Hypopituitarism May Be an Additional Feature of SIM1 and POU3F2 Containing 6Q16 Deletions in Children with Early Onset Obesity
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

S41467-020-18249-3.Pdf
ARTICLE https://doi.org/10.1038/s41467-020-18249-3 OPEN Pharmacologically reversible zonation-dependent endothelial cell transcriptomic changes with neurodegenerative disease associations in the aged brain Lei Zhao1,2,17, Zhongqi Li 1,2,17, Joaquim S. L. Vong2,3,17, Xinyi Chen1,2, Hei-Ming Lai1,2,4,5,6, Leo Y. C. Yan1,2, Junzhe Huang1,2, Samuel K. H. Sy1,2,7, Xiaoyu Tian 8, Yu Huang 8, Ho Yin Edwin Chan5,9, Hon-Cheong So6,8, ✉ ✉ Wai-Lung Ng 10, Yamei Tang11, Wei-Jye Lin12,13, Vincent C. T. Mok1,5,6,14,15 &HoKo 1,2,4,5,6,8,14,16 1234567890():,; The molecular signatures of cells in the brain have been revealed in unprecedented detail, yet the ageing-associated genome-wide expression changes that may contribute to neurovas- cular dysfunction in neurodegenerative diseases remain elusive. Here, we report zonation- dependent transcriptomic changes in aged mouse brain endothelial cells (ECs), which pro- minently implicate altered immune/cytokine signaling in ECs of all vascular segments, and functional changes impacting the blood–brain barrier (BBB) and glucose/energy metabolism especially in capillary ECs (capECs). An overrepresentation of Alzheimer disease (AD) GWAS genes is evident among the human orthologs of the differentially expressed genes of aged capECs, while comparative analysis revealed a subset of concordantly downregulated, functionally important genes in human AD brains. Treatment with exenatide, a glucagon-like peptide-1 receptor agonist, strongly reverses aged mouse brain EC transcriptomic changes and BBB leakage, with associated attenuation of microglial priming. We thus revealed tran- scriptomic alterations underlying brain EC ageing that are complex yet pharmacologically reversible. -

Appendix 2. Significantly Differentially Regulated Genes in Term Compared with Second Trimester Amniotic Fluid Supernatant
Appendix 2. Significantly Differentially Regulated Genes in Term Compared With Second Trimester Amniotic Fluid Supernatant Fold Change in term vs second trimester Amniotic Affymetrix Duplicate Fluid Probe ID probes Symbol Entrez Gene Name 1019.9 217059_at D MUC7 mucin 7, secreted 424.5 211735_x_at D SFTPC surfactant protein C 416.2 206835_at STATH statherin 363.4 214387_x_at D SFTPC surfactant protein C 295.5 205982_x_at D SFTPC surfactant protein C 288.7 1553454_at RPTN repetin solute carrier family 34 (sodium 251.3 204124_at SLC34A2 phosphate), member 2 238.9 206786_at HTN3 histatin 3 161.5 220191_at GKN1 gastrokine 1 152.7 223678_s_at D SFTPA2 surfactant protein A2 130.9 207430_s_at D MSMB microseminoprotein, beta- 99.0 214199_at SFTPD surfactant protein D major histocompatibility complex, class II, 96.5 210982_s_at D HLA-DRA DR alpha 96.5 221133_s_at D CLDN18 claudin 18 94.4 238222_at GKN2 gastrokine 2 93.7 1557961_s_at D LOC100127983 uncharacterized LOC100127983 93.1 229584_at LRRK2 leucine-rich repeat kinase 2 HOXD cluster antisense RNA 1 (non- 88.6 242042_s_at D HOXD-AS1 protein coding) 86.0 205569_at LAMP3 lysosomal-associated membrane protein 3 85.4 232698_at BPIFB2 BPI fold containing family B, member 2 84.4 205979_at SCGB2A1 secretoglobin, family 2A, member 1 84.3 230469_at RTKN2 rhotekin 2 82.2 204130_at HSD11B2 hydroxysteroid (11-beta) dehydrogenase 2 81.9 222242_s_at KLK5 kallikrein-related peptidase 5 77.0 237281_at AKAP14 A kinase (PRKA) anchor protein 14 76.7 1553602_at MUCL1 mucin-like 1 76.3 216359_at D MUC7 mucin 7, -

