Gait Disorders
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Myopathy Associated with Pigmentary Degene- Ration
MYOPATHY ASSOCIATED WITH PIGMENTARY DEGENE RATION OF THE RETINA AND HIGH PROTEIN CONTENT OF CEREBROSPINAL FLUID JOSÉ ANTONIO LEVY*; MlLBERTO SCAFF*; ANA MARIA C. TSANACLIS**; VANDERLEI GARCIA RODRIGUES**; EDGARD SILVA LUSVARGHI** Harenko and Lapallainen4 (1962) reported a case of chronic progressive ophtalmoplegia with pigmentary degeneration of the retina, also referring 5 similar reports. Assis1 (1967) published the case of a 16-year-old female patient with progressive ophthalmoplegia, which began with palpebral ptosis and pigmentary degeneration of the retina, spreading to the macular regions; biopsy of the left superior rectus muscle showed a dystrophic process, i.e., a myopathy. Olson6 reported 7 cases of progressive ophthalmoplegia (patients' ages varied between 11 and 47 years, the period of time from the onset of the disease varying between 3 and 12 years) in which the biopsy of clinically normal limb muscles showed alterations confirming the existence of a myo pathy. A biopsy revealing myopathy and the external ophtalmoplegia were common in all these patients. Three of them displayed pigmentary retinosis; three had a slight motor deficit in the limb girdle muscles; four had electro- encephalographic abnormalities; in 5 of the cases which underwent a cerebro spinal fluid examination, a high protein content was encountered; in four cases the muscle biopsy showed alterations which suggested a lesion of the peripheral motor nerve; none of the cases suggested progressive muscular dystrophy with serious motor deficit in the limb girdle muscles. Kearn, quoted by Engel2, reported the case of a myopathic patient with external ophtalmo plegia associated with cardiomyopathy and pigmentary degeneration of the retina. -

A Syndrome-Based Clinical Approach for Clerkship Students General Comments 1. This Is Not an All-Inclusive “Cookbook” for Ev
A Syndrome-Based Clinical Approach for Clerkship Students General Comments 1. This is not an all-inclusive “cookbook” for every Neurology patient, but a set of guidelines to help you rationally approach patients with certain syndromes (sets of signs and symptoms which suggest a lesion in particular parts of the nervous system). 2. As you obtain a history and perform a neurological physical exam, try initially to localize all the patient’s signs and symptoms to one, single lesion in the nervous system. It may be surprising that a variety of signs and symptoms, at first glance apparently unrelated, on second thought can localize accurately to a single lesion. If this approach fails, then consider multiple, separate lesions for the patient’s signs and symptoms. 3. The tempo or rate at which signs and symptoms develop or occur often suggests the underlying pathological process. a. sudden onset---favors stroke (ischemia or hemorrhage), seizure, migraine (or other headache syndromes), and trauma b. subacute onset---favors inflammatory, infectious or immune-mediated disorders c. chronic onset---favors degenerative disorders, tumors Toximetabolic disorders, potentially treatable and reversible, may mimic lesions in the nervous system, and can evolve at variable tempos. Hereditary conditions may be congenital (present at birth) and nonprogressive or static, or develop later in life, with variable rates of progression. Family members affected by the same genetic disorder may be remarkably similar with regards to onset and clinical severity, while some genetic disorders vary widely regarding when and how severely family members are affected. 4. In the central nervous system, “positive symptoms or phenomena,” such as flashes of light, or a tingling sensation, suggest “excitation” or increased activity in the nervous system: migraine or seizure. -

Inherited Neuropathies
