smoke has immediate adverse effects on the cardiovascular system and causes coronary heart disease and lung cancer; (4) there is no risk-free level of exposure to secondhand smoke; (5) establishing smokefree workplaces is the only effective way to ensure that secondhand smoke exposure does not occur in the workplace, because ventilation and other air cleaning technologies cannot completely control for exposure of nonsmokers to secondhand smoke; and (6) evidence from peer-reviewed studies shows that smokefree policies and laws do not have an adverse economic impact on the hospitality industry.1 According to the 2010 U.S. Surgeon General's Report, How Tobacco Smoke Causes Disease, even occasional exposure to secondhand smoke is harmful and low levels of exposure to secondhand tobacco smoke lead to a rapid and sharp increase in dysfunction and inflammation of the lining of the blood vessels, which are implicated in heart attacks and stroke.2 According to the 2014 U.S. -

"I Always Thought They Were All Pure Tobacco'': American
“I always thought they were all pure tobacco”: American smokers’ perceptions of “natural” cigarettes and tobacco industry advertising strategies Patricia A. McDaniel* Department of Social and Behavioural Sciences, School of Nursing University of California, San Francisco 3333 California Street, Suite 455 San Francisco, CA 94118 USA work: (415) 514-9342 fax: (415) 476-6552 [email protected] Ruth E. Malone Department of Social and Behavioral Sciences, School of Nursing University of California, San Francisco, USA *Corresponding author The Corresponding Author has the right to grant on behalf of all authors and does grant on behalf of all authors, an exclusive licence (or non exclusive for government employees) on a worldwide basis to the BMJ Publishing Group Ltd and its Licensees to permit this article (if accepted) to be published in Tobacco Control editions and any other BMJPGL products to exploit all subsidiary rights, as set out in our licence (http://tc.bmj.com/misc/ifora/licence.pdf). keywords: natural cigarettes, additive-free cigarettes, tobacco industry market research, cigarette descriptors Word count: 223 abstract; 6009 text 1 table, 3 figures 1 ABSTRACT Objective: To examine how the U.S. tobacco industry markets cigarettes as “natural” and American smokers’ views of the “naturalness” (or unnaturalness) of cigarettes. Methods: We reviewed internal tobacco industry documents, the Pollay 20th Century Tobacco Ad Collection, and newspaper sources, categorized themes and strategies, and summarized findings. Results: Cigarette advertisements have used the term “natural” since at least 1910, but it was not until the 1950s that “natural” referred to a core element of brand identity, used to describe specific product attributes (filter, menthol, tobacco leaf). -

Healthy Mouth, Healthy You the Connection Between Oral and Overall Health
Healthy Mouth, Healthy You The connection between oral and overall health Your dental health is part of a bigger picture: whole-body wellness. Learn more about the relationship between your teeth, gums and the rest of your body. We keep you smiling® deltadentalins.com/enrollees Pregnancy Pregnancy is a crucial time to take care of your oral health. Hormonal changes may increase the risk of gingivitis, or inflammation of the gums. Symptoms include tenderness, swelling and bleeding of the gums. Without proper care, these problems may become more serious and can lead to gum disease. Gum disease is linked to premature birth and low birth weight. If you notice any changes in your mouth during pregnancy, see your dentist. WHAT YOU CAN DO • Be vigilant about your oral health. Brush twice daily and floss at least once a day — these basic oral health practices will help reduce plaque buildup and keep your mouth healthy. • Talk to your dentist. Always let your dentist know that you are pregnant. • Eat well. Choose nutritious, well-balanced meals, including fresh fruits, raw vegetables and dairy products. Athletics Sports and exercise are great ways to build muscle and improve cardiovascular health, but they can also increase risks to your oral health. Intense exercise can dry out the mouth, leading to a greater chance of tooth decay. If you play a high-impact sport without proper protection, you risk knocking out a tooth or dislocating your jaw. WHAT YOU CAN DO • Hydrate early. Prevent dehydration by drinking water during your workout — and several hours beforehand. • Skip the sports drinks. -

