Project Proposal
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Resident Coordinator Support Office, Upper Nile State Briefing Pack
Resident Coordinator Support Office, Upper Nile State Briefing Pack Table of Contents Page No. Table of Contents 1 State Map 2 Overview 3 Security and Political History 3 Major Conflicts 4 State Government Structure 6 Recovery and Development 7 State Resident Coordinator’s Support Office 8 Organizations Operating in the State 9-11 1 Map of Upper Nile State 2 Overview The state of Upper Nile has an area of 77,773 km2 and an estimated population of 964,353 (2009 population census). With Malakal as its capital, the state has 13 counties with Akoka being the most recent. Upper Nile shares borders with Southern Kordofan and Unity in the west, Ethiopia and Blue Nile in the east, Jonglei in the south, and White Nile in the north. The state has four main tribes: Shilluk (mainly in Panyikang, Fashoda and Manyo Counties), Dinka (dominant in Baliet, Akoka, Melut and Renk Counties), Jikany Nuer (in Nasir and Ulang Counties), Gajaak Nuer (in Longochuk and Maiwut), Berta (in Maban County), Burun (in Maban and Longochok Counties), Dajo in Longochuk County and Mabani in Maban County. Security and Political History Since inception of the 2005 Comprehensive Peace Agreement (CPA), Upper Nile State has witnessed a challenging security and political environment, due to the fact that it was the only state in Southern Sudan that had a Governor from the National Congress Party (NCP). (The CPA called for at least one state in Southern Sudan to be given to the NCP.) There were basically three reasons why Upper Nile was selected amongst all the 10 states to accommodate the NCP’s slot in the CPA arrangements. -

Upper Nile State SOUTH SUDAN
COMMUNITY CONSULTATION REPORT Upper Nile State SOUTH SUDAN Bureau for Community Security South Sudan Peace and Small Arms Control and Reconciliation Commission United Nations Development Programme Ministry of Foreign Affairs of the Netherlands The Bureau for Community Security and Small Arms Control under the Ministry of Interior is the Gov- ernment agency of South Sudan mandated to address the threats posed by the proliferation of small arms and community insecurity to peace and development. The South Sudan Peace and Reconciliation Commission is mandated to promote peaceful co-existence amongst the people of South Sudan and advises the Government on matters related to peace. The United Nations Development Programme in South Sudan, through the Community Security and Arms Control Project, supports the Bureau strengthen its capacity in the area of community security and arms control at the national, state and county levels. The consultation process was led by the Government of South Sudan, with support from the Govern- ment of the Netherlands’ Ministry of Foreign Affairs. Cover photo: A senior chief from Upper Nile. © UNDP/Sun-ra Lambert Baj COMMUNITY CONSULTATION REPORT Upper Nile State South Sudan Published by South Sudan Bureau for Community Security and Small Arms Control South Sudan Peace and Reconciliation Commission United Nations Development Programme MAY 2012 JUBA, SOUTH SUDAN CONTENTS Acronyms ........................................................................................................................... i Foreword .......................................................................................................................... -

The Conflict in Upper Nile State (18 March 2014 Update)
The Conflict in Upper Nile State (18 March 2014 update) Three months have elapsed since widespread conflict broke out in South Sudan, and Malakal, Upper Nile’s state capital, remains deserted and largely burned to the ground. The state is patchwork of zones of control, with the rebels holding the largely Nuer south (Longochuk, Maiwut, Nasir, and Ulang counties), and the government retaining the north (Renk), east (Maban and Melut), and the crucial areas around Upper Nile’s oil fields. The rest of the state is contested. The conflict in Upper Nile began as one between different factions within the SPLA but has now broadened to include the targeted ethnic killing of civilians by both sides. With the status of negotiations in Addis Ababa unclear, and the rebel’s 14 March decision to refuse a regional peacekeeping force, conflict in the state shows no sign of ending in the near future. With the first of the seasonal rains now beginning, humanitarian costs of ongoing conflict are likely to be substantial. Conflict began in Upper Nile on 24 December 2013, after a largely Nuer contingent of the Sudan People’s Liberation Army’s (SPLA) 7th division, under the command of General Gathoth Gatkuoth, declared their loyalty to former vice-president Riek Machar and clashed with government troops in Malakal. Fighting continued for three days. The central market was looted and shops set on fire. Clashes also occurred in Tunja (Panyikang county), Wanding (Nasir county), Ulang (Ulang county), and Kokpiet (Baliet county), as the SPLA’s 7th division fragmented, largely along ethnic lines, and clashed among themselves, and with armed civilians. -