407 Inherited Neuropathies Vera Fridman, MD1 M. M. Reilly, MD, FRCP, FRCPI2 1 Department of Neurology, Neuromuscular Diagnostic Center, Address for correspondence Vera Fridman, MD, Neuromuscular Massachusetts General Hospital, Boston, Massachusetts Diagnostic Center, Massachusetts General Hospital, Boston, 2 MRC Centre for Neuromuscular Diseases, UCL Institute of Neurology Massachusetts, 165 Cambridge St. Boston, MA 02114 and The National Hospital for Neurology and Neurosurgery, Queen (e-mail: [email protected]). Square, London, United Kingdom Semin Neurol 2015;35:407–423. Abstract Hereditary neuropathies (HNs) are among the most common inherited neurologic Keywords disorders and are diverse both clinically and genetically. Recent genetic advances have ► hereditary contributed to a rapid expansion of identifiable causes of HN and have broadened the neuropathy phenotypic spectrum associated with many of the causative mutations. The underlying ► Charcot-Marie-Tooth molecular pathways of disease have also been better delineated, leading to the promise disease for potential treatments. This chapter reviews the clinical and biological aspects of the ► hereditary sensory common causes of HN and addresses the challenges of approaching the diagnostic and motor workup of these conditions in a rapidly evolving genetic landscape. neuropathy ► hereditary sensory and autonomic neuropathy Hereditary neuropathies (HN) are among the most common Select forms of HN also involve cranial nerves and respiratory inherited neurologic diseases, with a prevalence of 1 in 2,500 function. Nevertheless, in the majority of patients with HN individuals.1,2 They encompass a clinically heterogeneous set there is no shortening of life expectancy. of disorders and vary greatly in severity, spanning a spectrum Historically, hereditary neuropathies have been classified from mildly symptomatic forms to those resulting in severe based on the primary site of nerve pathology (myelin vs. -

THE NEUROLOGY Exam & Clinical Pearls
THE NEUROLOGY Exam & Clinical Pearls Gaye McCafferty, RN, MS, NP-BC, MSCS, SCRN NPANYS-SPHP Education Day Troy, New York April 7, 2018 Objectives I. Describe the core elements of the neurology exam II. List clinical pearls of the neuro exam Neurology Exam . General Physical Exam . Mental Status . Cranial Nerves . Motor Exam . Reflex Examination . Sensory Exam . Coordination . Gait and Station 1 General Systemic Physical Exam Head Trauma Dysmorphism Neck Tone Thyromegaly Bruits MSOffice1 General Systemic Physical Exam .Cardiovascular . Heart rate, rhythm, murmur; peripheral pulses, JVD .Pulmonary . Breathing pattern, cyanosis, Mallampati airway .General Appearance Hygiene, grooming, weight (signs of self neglect) .Funduscopic Exam Mental Status Level of Consciousness . Awake . Drowsy . Somnolent . Comatose 2 Slide 5 MSOffice1 , 6/14/2009 Orientation & Attention . Orientation . Time . Place . Person Orientation & Attention . Attention . Digit Span-have the patient repeat a series of numbers, start with 3 or 4 in a series and increase until the patient makes several mistakes. Then explain that you want the numbers backwards. Normal-seven forward, five backward Hint; use parts of telephone numbers you know Memory Immediate recall and attention Tell the patient you want him to remember a name and address – Jim Green – 20 Woodlawn Road, Chicago Note how many errors are made in repeating it and how many times you have to repeat it before it is repeated correctly. Normal: Immediate registration 3 Memory . Short-term memory . About 5 minutes after asking the patient to remember the name and address, ask him to repeat it. Long –term memory . Test factual knowledge . Dates of WWII . Name a president who was shot dead Memory Mini-Mental State Exam – 30 items Mini-Cog – Rapid Screen for Cognitive Impairment – A Composite of 3 item recall and clock drawing – Takes about 5 minutes to administer Mini-Cog Mini-Cog Recall 0 Recall 1-2 Recall 3 Demented Non-demented Abnormal Clock Normal Clock Demented Non-demented 4 Memory . -

EM Guidemap - Myopathy and Myoglobulinuria
myopathy EM guidemap - Myopathy and myoglobulinuria Click on any of the headings or subheadings to rapidly navigate to the relevant section of the guidemap Introduction General principles ● endocrine myopathy ● toxic myopathy ● periodic paralyses ● myoglobinuria Introduction - this short guidemap supplements the neuromuscular weakness guidemap and offers the reader supplementary information on myopathies, and a short section on myoglobulinuria - this guidemap only consists of a few brief checklists of "causes of the different types of myopathy" that an emergency physician may encounter in clinical practice when dealing with a patient with acute/subacute muscular weakness General principles - a myopathy is suggested when generalized muscle weakness involves large proximal muscle