July 2021 L.A. Care Health Plan Medi-Cal Dual Formulary
L.A. Care Health Plan Medi-Cal Dual Formulary Formulary is subject to change. All previous versions of the formulary are no longer in effect. You can view the most current drug list by going to our website at http://www.lacare.org/members/getting-care/pharmacy-services For more details on available health care services, visit our website: http://www.lacare.org/members/welcome-la-care/member-documents/medi-cal LA1308E 02/20 EN lacare.org Last Updated: 07/01/2021 INTRODUCTION Foreword Te L.A. Care Health Plan (L.A. Care) Medi-Cal Dual formulary is a preferred list of covered drugs, approved by the L.A. Care Health Plan Pharmacy Quality Oversight Committee. Tis formulary applies only to outpatient drugs and self-administered drugs not covered by your Medicare Prescription Drug Beneft. It does not apply to medications used in the inpatient setting or medical ofces. Te formulary is a continually reviewed and revised list of preferred drugs based on safety, clinical efcacy, and cost-efectiveness. Te formulary is updated on a monthly basis and is efective the frst of every month. Tese updates may include, and are not limited to, the following: (i) removal of drugs and/or dosage forms, (ii) changes in tier placement of a drug that results in an increase in cost sharing, and (iii) any changes of utilization management restrictions, including any additions of these restrictions. Updated documents are available online at: lacare.org/members/getting-care/pharmacy-services. If you have questions about your pharmacy coverage, call Customer Solutions Center at 1-888-839-9909 (TTY 711), available 24 hours a day, 7 days a week. -
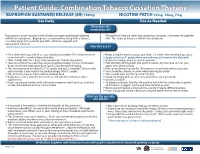
Bupropion + Patch
Patient Guide: Combination Tobacco Cessation Therapy BUPROPION SUSTAINED RELEASE (SR) 150mg NICOTINE PATCH 21mg, 14mg, 7mg Use Daily Use As Needed What does this medication do? Bupropion is a non-nicotine aid that helps you quit smoking by reducing The patch will release small, but continuous amounts of nicotine through the withdrawal symptoms. Bupropion is recommended along with a tobacco skin. This helps to decrease withdrawal symptoms. cessation program to provide you with additional support and educational materials. How do I use it? BUPROPION SUSTAINED RELEASE (SR) 150mg NICOTINE PATCH 21mg, 14mg, 7mg Set a date when you intend to stop smoking (quit date). The medicine needs Begin using the patch on your quit date, 1-2 weeks after starting bupropion. to be started 1-2 weeks before that date. Apply only one (1) patch when you wake up and remove the old patch. Take 1 tablet daily for 3 days, then increase to 1 tablet twice daily. If you miss a dose, use it as soon as you can. Take at a similar time each day, allowing approximately 8 hours in between Peel the back off the patch and put it on clean, dry, hair-free skin on your doses. Don’t take bupropion past 5pm to avoid trouble sleeping. upper arm, chest or back. This medicine may be taken for 7-12 weeks and up to 6 months. Discuss with Press patch firmly in place for 10 seconds so it will stick well to your skin. your provider if you need to be treated longer than 12 weeks. -

