Ocular Allergies
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Comparison of Intramuscular Betamethasone and Oral
Color profile: Disabled Composite Default screen 100 ORIGINAL ARTICLE 100 95 95 75 75 25 25 5 5 0 Comparison of intramuscular 0 betamethasone and oral prednisone in the prevention of relapse of acute asthma John S Chan MD1, Robert L Cowie MD1, Gerald C Lazarenko MD2, Cinde Little RRT1, Sandra Scott RRT1, Gordon T Ford MD FCCP1 1Division of Respiratory Medicine and 2Department of Emergency Medicine, University of Calgary, Calgary, Alberta JS Chan, RL Cowie, GC Lazarenko, C Little, S Scott, tively) and use of inhaled corticosteroids (46% versus 64.3% GT Ford. Comparison of intramuscular betamethasone respectively) (P<0.05). Using intention-to-treat analysis, the and oral prednisone in the prevention of relapse of acute relapse rates for betamethasone and prednisone at day 7 were asthma. Can Respir J 2001;8(3):147-152. 14.9% (13 of 87 patients) and 25% (21 of 84 patients), respectively (P=0.1), and at day 21, the rates were 36.8% (32 OBJECTIVE: To compare the relapse rate after a single intra- of 87 patients) and 31% (26 of 84 patients), respectively muscular injection of a long acting corticosteroid, betametha- (P=0.4). There were no differences in symptom score, peak sone, with oral prednisone in patients discharged from the flows and adverse effects between the two groups at days 7 emergency department (ED) for acute exacerbations of and 21. asthma. CONCLUSIONS: A single dose of intramuscular betametha- PATIENTS AND METHODS: Patients with acute exacer- sone 12 mg was safe and as efficacious as prednisone in pre- bations of asthma who were suitable for discharge from the venting the relapse of acute asthma. -

3364-136-03-01 Preparation and Administration of Medications Used in Respiratory Care Page 2
Name of Policy: Preparation and Administration of Medications Used in Respiratory Care Policy Number: 3364-136-03-01 Department: Respiratory Care Approving Officer: Associate VP Patient Care Services / CNO Responsible Agent: Director, Respiratory Care Scope: Effective Date: 6/1/2020 The University of Toledo Medical Center Initial Effective Date: 5/7/1989 Respiratory Care Department New policy proposal X Minor/technical revision of existing policy Major revision of existing policy Reaffirmation of existing policy (A) Policy Statement Medications administered by persons in the Respiratory Care Department will be in accordance with the physician's order as described in Hospital Policy # 3364-100-70-10 “Medication Management”, Pharmacy policies #3364-133-28 “Use of single and multi-dose Vials”, and # 3364-133-70 “Standard Medication Administration Times”. Medications for Respiratory Care administration must be approved by the Medical Director of Respiratory Care. Approved drugs are listed in attached Appendix A for 3364-136-03-01. (B) Purpose of Policy To insure safe preparation and administration of medications used by the practitioners of the Respiratory Care Department. (C) Procedure I. Procedure for Preparing Medications for Patient Use: Unit dose: . Unit dose medications will be used when available in ordered doses. Medications removed from the AcuDose Medication System and not administered must be returned to the AcuDose using the return medication procedure. Persons administering medications for respiratory care purposes will be knowledgeable about the drug being administered, regarding its purpose, indication, contraindication, and side affects. II. Medication Errors: The on-line SafetyNet system must be used for occurrences if: . A medication is missed. -