groups, especially around the shoulder and proximal girdle, and when the diffuse muscle weakness is associated with normal tendon reflexes and no sensory findings - a simple classification of myopathy:- Hereditary ● muscular dystrophies ● congenital myopathies http://www.homestead.com/emguidemaps/files/myopathy.html (1 of 13)8/20/2004 5:14:27 PM myopathy ● myotonias ● channelopathies (periodic paralysis syndromes) ● metabolic myopathies ● mitochondrial myopathies Acquired ● inflammatory myopathy ● endocrine myopathies ● drug-induced/toxic myopathies ● myopathy associated with systemic illness - a myopathy can present with fixed weakness (muscular dystrophy, inflammatory myopathy) or episodic weakness (periodic paralysis due to a channelopathy, metabolic myopathy -
Study & Evaluation Scheme Of
Study & Evaluation Scheme Of Bachelor of Physiotherapy [Applicable w.e.f. Academic Session 2013-14 till revised] [with revision approved by AC/EC meeting date September 21, 2013] TEERTHANKER MAHAVEER UNIVERSITY N.H.-24, Delhi Road, Moradabad, Uttar Pradesh-244001 Website: www.tmu.ac.in BPT Revised Syllabus Applicable w.e.f. Academic Session 2013-14 [21092013] Page 1 TEERTHANKER MAHAVEER UNIVERSITY (Established under Govt. of U. P. Act No. 30, 2008) Delhi Road, Bagarpur, Moradabad (U.P) Study & Evaluation Scheme of Bachelor of Physiotherapy SUMMARY Programme : Bachelor of Physiotherapy (BPT) Four years full time and six months internship (Annual Duration : System) Medium : English Minimum Required Attendance : 75 % (Theory) 80 % (Lab) Maximum Credits : 104 Minimum credits required for the degree : 104 Internal External Total Assessment (Theory) : 30 70 100 Class Class Class Assignment(s) Other Total Test Test Test Activity I II III (including Internal Evaluation (Theory Best two out of the attendance Papers) three 10 10 10 5 5 30 Internal External Total Evaluation Lab/Dissertations & Project 50 50 100 : Reports External Internal Duration of Examination : 3 hrs. 1 ½ hr. To qualify the course a student is required to secure a minimum of 50% marks in each subject including the year-end examination and teacher’s continuous evaluation (i.e. both internal and external). A candidate, who secures less than 50% marks in the year end examination, shall be deemed to have failed in that subject/course(s). To be eligible for the next year-end examination, a candidate must not have failed in more than two papers. Failure to fulfil this requirement will cause the student either to revert back to corresponding junior batch of students and continue his/her studies with them for rest of the program or clear the backlog as an external/ reappear candidate. -
2020 Measure Value Set Colorectal Cancer Screening
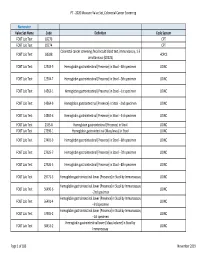
PT ‐ 2020 Measure Value Set_Colorectal Cancer Screening Numerator Value Set Name Code Definition Code System FOBT Lab Test 82270 CPT FOBT Lab Test 82274 CPT Colorectal cancer screening; fecal occult blood test, immunoassay, 1‐3 FOBT Lab Test G0328 HCPCS simultaneous (G0328) FOBT Lab Test 12503‐9 Hemoglobin.gastrointestinal [Presence] in Stool ‐‐4th specimen LOINC FOBT Lab Test 12504‐7 Hemoglobin.gastrointestinal [Presence] in Stool ‐‐5th specimen LOINC FOBT Lab Test 14563‐1 Hemoglobin.gastrointestinal [Presence] in Stool ‐‐1st specimen LOINC FOBT Lab Test 14564‐9 Hemoglobin.gastrointestinal [Presence] in Stool ‐‐2nd specimen LOINC FOBT Lab Test 14565‐6 Hemoglobin.gastrointestinal [Presence] in Stool ‐‐3rd specimen LOINC FOBT Lab Test 2335‐8 Hemoglobin.gastrointestinal [Presence] in Stool LOINC FOBT Lab Test 27396‐1 Hemoglobin.gastrointestinal [Mass/mass] in Stool LOINC FOBT Lab Test 27401‐9 Hemoglobin.gastrointestinal [Presence] in Stool ‐‐6th specimen LOINC FOBT Lab Test 27925‐7 Hemoglobin.gastrointestinal [Presence] in Stool ‐‐7th specimen LOINC FOBT Lab Test 27926‐5 Hemoglobin.gastrointestinal [Presence] in Stool ‐‐8th specimen LOINC FOBT Lab Test 29771‐3 Hemoglobin.gastrointestinal.lower [Presence] in Stool by Immunoassay LOINC Hemoglobin.gastrointestinal.lower [Presence] in Stool by Immunoassay FOBT Lab Test 56490‐6 LOINC ‐‐2nd specimen Hemoglobin.gastrointestinal.lower [Presence] in Stool by Immunoassay FOBT Lab Test 56491‐4 LOINC ‐‐3rd specimen Hemoglobin.gastrointestinal.lower [Presence] in Stool by Immunoassay FOBT Lab Test 57905‐2 -

9781441967237.Pdf