The Interaction of DNA Repair Factors ASCC2 and ASCC3 Is Affected by Somatic Cancer Mutations
ARTICLE https://doi.org/10.1038/s41467-020-19221-x OPEN The interaction of DNA repair factors ASCC2 and ASCC3 is affected by somatic cancer mutations Junqiao Jia 1, Eva Absmeier1,5, Nicole Holton1, Agnieszka J. Pietrzyk-Brzezinska1,6, Philipp Hackert2, ✉ Katherine E. Bohnsack 2, Markus T. Bohnsack2,3 & Markus C. Wahl 1,4 The ASCC3 subunit of the activating signal co-integrator complex is a dual-cassette Ski2-like nucleic acid helicase that provides single-stranded DNA for alkylation damage repair by the 1234567890():,; α-ketoglutarate-dependent dioxygenase AlkBH3. Other ASCC components integrate ASCC3/ AlkBH3 into a complex DNA repair pathway. We mapped and structurally analyzed inter- acting ASCC2 and ASCC3 regions. The ASCC3 fragment comprises a central helical domain and terminal, extended arms that clasp the compact ASCC2 unit. ASCC2–ASCC3 interfaces are evolutionarily highly conserved and comprise a large number of residues affected by somatic cancer mutations. We quantified contributions of protein regions to the ASCC2–ASCC3 interaction, observing that changes found in cancers lead to reduced ASCC2–ASCC3 affinity. Functional dissection of ASCC3 revealed similar organization and regulation as in the spliceosomal RNA helicase Brr2. Our results delineate functional regions in an important DNA repair complex and suggest possible molecular disease principles. 1 Laboratory of Structural Biochemistry, Freie Universität Berlin, D-14195 Berlin, Germany. 2 Department of Molecular Biology, University Medical Centre Göttingen, Göttingen, Germany. 3 Göttingen Center for Molecular Biosciences, Georg-August-Universität, Göttingen, Germany. 4 Helmholtz-Zentrum Berlin für Materialien und Energie, Macromolecular Crystallography, D-12489 Berlin, Germany. 5Present address: MRC Laboratory of Molecular Biology, Cambridge Biomedical Campus, Cambridge CB2 0QH, UK. -

Karla Alejandra Vizcarra Zevallos Análise Da Função De Genes
Karla Alejandra Vizcarra Zevallos Análise da função de genes candidatos à manutenção da inativação do cromossomo X em humanos Dissertação apresentada ao Pro- grama de Pós‐Graduação Inter- unidades em Biotecnologia USP/ Instituto Butantan/ IPT, para obtenção do Título de Mestre em Ciências. São Paulo 2017 Karla Alejandra Vizcarra Zevallos Análise da função de genes candidatos à manutenção da inativação do cromossomo X em humanos Dissertação apresentada ao Pro- grama de Pós‐Graduação Inter- unidades em Biotecnologia do Instituto de Ciências Biomédicas USP/ Instituto Butantan/ IPT, para obtenção do Título de Mestre em Ciências. Área de concentração: Biotecnologia Orientadora: Profa. Dra. Lygia da Veiga Pereira Carramaschi Versão corrigida. A versão original eletrônica encontra-se disponível tanto na Biblioteca do ICB quanto na Biblioteca Digital de Teses e Dissertações da USP (BDTD) São Paulo 2017 UNIVERSIDADE DE SÃO PAULO Programa de Pós-Graduação Interunidades em Biotecnologia Universidade de São Paulo, Instituto Butantan, Instituto de Pesquisas Tecnológicas Candidato(a): Karla Alejandra Vizcarra Zevallos Título da Dissertação: Análise da função de genes candidatos à manutenção da inativação do cromossomo X em humanos Orientador: Profa. Dra. Lygia da Veiga Pereira Carramaschi A Comissão Julgadora dos trabalhos de Defesa da Dissertação de Mestrado, em sessão pública realizada a ........./......../.........., considerou o(a) candidato(a): ( ) Aprovado(a) ( ) Reprovado(a) Examinador(a): Assinatura: .............................................................................. -