Long-Term Budesonide Or Nedocromil Mineral Accretion Over a Period of Years
term inhaled corticosteroid (ICS) treatment on bone Long-term Budesonide or Nedocromil mineral accretion over a period of years. Treatment, Once Discontinued, Does Not Alter the Course of Mild to Moderate Asthma in STUDY POPULATION. Cohort follow-up study for a median Children and Adolescents of 7 years with 877 children 5 to 12 years of age who Strunk RC, Sternberg AL, Szefler SJ, et al. J Pediatr. had mild-to-moderate asthma and initially were ran- 2009;154(5):682–687 domly assigned in the Childhood Asthma Management Program. PURPOSE OF THE STUDY. To determine whether long-term, METHODS. Serial dual-energy x-ray absorptiometry scans continuous use of inhaled antiinflammatory medications of the lumbar spine to assess bone mineral density were affects asthma outcomes in children with mild-to-mod- performed for all patients. Annual bone mineral accre- erate asthma after use is discontinued. tion was calculated for 531 boys and 346 girls. STUDY POPULATION. A total of 941 children, 5 to 12 years of RESULTS. Oral corticosteroid bursts produced dose- age, who had previously participated in the Childhood dependent reductions in bone mineral accretion (0.052, Asthma Management Program (CAMP). 0.049, and 0.046 g/cm2 per year with 0, 1–4, and Ն5 courses, respectively) and increases in the risk for osteo- METHODS. During the CAMP trial, subjects received treat- penia (10%, 14%, and 21%, respectively) in boys but ment with budesonide, nedocromil, or placebo for 4.3 not girls. Cumulative ICS use was associated with a small years. During the posttrial period, asthma manage- decrease in bone mineral accretion in boys but not girls ment was provided by primary care physicians ac- but no increased risk for osteopenia. -

Or Should It Be Mast Cell Mediator Disorders?
HHS Public Access Author manuscript Author ManuscriptAuthor Manuscript Author Expert Rev Manuscript Author Clin Immunol Manuscript Author . Author manuscript; available in PMC 2020 February 06. Published in final edited form as: Expert Rev Clin Immunol. 2019 June ; 15(6): 639–656. doi:10.1080/1744666X.2019.1596800. Recent advances in our understanding of mast cell activation – or should it be mast cell mediator disorders? Theoharis C. Theoharidesa,b,c,d, Irene Tsilionia, Huali Rene aMolecular Immunopharmacology and Drug Discovery Laboratory, Department of Immunology, Tufts University School of Medicine, Boston, MA, USA bSackler School of Graduate Biomedical Sciences, Tufts University School of Medicine, Boston, MA, USA cDepartment of Internal Medicine, Tufts University School of Medicine and Tufts Medical Center, Boston, MA, USA dDepartment of Psychiatry, Tufts University School of Medicine and Tufts Medical Center, Boston, MA, USA eDepartment of Otolaryngology, Beijing Electric Power Hospital, Beijing, China Abstract Introduction: An increasing number of patients present with multiple symptoms affecting many organs including the brain due to multiple mediators released by mast cells. These unique tissue immune cells are critical for allergic reactions triggered by immunoglobulin E (IgE), but are also stimulated (not activated) by immune, drug, environmental, food, infectious, and stress triggers, leading to secretion of multiple mediators often without histamine and tryptase. The presentation, diagnosis, and management of the spectrum of mast cell disorders are very confusing. As a result, specialists have recently excluded neuropsychiatric symptoms, and made the diagnostic criteria stricter, at the expense of excluding most patients. Areas covered: A literature search was performed on papers published between January 1990 and November 2018 using MEDLINE. -

FDA Briefing Document Pulmonary-Allergy Drugs Advisory Committee Meeting
FDA Briefing Document Pulmonary-Allergy Drugs Advisory Committee Meeting August 31, 2020 sNDA 209482: fluticasone furoate/umeclidinium/vilanterol fixed dose combination to reduce all-cause mortality in patients with chronic obstructive pulmonary disease NDA209482/S-0008 PADAC Clinical and Statistical Briefing Document Fluticasone furoate/umeclidinium/vilanterol fixed dose combination for all-cause mortality DISCLAIMER STATEMENT The attached package contains background information prepared by the Food and Drug Administration (FDA) for the panel members of the advisory committee. The FDA background package often contains assessments and/or conclusions and recommendations written by individual FDA reviewers. Such conclusions and recommendations do not necessarily represent the final position of the individual reviewers, nor do they necessarily represent the final position of the Review Division or Office. We have brought the supplemental New Drug Application (sNDA) 209482, for fluticasone furoate/umeclidinium/vilanterol, as an inhaled fixed dose combination, for the reduction in all-cause mortality in patients with COPD, to this Advisory Committee in order to gain the Committee’s insights and opinions, and the background package may not include all issues relevant to the final regulatory recommendation and instead is intended to focus on issues identified by the Agency for discussion by the advisory committee. The FDA will not issue a final determination on the issues at hand until input from the advisory committee process has been considered -