The Neurologic Diagnosis wwwwwwwwww Jack N. Alpert The Neurologic Diagnosis A Practical Bedside Approach Jack N. Alpert, MD St. Luke’s Episcopal Hospital Department of Neurology University of Texas Medical School at Houston Houston, TX, USA [email protected] ISBN 978-1-4419-6723-7 e-ISBN 978-1-4419-6724-4 DOI 10.1007/978-1-4419-6724-4 Springer New York Dordrecht Heidelberg London Library of Congress Control Number: 2011941214 © Springer Science+Business Media, LLC 2012 All rights reserved. This work may not be translated or copied in whole or in part without the written permission of the publisher (Springer Science+Business Media, LLC, 233 Spring Street, New York, NY 10013, USA), except for brief excerpts in connection with reviews or scholarly analysis. Use in connection with any form of information storage and retrieval, electronic adaptation, computer software, or by similar or dissimilar methodology now known or hereafter developed is forbidden. The use in this publication of trade names, trademarks, service marks, and similar terms, even if they are not identifi ed as such, is not to be taken as an expression of opinion as to whether or not they are subject to proprietary rights. While the advice and information in this book are believed to be true and accurate at the date of going to press, neither the authors nor the editors nor the publisher can accept any legal responsibility for any errors or omissions that may be made. The publisher makes no warranty, express or implied, with respect to the material contained herein. Printed on acid-free paper Springer is part of Springer Science+Business Media (www.springer.com) In Memory of Morris B. -

Physical Therapy Practice
Physical Therapy Practice THE MAGAZINE OF THE ORTHOPAEDIC SECTION, APTA VOL. 18, NO. 2 2006 ORTHOPAEDIC CARDON REHABILITATION PRODUCTS, INC.™ Wurlitzer Industrial Park, 908 Niagara Falls Blvd. North Tonawanda, NY 14120 Telephone: 1-800-944-7868 • Fax: 716-297-0411 E-mail: [email protected] THE ACCEPTED STANDARD OF PERFORMANCE The Cardon Mobilization Table . Going beyond the third dimension . Now available with the patented option which eliminates the use of flexion and rotation levers. This allows the therapist to perform advanced manual therapy techniques with complete confidence and comfort with an ergonomically friendly design. The unique design provides more efficient and smooth setup while providing superior patient comfort. The option enhances patient care by allowing unsurpassed opportunity for more preciseness of treatment and monitoring of segments and joints. he design and concepts make this “T the best mobilization table manufactured today.” Professor Freddy Kaltenborn Autho, Int’l Lecturer in Manual Therapy he various sections have minimum flex “T allowing very accurate application of specific manual therapy techniques.” Olaf Evjenth ES! I would like to preview the Author, Int’l Lecturer in Manual Therapy Y Cardon Mobilization Table. Please rush your 15 minute VHS video (for standard model): SEE FOR Name: Title: YOURSELF Clinic/Institution: THESE Address: OUTSTANDING City: State: Zip Code: Telephone: Signature: FEATURES: CARDON REHABILITATION PRODUCTS, INC.™ • Accurate localization of the vertebral segment Wurlitzer Industrial Park, 908 Niagara Falls Blvd. • Precision and versatility of technique North Tonawanda, NY 14120 • Absolute control of the mobilization forces Telephone: 1-800-944-7868 • Fax: 716-297-0411 • Excellent stability for manipulation. E-mail: [email protected] Orthopaedic Practice Vol. -

Neurological History and Physical Examination
emedicine.medscape.com eMedicine Specialties > Clinical Procedures > none Neurological History and Physical Examination Kalarickal J Oommen, MD, FAAN, Professor and Crofoot Chair of Epilepsy, Department of Neurology, Chief, Section of Epilepsy, Texas Tech University Health Sciences Center; Medical Director, Texas Tech University Health Sciences Center (TTUHSC) Covenant Comprehensive Epilepsy Center Updated: Nov 25, 2009 Neurological History "From the brain and the brain only arise our pleasures, joys, laughter and jests, as well as our sorrows, pains, griefs, and tears.... These things we suffer all come from the brain, when it is not healthy, but becomes abnormally hot, cold, moist or dry." —Hippocrates The Sacred Disease, Section XVII Taking the patient's history is traditionally the first step in virtually every clinical encounter. A thorough neurologic history allows the clinician to define the patient's problem and, along with the result of physical examination, assists in formulating an etiologic and/or pathologic diagnosis in most cases.