Improving the Detection of Genomic Rearrangements in Short Read Sequencing Data
Improving the detection of genomic rearrangements in short read sequencing data Daniel Lee Cameron orcid.org/0000-0002-0951-7116 Doctor of Philosophy July 2017 Department of Medical Biology, University of Melbourne Bioinformatics Division, Walter and Eliza Hall Institute of Medical Research Submitted in total fulfilment of the requirements of the degree of Doctor of Philosophy Produced on archival quality paper Page i Abstract Genomic rearrangements, also known as structural variants, play a significant role in the development of cancer and in genetic disorders. With the bulk of genetic studies focusing on single nucleotide variants and small insertions and deletions, structural variants are often overlooked. In part this is due to the increased complexity of analysis required, but is also due to the increased difficulty of detection. The identification of genomic rearrangements using massively parallel sequencing remains a major challenge. To address this, I have developed the Genome Rearrangement Identification Software Suite (GRIDSS). In this thesis, I show that high sensitivity and specificity can be achieved by performing reference-guided assembly prior to variant calling and incorporating the results of this assembly into the variant calling process itself. Utilising a novel genome-wide break-end assembly approach, GRIDSS halves the false discovery rate compared to other recent methods on human cell line data. A comparison of assembly approaches reveals that incorporating read alignment information into a positional de Bruijn graph improves assembly quality compared to traditional de Bruijn graph assembly. To characterise the performance of structural variant calling software, I have performed the most comprehensive benchmarking of structural variant calling software to date. -

Supplementary Information
Supplementary Information Table S1. Gene Ontology analysis of affected biological processes/pathways/themes in H1 hESCs based on sets of statistically significant differentially expressed genes. Exposures Overrepresented Categories (Upregulation) EASE Score Negative regulation of cell differentiation 0.0049 Lipid biosynthetic process 0.015 Negative regulation of cell proliferation 0.02 5 cGy, 2 h Transcription factor binding 0.037 Regulation of apoptosis 0.038 Positive regulation of anti-apoptosis 0.048 P53 signaling pathway 4.2 × 10−10 Positive regulation of apoptosis 7.5 × 10−8 Response to DNA damage stimulus 1.5 × 10−6 Cellular response to stress 9.6 × 10−6 1 Gy, 2 h Negative regulation of cell proliferation 9.8 × 10−6 Cell cycle arrest 7.0 × 10−4 Negative regulation of cell differentiation 1.5 × 10−3 Regulation of protein kinase activity 0.011 I-kappaB kinase/NF-kappaB cascade 0.025 Metallothionein superfamily 9.9 × 10−18 Induction of apoptosis 8.8 × 10−5 DNA damage response 2.6 × 10−4 1 Gy, 16 h Positive regulation of anti-apoptosis 0.001 Positive regulation of cell death 0.005 Cellular response to stress 0.012 Exposures Overrepresented Categories (Downregulation) EASE Score Alternative splicing 0.016 1 Gy, 2 h Chromatin organization 0.020 Chromatin assembly 2.0 × 10−6 Cholesterol biosynthesis 5.1 × 10−5 Macromolecular complex assembly 9.3 × 10−4 1 Gy, 16 h PPAR signaling pathway 0.007 Hemopoietic organ development 0.033 Immune system development 0.040 S2 Table S2. Gene Ontology analysis of affected biological processes/pathways/themes in H7 based on sets of statistically significant differentially expressed genes. -