South Sudan 2015 Human Rights Report
SOUTH SUDAN 2015 HUMAN RIGHTS REPORT EXECUTIVE SUMMARY South Sudan is a republic operating under a transitional constitution signed into law upon declaration of independence from Sudan in 2011. President Salva Kiir Mayardit, whose authority derives from his 2010 election as president of what was then the semiautonomous region of Southern Sudan within the Republic of Sudan, led the country. While the 2010 Sudan-wide elections did not wholly meet international standards, international observers believed Kiir’s election reflected the will of a large majority of Southern Sudanese. International observers considered the 2011 referendum on South Sudanese self-determination, in which 98 percent of voters chose to separate from Sudan, to be free and fair. President Kiir is a founding member of the Sudan People’s Liberation Movement (SPLM) political party, the political wing of the Sudan People’s Liberation Army (SPLA). Of the 27 ministries, only 21 had appointed ministers in charge, of which 19 are SPLM representatives. The bicameral legislature consists of 332 seats in the National Legislative Assembly (NLA), of which 296 were filled, and 50 seats in the Council of States. SPLM representatives controlled the vast majority of seats in the legislature. Through presidential decrees Kiir replaced eight of the 10 state governors elected since 2010. The constitution states that an election must be held within 60 days if an elected governor has been relieved by presidential decree. This has not happened. The legislature lacked independence, and the ruling party dominated it. Civilian authorities failed at times to maintain effective control over the security forces. In 2013 armed conflict between government and opposition forces began after violence erupted within the Presidential Guard Force (PG) of the SPLA, also known as the Tiger Division. -

Ulang Town, Nyangora, Barmach, Ulang County, Upper Nile State
IRNA Report: [Ulang Town, Nyangora, Barmach, Ulang County, Upper Nile State] [18-20 September 2014] This IRNA Report is a product of Inter-Agency Assessment mission conducted and information compiled based on the inputs provided by partners on the ground including; government authorities, affected communities/IDPs and agencies. Highlights: • Displacement was primarily within Ulang county and IDPs and host community are well integrated • In Ulang town people are primarily returning IDPs while in Nyangora and Barmach they are a mix of IDPs and host community • Preliminary numbers are 8,440 returning IDPs in Ulang town, 4,000 IDPs and 8,000 host community in Nyangora, and 6,300 IDPs and 7,600 host community in Barmach • Proxy malnutrition at very high rates, SAM 16.6%, MAM 28.4%, and GAM 45% Food distribution and re-establishment of health and nutrition services also high priorities • • NGOs planning response include GOAL (health and nutrition), ADRA (education), Nile Hope (protection), NP (protection), Medair (WASH), and Food For the Hungry with WFP (FSL) • As Ulang is on the Malakal – Nasir road, it is vulnerable to attack in the dry season. Contingencies to move operations to Nyangora (across the river in sight of Ulang town) must therefore be in place, or response should focus on Nyangora to begin with. Situation overview From 18-20 September a joint assessment team visited Ulang town, Nyangora, and Barmach in Ulang County, Upper Nile State, to assess reports of humanitarian need resulting from conflict-related displacement that occurred in the first half of 2014. On 18 and 20 September the team assessed Ulang town and on 19 September the team split and assessed Nyangora and Barmach, across the Sobat river from Ulang town. -
Jonglei Unity Upper Nile
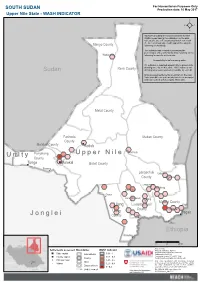
For Humanitarian Purposes Only SOUTH SUDAN Production date: 10 May 2017 Upper Nile State - WASH INDICATOR REACH calculated the areas more likely to have WASH needs basing the estimation on the data collected between February and March 2017 with the Area of Knowledge (AoK) approach, using the Manyo County following methodology. The indicator was created by averaging the percentages of key informants (KIs) reporting on the Wadakona following for specific settlements: - Accessibility to safe drinking water 0% indicates a reported impossibility to access safe Renk County drinking water by all KIs, while 100% indicates safe Sudan drinking water was reported accessible by each KI. Only assessed settlements are shown on the map. Values for different settlements have been averaged and represented with hexagons 10km wide. Melut County Fashoda Maban County County Malakal County Kodok Panyikang Guel Guk Ogod U p p e r N i l e U n i t y County Tonga Malakal Baliet County Pakang Longochuk Udier County Chotbora Longuchok Mathiang Kiech Kon Dome Gum (Kierwan) Mading Maiwut County Ulang Luakpiny/Nasir Kigili County Maiwut Ulang Pagak J o n g l e i County Jikmir Jikou Ethiopia Wanding Sudan 0 25 50 km Data sources: Ethiopia Settlements assessed Boundaries WASH indicator Thematic indicators: REACH Administrative boundaries: UNOCHA; State capital International 0.81 - 1 Settlements: UNOCHA; County capital 0.61 - 0.8 Coordinate System:GCS WGS 1984 C.A.R. County Contact: [email protected] Principal town 0.41 - 0.6 Note: Data, designations and boundaries contained Juba State Village 0.21 - 0.4 on this map are not warranted to be error-free and do not imply acceptance by the REACH partners, Disputed area associates, donors or any other stakeholder D.R.C. -