Protective Effects of Inhaled Ipratropium Bromide on Bronchoconstriction Induced by Adenosine and Methacholine in Asthma
Eur Aesplr J 1992, 5, 56()-665 Protective effects of inhaled ipratropium bromide on bronchoconstriction induced by adenosine and methacholine In asthma N. Crimi, F. Palermo, R. Oliveri, R. Polosa, I. Settinieri, A. Mistretta Protective effects of inhaled ipratropium bromide on bronchoconstriction induced by Istituto di Malattie dell' Apparato adenosine and methacholine in asthma. N. Crimi, F. Palermo, R. Oliveri, R. Po/osa, Respiratorio e Tisiologia, Universita' di Catania, Catania, Italy. I. Seuinier~ A. Mistretta. ABSTRACT: Although adenosine-Induced bronchoconstrictlon is mainly due to Correspondence: N. Crimi mast cell mediator release, vagal reflexes have also been Implicated in this Istituto di Malattie dell' Appara.to response. Respiratorio e Tisiologia We have Investigated the effect of a speciflc muscarlnlc-receptor antagonist, Universita' di Catania ipratroplum bromide, on methacholine- and adenosine-Induced bronchoconstriction Via Passo Gravina 187 In a randomized, placebo-controlled, double-blind study of 12 asthmatic subjects. 95125 Catania Airway response was evaluated as forced expiratory volume in one second (FEV,). Italy Inhaled lpratroplum bromide (40 Jlg), administered 20 mln prior to bronchoprovocation, Increased the provocation dose of Inhaled methacholine and Keywords: Adenosine adenosine required to reduce FEV, by 20% from baseline (PD,.) from 0.11 to 0.79 asthma ipratropium bromide mg (p<O.Ol) and from 0.57 to 1.27 mg (p<0.01), respectively. The mean baseline methacholine FEV, values after administration of lpratroplum bromide were signlfkantly higher than after placebo administration (p<O.OS). However, there was no correlation Received: May 22 1991 between the degree of bronchodllatatlon and dose-ratios for methacholine and Accepted after revision January 7 1992 adenosine. -

Core Safety Profile
Core Safety Profile Active substance: Nedocromil Pharmaceutical form(s)/strength: Eye drops: 20 mg/ml, Inhalation vapour: 5 mg/ml, Pressurised inhalation: 2 mg/dose, 2mg/0,1 mg, Nebuliser solution: 10 mg/2 ml, Inhalation powder: 10 mg/dose, Nasal spray: 10 mg/ml P-RMS: CZ/H/PSUR/0016/001 Date of FAR: 09.10.2010 EU Core Safety Profile (CSP) For Nedocromil sodium NB: This CSP is combining safety information from the three existing pharmaceutical forms: Eye drops, Nasal spray and Inhaler. Information that is specific to one form is identified by a subheading. No subheading indicates that information is valid for all pharmaceuticals forms 4.3 Contraindications For eye drops <Product name> eye drops is contraindicated in patients with known hypersensitivity to nedocromil sodium, benzalkonium chloride or other constituents of the formulation. For Nasal spray and Inhaler <Product name> nasal spray or inhaler is contraindicated in patients with known hypersensitivity to any of the constituents. 4.4 Special warnings and precautions for use For eye drops Patients should be advised not to wear soft contact lenses during treatment with <product name> eye drops. Benzalkonium chloride, a constituent of the formulation, may accumulate in soft contact lenses. This preservative, when slowly released, could possibly irritate the cornea. In patients who continue to wear hard or gas permeable contact lenses during <product name> eye drops treatment, the lenses should be taken out of the eye prior to instillation of the drops. They should be inserted again not earlier than 10 minutes after administration, in order to allow an even conjunctival distribution of the solution. -