Multiomic Analysis of the UV-Induced DNA Damage Response
Resource Multiomic Analysis of the UV-Induced DNA Damage Response Graphical Abstract Authors Stefan Boeing, Laura Williamson, Vesela Encheva, ..., Michael Howell, Ambrosius P. Snijders, Jesper Q. Svejstrup Correspondence [email protected] In Brief Boeing et al. investigate the UV-induced DNA damage response by combining a range of proteomic and genomic screens. A function in this response for the melanoma driver STK19 as well as a number of other factors are uncovered. Highlights d A multiomic screening approach examines the UV-induced DNA damage response d Multiple factors are connected to the transcription-related DNA damage response d Melanoma gene STK19 is required for a normal DNA damage response Boeing et al., 2016, Cell Reports 15, 1597–1610 May 17, 2016 ª 2016 The Author(s) http://dx.doi.org/10.1016/j.celrep.2016.04.047 Cell Reports Resource Multiomic Analysis of the UV-Induced DNA Damage Response Stefan Boeing,1,5 Laura Williamson,1 Vesela Encheva,2 Ilaria Gori,3 Rebecca E. Saunders,3 Rachael Instrell,3 Ozan Aygun,€ 1,7 Marta Rodriguez-Martinez,1 Juston C. Weems,4 Gavin P. Kelly,5 Joan W. Conaway,4,6 Ronald C. Conaway,4,6 Aengus Stewart,5 Michael Howell,3 Ambrosius P. Snijders,2 and Jesper Q. Svejstrup1,* 1Mechanisms of Transcription Laboratory, the Francis Crick Institute, Clare Hall Laboratories, South Mimms EN6 3LD, UK 2Protein Analysis and Proteomics Laboratory, the Francis Crick Institute, Clare Hall Laboratories, South Mimms EN6 3LD, UK 3High Throughput Screening Laboratory, the Francis Crick Institute, 44 Lincoln’s -

Metabolites OH
H OH metabolites OH Article Metabolite Genome-Wide Association Study (mGWAS) and Gene-Metabolite Interaction Network Analysis Reveal Potential Biomarkers for Feed Efficiency in Pigs Xiao Wang and Haja N. Kadarmideen * Quantitative Genomics, Bioinformatics and Computational Biology Group, Department of Applied Mathematics and Computer Science, Technical University of Denmark, Richard Petersens Plads, Building 324, 2800 Kongens Lyngby, Denmark; [email protected] * Correspondence: [email protected] Received: 1 April 2020; Accepted: 11 May 2020; Published: 15 May 2020 Abstract: Metabolites represent the ultimate response of biological systems, so metabolomics is considered the link between genotypes and phenotypes. Feed efficiency is one of the most important phenotypes in sustainable pig production and is the main breeding goal trait. We utilized metabolic and genomic datasets from a total of 108 pigs from our own previously published studies that involved 59 Duroc and 49 Landrace pigs with data on feed efficiency (residual feed intake (RFI)), genotype (PorcineSNP80 BeadChip) data, and metabolomic data (45 final metabolite datasets derived from LC-MS system). Utilizing these datasets, our main aim was to identify genetic variants (single-nucleotide polymorphisms (SNPs)) that affect 45 different metabolite concentrations in plasma collected at the start and end of the performance testing of pigs categorized as high or low in their feed efficiency (based on RFI values). Genome-wide significant genetic variants could be then used as potential genetic or biomarkers in breeding programs for feed efficiency. The other objective was to reveal the biochemical mechanisms underlying genetic variation for pigs’ feed efficiency. In order to achieve these objectives, we firstly conducted a metabolite genome-wide association study (mGWAS) based on mixed linear models and found 152 genome-wide significant SNPs (p-value < 1.06 10 6) in association with 17 metabolites that included 90 significant SNPs annotated × − to 52 genes. -