Sudan's North
Concordis International Sudan Report September 2010 MORE THAN A LINE: SUDAN’S NORTH - SOUTH BORDER SEPTEMBER 2010 02 Concordis International Sudan Report Contents Contents 04 Acknowledgements 50 Abyei 1.1 Snapshot Summary 1.2 Conflict Drivers 05 Glossary 1.2.1 National Political Context 1.2.2 Border Demarcation and the 08 Executive Summary Abyei Referendum 1.1 General Findings 1.2.3 Physical Demarcation 1.2 Thematic Findings 1.2.4 Land 1.3 Conflict Prone Areas 1.2.5 Militarisation 14 Introduction 1.3.6 Additional Factors 1.1 General Findings 1.4 Conflict Management 1.2 Thematic Findings 1.3 Conflict Prone Areas 67 Southern Kordofan/Unity 1.1 Snapshot Summary 28 South Darfur-Western Bahr al Ghazal 1.2 Conflict Drivers 1.1 Snapshot Summary 1.2.1 Transhumance 1.2 Conflict Drivers 1.2.2 Political Marginalisation 1.2.1 Border demarcation 1.2.3 Hardening Conflict Memory 1.2.2 Militarisation 1.2.4 Land/Oil and Demarcation 1.2.3 SPLA-Rezeigat Clashes 1.2.5 Community Land 1.2.4 Other Armed Groups 1.2.6 Militarisation 1.2.5 Wider Regional Instability 1.2.7 Community Conflict Management 1.2.6 Conflict Trends 1.3 Conflict Trends and Mitigation 1.3 Conflict Mitigation 79 Southern Kordofan 38 South Darfur-Northern Bahr al Ghazal 1.1 Snapshot Summary 1.1 Snapshot Summary 1.2 Conflict Drivers 1.2 Conflict Drivers 1.2.1 National Political Context 1.2.1 Contested Rights Along the 1.2.2 Land Grazing Area 1.2.3 Socio-economic Underdevelopment 1.2.2 Transportation of Arms 1.2.4 Integration of Adminstration 1.2.3 Militarisation 1.2.5 Security Integration and -