Drug Class Review Nasal Corticosteroids
Drug Class Review Nasal Corticosteroids Final Report Update 1 June 2008 The Agency for Healthcare Research and Quality has not yet seen or approved this report The purpose of this report is to make available information regarding the comparative effectiveness and safety profiles of different drugs within pharmaceutical classes. Reports are not usage guidelines, nor should they be read as an endorsement of, or recommendation for, any particular drug, use or approach. Oregon Health & Science University does not recommend or endorse any guideline or recommendation developed by users of these reports. Dana Selover, MD Tracy Dana, MLS Colleen Smith, PharmD Kim Peterson, MS Oregon Evidence-based Practice Center Oregon Health & Science University Mark Helfand, MD, MPH, Director Marian McDonagh, PharmD, Principal Investigator, Drug Effectiveness Review Project Copyright © 2008 by Oregon Health & Science University Portland, Oregon 97239. All rights reserved. Final Report Update 1 Drug Effectiveness Review Project TABLE OF CONTENTS INTRODUCTION ..........................................................................................................................5 Scope and Key Questions .......................................................................................................................7 METHODS ....................................................................................................................................9 Literature Search .....................................................................................................................................9 -
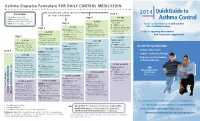
Asthma Control
Asthma Stepwise Formulary FOR DAILY CONTROL MEDICATION QuickGuide to abbreviations: step 6 2014 • ICS: inhaled corticosteroid step 5 • LABA: long-acting beta2-agonist Asthma Control HIGH-DOSE ICS • LTRA: leukotriene receptor antagonist (per step 5) • SABA: short-acting beta2-agonist step 4 LTRA (per step 4) for the care of pediatric and adult patients + LTRA (per step 4) + HIGH-DOSE ICS with established asthma step 3 (mark choice): + oral systemic steroids MEDIUM-DOSE ICS fluticasone (Flovent) MDI: (lowest dose for the shortest (per step 3; mark a choice there) 110 mcg: 2 puffs twice daily duration: 5-10 mg is A tool for ongoing assessment considered low-dose) MEDIUM-DOSE ICS + LTRA: montelukast budesonide (Pulmicort) respules: and treatment adjustment step 2 (mark choice): (Singulair) by mouth: 1.0 mg: 1 respule twice daily 4 mg: 1 tablet once daily, or fluticasone (Flovent) MDI: 1 packet oral granules once daily 110 mcg: 1 puff twice daily HIGH-DOSE ICS budesonide (Pulmicort) respules: (per step 5) LOW-DOSE ICS (mark choice): LABA (per step 3) 0.50 mg: 1 respule twice daily + LABA (per step 4) fluticasone (Flovent) MDI: + HIGH-DOSE ICS LABA (per step 3) Inside the QuickGuide... 44 mcg: 2 puffs twice daily (mark choice): + oral systemic steroids budesonide (Pulmicort) respules: + MEDIUM-DOSE ICS fluticasone (Flovent) MDI: (lowest dose for the shortest 0.25 mg: 1 respule twice daily (mark choice): • Asthma control tables step 1 110 mcg: 2 puffs twice daily duration: 5-10 mg is considered low-dose) fluticasone (Flovent) -

Chapter 10 Drugs for Treating Colds and Allergies Case Study It Seems
Chapter 10 Drugs for Treating Colds and Allergies Case Study It seems that the university’s wrestling team benefited from the exceptionally long break the coach gave them over the Christmas holidays because they all seem eager to continue the remaining part of the season in earnest. However, Sam, the team’s 74-kg class wrestler, appears uncomfortable and less energetic. He reports that over break he contracted an upper respiratory tract infection. Sam started taking an over-the-counter (OTC) medication to relieve his runny nose when he first felt the onset of the cold. He states that it seems to be helping, but he is feeling more tired since starting the medication. What is a possible explanation for Sam’s symptoms? Answer: The medication Sam is taking likely contains a first-generation antihistamine. These medications are found in several OTC cough, cold, and allergy products, both alone and in combination with other medications. They are helpful in colds because they decrease mucus production and have a drying effect, therefore relieving the symptom of runny nose. However, they also have a major adverse effect of causing drowsiness. This is likely the cause of Sam’s tiredness. The second-generation antihistamines are non-sedating; however, they also lack the drying effect of the first-generation antihistamines and therefore would not be as effective in treating Sam’s symptoms. Some of the first-generation antihistamines, such as chlorpheniramine, have less of a sedating effect, so switching products may help with the adverse effects. Exam Questions 1. All of the following intranasal corticosteroid products are available by prescription only except for: a. -