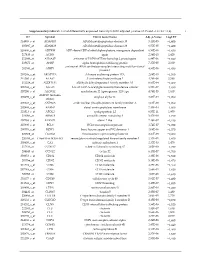
Supplementary Table S1. List of Differentially Expressed
Supplementary table S1. List of differentially expressed transcripts (FDR adjusted p‐value < 0.05 and −1.4 ≤ FC ≥1.4). 1 ID Symbol Entrez Gene Name Adj. p‐Value Log2 FC 214895_s_at ADAM10 ADAM metallopeptidase domain 10 3,11E‐05 −1,400 205997_at ADAM28 ADAM metallopeptidase domain 28 6,57E‐05 −1,400 220606_s_at ADPRM ADP‐ribose/CDP‐alcohol diphosphatase, manganese dependent 6,50E‐06 −1,430 217410_at AGRN agrin 2,34E‐10 1,420 212980_at AHSA2P activator of HSP90 ATPase homolog 2, pseudogene 6,44E‐06 −1,920 219672_at AHSP alpha hemoglobin stabilizing protein 7,27E‐05 2,330 aminoacyl tRNA synthetase complex interacting multifunctional 202541_at AIMP1 4,91E‐06 −1,830 protein 1 210269_s_at AKAP17A A‐kinase anchoring protein 17A 2,64E‐10 −1,560 211560_s_at ALAS2 5ʹ‐aminolevulinate synthase 2 4,28E‐06 3,560 212224_at ALDH1A1 aldehyde dehydrogenase 1 family member A1 8,93E‐04 −1,400 205583_s_at ALG13 ALG13 UDP‐N‐acetylglucosaminyltransferase subunit 9,50E‐07 −1,430 207206_s_at ALOX12 arachidonate 12‐lipoxygenase, 12S type 4,76E‐05 1,630 AMY1C (includes 208498_s_at amylase alpha 1C 3,83E‐05 −1,700 others) 201043_s_at ANP32A acidic nuclear phosphoprotein 32 family member A 5,61E‐09 −1,760 202888_s_at ANPEP alanyl aminopeptidase, membrane 7,40E‐04 −1,600 221013_s_at APOL2 apolipoprotein L2 6,57E‐11 1,600 219094_at ARMC8 armadillo repeat containing 8 3,47E‐08 −1,710 207798_s_at ATXN2L ataxin 2 like 2,16E‐07 −1,410 215990_s_at BCL6 BCL6 transcription repressor 1,74E‐07 −1,700 200776_s_at BZW1 basic leucine zipper and W2 domains 1 1,09E‐06 −1,570 222309_at -

Bedeutung Und Charakterisierung Der 6Q-Deletion Beim Prostatakarzinom
Bedeutung und Charakterisierung der 6q-Deletion beim Prostatakarzinom Dissertation zur Erlangung des Doktorgrades der Naturwissenschaften (Dr. rer. nat.) am Department Biologie der Fakultät Mathematik, Informatik und Naturwissenschaften der Universität Hamburg Vorgelegt von Martina Kluth Heide-Holstein Hamburg 2015 Gutachter der Dissertation Prof. Dr. Guido Sauter Prof. Dr. Thomas Dobner Datum der Disputation: 22.01.2016 Inhaltsverzeichnis 1Einleitung 1 1.1 Epidemiologie und Ätiologie des Prostatakarzinoms .............. 1 1.2 Früherkennung und Primärdiagnostik des Prostatakarzinoms .............................. 2 1.2.1 Digitale rektale Untersuchung (DRU) .................. 3 1.2.2 Prostataspezifisches Antigen (PSA) ................... 3 1.2.3 Stanzbiopsie der Prostata ........................ 5 1.3 Pathologie und Stadieneinteilung des Prostatakarzinoms ................................ 5 1.4 Therapie des Prostatakarzinoms ......................... 7 1.5 Prognosemarker beim Prostatakarzinom .................... 11 1.6 Genomische Veränderungen beim Prostatakarzinom .............. 12 1.6.1 Punktmutation .............................. 12 1.6.2 Chromosomale Zugewinne ........................ 12 1.6.3 Translokationen .............................. 13 1.6.4 Deletionen ................................. 14 1.7 Die 6q-Deletion beim Prostatakarzinom ..................... 15 1.7.1 Prävalenz der 6q-Deletion beim Prostatakarzinom ........... 15 1.7.2 Assoziation der 6q-Deletion mit dem Tumorphänotyp und der Progno- se des Prostatakarzinoms ........................ -