Fashoda Youth Forum Allocation Type
Requesting Organization : Fashoda Youth Forum Allocation Type : 1st Round Standard Allocation Primary Cluster Sub Cluster Percentage EDUCATION 100.00 100 Project Title : Lifesaving Education program for Upper Nile State Allocation Type Category : Frontline services OPS Details Project Code : SSD-16/E/88945 Fund Project Code : SSD-16/HSS10/SA1/E/NGO/695 Cluster : Education Project Budget in US$ : 119,995.15 Planned project duration : 6 months Priority: 1 Planned Start Date : 01/01/2016 Planned End Date : 30/06/2016 Actual Start Date: 01/01/2016 Actual End Date: 30/06/2016 Project Summary : The aim of this project is to provide life-saving education and youth-focused life skills vocational training for a total of 3,350 children, that is –1650 displaced children and 1700 host community children of both (girls and boys) and 125 adult (60 Teachers and 65 PTAs (men and women) in both Lul and Kodok Payams of Fashoda County. The project will provide training and services in life skills, PSS and child protection in schools, and also provide youth-focused PSS and Life Skills training for young people out of school in order to enroll them back into schools activities. TLS constructed earlier will be maintained to provide access to learning activities for the children school facilities will be rehabilitated also to provide child-friendly spaces which can continue to deliver lifesaving messages to the children. Sanitation facilities will be provided also to all the school facilities to prevent the spread of diseases and awareness on cholera will be raised thus promoting healthy and hygienic school environments. -

Malakal Combined Assessment I
February2018 Malakal Combined Assessment I. Town head-count — II. Malakal town services — III. PoC Site Survey p3 p4-11 p12-17 Malakal Town PoC Site 11,573 Individuals Identied Population: 24,417 Most common reason for p.14 displacement: conict p.4 7/27 villages deserted (26%) Recent inux from Fashoda 7 educational facilities; 68% of teaching because of conict p5-7 staff untrained or volunteers; unsafe buildings; lack of materials p.16 96% intend to remain or are unsure about the future p8-10 4 healthcare facilities in town employing 2 doctors. Urgent need for Improvement of security combined with human resources and electricity sources p.17 assurance from government on safety gure as the top pre-condition for return p11 6 water sources (bladder tanks) IOM’s Displacement Tracking Matrix (DTM) conducted a combined assessement comprising a Village Assessment Survey (VAS) in Malakal Town and a complementary survey in the PoC site from 16 to 26 February 2018 to meet information gaps identied by the inter cluster working group (ICWG). The VAS tool has been used in South Sudan since 2007 and serves to identify critical gaps in available services in areas of high or potentially high return. Findings are presented in sector-specic sections for easy reference. The survey conducted in Malakal’s Protection of Civilian (PoC) site complements VAS ndings by gauging the potential interest of the displaced population to return to the town to make use of the assessed services. Please note that the town’s current population is primarily composed of relocated households from a variety of origins. -

Secretary-General's Report on South Sudan
United Nations S/2020/145 Security Council Distr.: General 26 February 2020 Original: English Situation in South Sudan Report of the Secretary-General I. Introduction 1. The present report is submitted pursuant to Security Council resolution 2459 (2019), by which the Council extended the mandate of the United Nations Mission in South Sudan (UNMISS) until 15 March 2020 and requested me to report on the implementation of the Mission’s mandate every 90 days. It covers political and security developments between 1 December 2019 and 15 February 2020, the humanitarian and human rights situation and progress made in the implementation of the Mission’s mandate. II. Political and economic developments Key political updates 2. During the reporting period, the President of South Sudan, Salva Kiir, and the leader of the Sudan People’s Liberation Movement/Army in Opposition (SPLM/A-IO), Riek Machar, held several face-to-face meetings in Juba. The principals deliberated on outstanding pre-transitional tasks, including transitional security arrangements and the issue of states and their boundaries. Although the status of Mr. Machar remains unresolved, he travelled to Juba from 10 to 17 December and from 14 to 26 January, accompanied on both occasions by the Vice-President of the Sovereign Council of the Sudan, Lieutenant General Mohamed Hamdan Dagalo. 3. A key outstanding issue is the determination of the number of states and their boundaries. From 2 to 4 December, the Deputy President and Special Envoy of South Africa to South Sudan, David Mabuza – supported by the Special Envoys of the Intergovernmental Authority on Development (IGAD), Kenya, the Sudan and Uganda – convened deliberations on the matter, but was unable to get the parties to reach a consensus. -