Transdermal Nicotine Maintenance Attenuates the Subjective And
Neuropsychopharmacology (2004) 29, 991–1003 & 2004 Nature Publishing Group All rights reserved 0893-133X/04 $25.00 www.neuropsychopharmacology.org Transdermal Nicotine Maintenance Attenuates the Subjective and Reinforcing Effects of Intravenous Nicotine, but not Cocaine or Caffeine, in Cigarette-Smoking Stimulant Abusers 1 1 ,1,2 Bai-Fang X Sobel , Stacey C Sigmon and Roland R Griffiths* 1Department of Psychiatry and Behavioral Science, Johns Hopkins University School of Medicine, Baltimore, MD, USA; 2Department of Neuroscience, Johns Hopkins University School of Medicine, Baltimore, MD, USA The effects of transdermal nicotine maintenance on the subjective, reinforcing, and cardiovascular effects of intravenously administered cocaine, caffeine, and nicotine were examined using double-blind procedures in nine volunteers with histories of using tobacco, caffeine, and cocaine. Each participant was exposed to two chronic drug maintenance phases (21 mg/day nicotine transdermal patch and placebo transdermal patch). Within each drug phase, the participant received intravenous injections of placebo, cocaine (15 and 30 mg/70 kg), caffeine (200 and 400 mg/70 kg), and nicotine (1.0 and 2.0 mg/70 kg) in mixed order across days. Subjective and cardiovascular data were collected before and repeatedly after drug or placebo injection. Reinforcing effects were also assessed after each injection with a Drug vs Money Multiple-Choice Form. Intravenous cocaine produced robust dose-related increases in subjective and reinforcing effects; these effects were not altered by nicotine maintenance. Intravenous caffeine produced elevations on several subjective ratings; nicotine maintenance did not affect these ratings. Under the placebo maintenance condition, intravenous nicotine produced robust dose-related subjective effects, with maximal increases similar to the high dose of cocaine; nicotine maintenance significantly decreased the subjective and reinforcing effects of intravenous nicotine. -
Submission of Plans for Cigarette Packages and Cigarette Advertisements (Revised)*
Contains Nonbinding Recommendations Submission of Plans for Cigarette Packages and Cigarette Advertisements (Revised)* Guidance for Industry Comments may be submitted at any time for Agency consideration. Electronic comments may be submitted to https://www.regulations.gov. Alternatively, submit written comments to the Dockets Management Staff (HFA-305), Food and Drug Administration, 5630 Fishers Lane, Room 1061, Rockville, MD, 20852. All comments should be identified with the docket number listed in the notice of availability that publishes in the Federal Register. For questions regarding this guidance, contact the Center for Tobacco Products at (Tel) 1-877- CTP-1373 (1-877-287-1373) Monday-Friday, 9 a.m. – 4 p.m. EDT. Additional copies are available online at https://www.fda.gov/tobacco-products/products- guidance-regulations/rules-regulations-and-guidance. You may send an e-mail request to [email protected] to receive an electronic copy of this guidance. You may send a request for hard copies to U.S. Food and Drug Administration, Center for Tobacco Products, Attn: Office of Small Business Assistance, Document Control Center, Bldg. 71, Rm. G335, 10903 New Hampshire Ave., Silver Spring, MD 20993-0002. U.S. Department of Health and Human Services Food and Drug Administration Center for Tobacco Products July 2021 OMB Control Number: 0910-0877 Expiration Date: 4/30/2023 See additional PRA statement in Section IV of the guidance *This is a revision to the third edition of this final guidance, which issued in February 2021. A summary of the revisions is at the end of the guidance. Contains Nonbinding Recommendations Table of Contents I. -

Smoking Cessation in People with Alcohol and Other Drug Problems
CLINICAL Smoking cessation in people with alcohol and other drug problems Colin P Mendelsohn, Alex Wodak AM Background eople who are dependent on alcohol Prevalence and other drugs have very high In 2007, 73% of people in Australia with People who consume alcohol and other P smoking rates and are far more drug-use disorders and 61% of those with drugs are at particularly high risk of likely to die from a smoking-related illness alcohol dependence smoked, compared harm from smoking, yet tobacco use is than from their primary drug problem.1,2 with 22% of the population overall.7 commonly neglected in this patient group. Smoking cessation in this at-risk group The smoking rate in people who are dependent on alcohol and other drugs Objectives is often rated as a lower priority and frequently delayed or ignored.3–5 has remained high in recent decades, The objectives of this article are to People with risky use of alcohol and while declining appreciably in the general 8 increase awareness of the high risk of other drugs frequently present with a community. tobacco-related harm in people who crisis that is usually given precedence Several explanations have been consume alcohol and other drugs, identify over smoking. In addition, there are proposed for this high-sustained smoking 9,10 the barriers to quitting and provide many misconceptions about smoking rate. There is a shared genetic practical guidelines to assist quitting. cessation in this population that predisposition to nicotine and other undermine intervention. For example, drugs of dependence. Nicotine and other Discussion addictive drugs trigger the release of health professionals often think that dopamine in the reward pathway, which People who are dependent on alcohol people who are dependent on alcohol creates pleasure, and co-administration and other drugs are far more likely and other drugs are unmotivated or has an additive effect that enhances to die from a smoking-related illness unable to quit smoking.5 In addition, enjoyment.