Comparison of Long-Term Clinical Implications of Beta-Blockade In
Comparison of long-term clinical implications of beta-blockade in patients with obstructive airway diseases exposed to beta-blockers with different 1-adrenoreceptor selectivity An Italian population-based cohort study Sessa, Maurizio; Mascolo, Annamaria; Scavone, Cristina; Perone, Ilaria; Giorgio, Annalisa Di; Tari, Michele; Fucile, Annamaria; De Angelis, Antonella; Rasmussen, Daniel Bech; Jensen, Magnus Thorsten; Kragholm, Kristian; Rossi, Francesco; Capuano, Annalisa; Sportiello, Liberata Published in: Frontiers in Pharmacology DOI: 10.3389/fphar.2018.01212 Publication date: 2018 Document version Publisher's PDF, also known as Version of record Citation for published version (APA): Sessa, M., Mascolo, A., Scavone, C., Perone, I., Giorgio, A. D., Tari, M., Fucile, A., De Angelis, A., Rasmussen, D. B., Jensen, M. T., Kragholm, K., Rossi, F., Capuano, A., & Sportiello, L. (2018). Comparison of long-term clinical implications of beta-blockade in patients with obstructive airway diseases exposed to beta-blockers with different 1-adrenoreceptor selectivity: An Italian population-based cohort study. Frontiers in Pharmacology, 9, 1- 8. [1212]. https://doi.org/10.3389/fphar.2018.01212 Download date: 26. Sep. 2021 fphar-09-01212 October 23, 2018 Time: 14:25 # 1 ORIGINAL RESEARCH published: 25 October 2018 doi: 10.3389/fphar.2018.01212 Comparison of Long-Term Clinical Implications of Beta-Blockade in Patients With Obstructive Airway Diseases Exposed to Beta-Blockers With Different b1-Adrenoreceptor Edited by: Lei Xi, Selectivity: An Italian -

Product Information Tilade Cfc-Free
PRODUCT INFORMATION TILADE CFC-FREE NAME OF THE MEDICINE nedocromil sodium DESCRIPTION Tilade CFC-Free contains nedocromil sodium as a suspension in a non-CFC propellant, 1,1,1,2,3,3,3-heptafluoropropane (HFA-227). Other excipients include povidone, macrogol 600 and menthol. CAS number: 69049-74-74 Nedocromil sodium (Disodium 9-ethyl-6,9-dihydro-4,6-dioxo-10-propyl-4H-pyrano-(3,2- g)quinoline-2,8-dicarboxylate). PHARMACOLOGY Nedocromil sodium inhibits the release of inflammatory mediators from a variety of cell types occurring in the lumen and in the mucosa of the bronchial tree. Laboratory experiments have shown that nedocromil sodium prevents the release of inflammatory chemotactic and smooth muscle contracting mediators which are preformed or derived from arachidonic acid metabolism by both the lipoxygenase and cyclo-oxygenase pathways in a range of human and animal leucocytes. In the Ascaris suum sensitised monkey subjected to bronchial challenge with specific antigen, nedocromil sodium provides protection against changes in airways resistance and lung compliance. Nedocromil sodium prevents the release of mediators such as histamine, LTC4 and PGD2 from the cellular population of the chronically inflamed bronchus. There is growing evidence that these mediators are important also in lung disease in man, and this additional activity may be expected to give nedocromil sodium extended scope in the management of bronchial asthma in which inflammation, allergy and bronchial hyper-responsiveness are significant physiological factors. Pharmacokinetics After inhalation, nedocromil sodium is deposited throughout the respiratory tract, from which about 5% of the dose is absorbed. By the nature of inhalation dosing, much of the delivered dose is swallowed directly or subsequently upon mucociliary clearance from the large airways.