South Sudan - Upper Nile State South Sudan Displacement Crisis Assessment of Hard-To-Reach Areas in South Sudan May 2017
South Sudan - Upper Nile State South Sudan Displacement Crisis Assessment of Hard-to-Reach Areas in South Sudan May 2017 Overview Assessment coverage In 2014 and 2015, Upper Nile State was the site of some data in hard-to-reach areas of Unity State. Juba PoC1 and PoC3, as well as recently arrived IDPs of the most intense conflict in South Sudan. Although In December 2016, REACH decided to refine the in Akobo. Data collection was expanded to Renk in Upper 158 Key Informants assessed the state had enjoyed a period of relative calm in 2016, methodology, moving from the AoO to the Area of Nile State in April 2017. since January 2017, conflict has reignited across the Knowledge (AoK) methodology, an approach collecting Data collected is aggregated to the settlement level and all 99 Settlements assessed state. Many areas in Upper Nile are largely inaccessible information at the settlement level. The most recent percentiles presented in this factsheet, unless otherwise Contact with Area of Knowledge to humanitarian actors due to insecurity and logistical OCHA Common Operational Dataset (COD) released specified, represent percent of settlements within Upper constraints. As a result, only limited information is in February 2016 has been used as the reference for Nile with that specific response. The displacement section KIs reported to be newly arrived available on the humanitarian situation outside major settlement names and locations. Through AoK, REACH on page 2 refers to the proportion of assessed KIs arrived 98% IDPs. displacement sites. collects data from a network of Key Informants (KIs) who within the previous month (newly arrived IDPs). -
Third Party Monitoring of the World Bank Rapid Results Health Project Final Report
Third Party Monitoring of the World Bank Rapid Results Health Project Final Report 1 / 17 Abbreviations BPHNS: Basic Package of Health and Nutrition Services CH: County Hospital CHD: County Health Department CMA: Christian Mission Aid CMD: Christian Mission for Development CO: Clinical Officer CPA: Comprehensive Peace Agreement FGD: Focus Group Discussions GO: Government GoSS: Government of the Republic of South Sudan (GoSS) HL: Health Link HPF: Health Pooled Fund IMA: IMA World Health IMC: International Medical Corps IO: In-Opposition IOM: International Organisation for Migration IP: Implementing Partner KII: Key Informant Interview LGSDP: Local Governance and Service Delivery Project. MoH: Ministry of Health NGO: Non-Governmental Organisation PHC: Primary Health Care PHCC: Primary Health Care Centre PHCU: Primary Health Care Unit PIU: Project Implementation Unit RRHP: Rapid Results Health Project SGBV: Sexual and Gender Based Violence SMC: Sudan Medical Care SSAID: South Sudan Agency for Internal Development UNKEA: Universal Network for Knowledge and Empowerment Agency WB: World Bank WV: World Vision TPM: Third Party Monitoring 2 / 17 Executive Summary and Findings 1. Introduction The World Bank’s portfolio for South Sudan contains a number of International Development Association’s (IDA) investment projects aimed at improving local governance and service delivery. Although the World Bank (WB) has put in place measures to mitigate political security and fiduciary risks, there remains a gap in managing operational risk in terms of monitoring and evaluation of its investment projects in South Sudan following the resumption of armed conflict in 2013. Due to its strong operational capacity and presence in South Sudan, WB contracted the International Organization for Migration (IOM) in June 2018 to implement Third Party Monitoring (TPM) activities of its Rapid Results Health Project (RRHP) currently being implemented in former Upper Nile State and Jonglei State, and the Local Government and Service Delivery Project (LOGOSEED).