The Role of SMARCAD1 During Replication Stress Sarah Joseph
The role of SMARCAD1 during replication stress Sarah Joseph Submitted in partial fulfillment of the requirements for the degree of Doctor of Philosophy under the Executive Committee of the Graduate School of Arts and Sciences COLUMBIA UNIVERSITY 2020 © 2020 Sarah Joseph All Rights Reserved Abstract The role of SMARCAD1 during replication stress Sarah Joseph Heterozygous mutations in BRCA1 or BRCA2 predispose carriers to an increased risk for breast or ovarian cancer. Both BRCA1 and BRCA2 (BRCA1/2) play an integral role in promoting genomic stability through their respective actions during homologous recombination (HR) mediated repair and stalled replication fork protection from nucleolytic degradation. SMARCAD1 (SD1) is a SWI/SNF chromatin remodeler that has been implicated in promoting long-range end resection and contributes to HR. Using human cell lines, we show that SMARCAD1 promotes nucleolytic degradation in BRCA1/2-deficient cells dependent on its chromatin remodeling activity. Moreover, SMARCAD1 prevents DNA break formation and promotes fork restart at stalled replication forks. These studies identify a new role for SMARCAD1 at the replication fork. In addition to the work presented here, I discuss a method for introducing stop codons (nonsense mutations) into genes using CRISPR-mediated base editing, called iSTOP, and provide an online resource for accessing the sequence of iSTOP sgRNASs (sgSTOPs) for five base editor variants (VQR-BE3, EQR-BE3, VRER-BE3, SaBE3, and SaKKH-BE3) in humans and over 3 million targetable gene coordinates for eight eukaryotic species. Ultimately, with improvements to CRISPR base editors this method can help model and study nonsense mutations in human disease. Table of Contents List of Figures ................................................................................................................. -

Agricultural University of Athens
ΓΕΩΠΟΝΙΚΟ ΠΑΝΕΠΙΣΤΗΜΙΟ ΑΘΗΝΩΝ ΣΧΟΛΗ ΕΠΙΣΤΗΜΩΝ ΤΩΝ ΖΩΩΝ ΤΜΗΜΑ ΕΠΙΣΤΗΜΗΣ ΖΩΙΚΗΣ ΠΑΡΑΓΩΓΗΣ ΕΡΓΑΣΤΗΡΙΟ ΓΕΝΙΚΗΣ ΚΑΙ ΕΙΔΙΚΗΣ ΖΩΟΤΕΧΝΙΑΣ ΔΙΔΑΚΤΟΡΙΚΗ ΔΙΑΤΡΙΒΗ Εντοπισμός γονιδιωματικών περιοχών και δικτύων γονιδίων που επηρεάζουν παραγωγικές και αναπαραγωγικές ιδιότητες σε πληθυσμούς κρεοπαραγωγικών ορνιθίων ΕΙΡΗΝΗ Κ. ΤΑΡΣΑΝΗ ΕΠΙΒΛΕΠΩΝ ΚΑΘΗΓΗΤΗΣ: ΑΝΤΩΝΙΟΣ ΚΟΜΙΝΑΚΗΣ ΑΘΗΝΑ 2020 ΔΙΔΑΚΤΟΡΙΚΗ ΔΙΑΤΡΙΒΗ Εντοπισμός γονιδιωματικών περιοχών και δικτύων γονιδίων που επηρεάζουν παραγωγικές και αναπαραγωγικές ιδιότητες σε πληθυσμούς κρεοπαραγωγικών ορνιθίων Genome-wide association analysis and gene network analysis for (re)production traits in commercial broilers ΕΙΡΗΝΗ Κ. ΤΑΡΣΑΝΗ ΕΠΙΒΛΕΠΩΝ ΚΑΘΗΓΗΤΗΣ: ΑΝΤΩΝΙΟΣ ΚΟΜΙΝΑΚΗΣ Τριμελής Επιτροπή: Aντώνιος Κομινάκης (Αν. Καθ. ΓΠΑ) Ανδρέας Κράνης (Eρευν. B, Παν. Εδιμβούργου) Αριάδνη Χάγερ (Επ. Καθ. ΓΠΑ) Επταμελής εξεταστική επιτροπή: Aντώνιος Κομινάκης (Αν. Καθ. ΓΠΑ) Ανδρέας Κράνης (Eρευν. B, Παν. Εδιμβούργου) Αριάδνη Χάγερ (Επ. Καθ. ΓΠΑ) Πηνελόπη Μπεμπέλη (Καθ. ΓΠΑ) Δημήτριος Βλαχάκης (Επ. Καθ. ΓΠΑ) Ευάγγελος Ζωίδης (Επ.Καθ. ΓΠΑ) Γεώργιος Θεοδώρου (Επ.Καθ. ΓΠΑ) 2 Εντοπισμός γονιδιωματικών περιοχών και δικτύων γονιδίων που επηρεάζουν παραγωγικές και αναπαραγωγικές ιδιότητες σε πληθυσμούς κρεοπαραγωγικών ορνιθίων Περίληψη Σκοπός της παρούσας διδακτορικής διατριβής ήταν ο εντοπισμός γενετικών δεικτών και υποψηφίων γονιδίων που εμπλέκονται στο γενετικό έλεγχο δύο τυπικών πολυγονιδιακών ιδιοτήτων σε κρεοπαραγωγικά ορνίθια. Μία ιδιότητα σχετίζεται με την ανάπτυξη (σωματικό βάρος στις 35 ημέρες, ΣΒ) και η άλλη με την αναπαραγωγική