[1 ] Solid knowledge of the basic principles of the various disease processes is essential for obtaining a good history. As Goethe stated, "The eyes see what the mind knows." To this end, the reader is referred to the literature about the natural history of diseases. The purpose of this article is to highlight the process of the examination rather than to provide details about the clinical and pathologic features of specific diseases. The history of the presenting illness or chief complaint should -
Movement Disorders and Gait Disturbances
Movement disorders and gait disturbances Kovács Norbert PTE ÁOK Neurológiai Klinika Pécs 1 MD pathophysiology z Genetic mutation or environmental injury of basal ganglia functioning z Pallidum, thalamus, subthalamic nucleus, caudate nucleus, pedunculopintine nucleus 2 Vitek JL. Mov Disord 2002;17(Supp 3):S49-62 Phenomenology in MD Hyperkinetic Isokinetic Hypokinetic • Tremor (regular) • Ataxia • Rigidity • Chorea • Bradykinesia • Ballism • Hypokinesia • Dystonia • Athetosis • Myoclonus (jerky) • Tic (jerky) 3 Hyperkinetic movements 4 Tremor classification More or less regular, sinusoid movements Any body parts can be affected (e.g. limbs, neck, trunc, vocal cords) Classification: • Intensity (invisible, barely visible, moderate, severe) • Frequency (slow or fast) • Position – Rest tremor (e.g. Parkinsonism) – Postural tremor (e.g. hyperthyroidism) – Kinetic tremor (e.g. essential tremor) – Intention tremor (e.g. cerebellar tremor) 5 Rest tremor Cognition (e.g. counting), gait or talking about the disease 6 usually increases the amplitude Intention tremor The tremor amplitude is the highest at the target. Usually 7 caused by cerebellar problems. Postural –kinetic tremor 8 Postural –kinetic tremor 9 Essential tremor is the most frequent cause of kinetic tremor. Postural –kinetic tremor 10 Always examine water drinking, writing and tableware use -- QoL Deep brain stimulation for tremor 11 Chorea The word chorea denotes rapid irregular muscle jerks that occur involuntarily and unpredictably in different parts of the body. Most important cause is12 Parkinson’s disease Ballism Large involuntary movements involving the whole extremity. Usually accompanies the chorea. Vascular lesion e.g. in the area of subthalamic13 nucleus can produce Athetosis abnormal movements that are slow, sinuous, and writhing in character. 14 Dystonia • Not a disease, it is a syndrome • Involuntary phasic, movement and/or • Sustained, involuntary, abnormal muscle contractions. -
GAIT DISORDERS, FALLS, IMMOBILITY Mov7 (1)
GAIT DISORDERS, FALLS, IMMOBILITY Mov7 (1) Gait Disorders, Falls, Immobility Last updated: April 17, 2019 GAIT DISORDERS ..................................................................................................................................... 1 CLINICAL FEATURES .............................................................................................................................. 1 CLINICO-ANATOMICAL SYNDROMES .............................................................................................. 1 CLINICO-PHYSIOLOGICAL SYNDROMES ......................................................................................... 1 Dyssynergy Syndromes .................................................................................................................... 1 Frontal gait ............................................................................................................................ 2 Sensory Gait Syndromes .................................................................................................................. 2 Sensory ataxia ........................................................................................................................ 2 Vestibular ataxia .................................................................................................................... 2 Visual ataxia .......................................................................................................................... 2 Multisensory disequilibrium .................................................................................................