Highly Prevalent Falciparum Malaria in North West Guyana: Its Development History and Control Problems1
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

213Th Sitting April 1980 THEPARLIAMENTARYDEBAT ESOFFICIALREPORT /Volume 7
213th Sitting April 1980 T H E P A R L I A M E N T A R Y D E B A T E S O F F I C I A L R E P O R T /Volume 7/ PROCEEDINGS AND DEBATES OF THE FIRST SESSION OF THE NATIONAL ASSEMBLY OF THE THIRD PARLIAMENT OF GUYANA UNDER THE CONSTITUTION OF GUYANA 213th Sitting 2 p.m. Monday, 14th April 1980 MEMBERS OF THE NATIONAL ASSEMBLY (63) Speaker Cde. Sase Narain, O.R., J.P., Speaker Members of the Government - People’s National Congress (46) Prime Minister (1) Cde. L.F.S. Burnham, O.E., S.C., (Absent - on leave) Prime Minister Deputy Prime Minister (1) Cde. P.A. Reid, O.E., Deputy Prime Minister and Minister of (Absent) National Development Senior Ministers (11) Cde. H.D. Hoyte, S. C., Minister of Economic Development and Co-operatives Cde. S.S. Naraine, A.A., Minister of Works and Transport Cde. B. Ramsaroop, Minister of Parliamentary Affairs and Leader of the House Cde. C.V. Mingo, Minister of Home Affairs *Cde. H. Green, Minister of Health, Housing and Labour *Cde. H O . Jack, Minister of Energy and Natural Resources (Absent) *Cde. F.E. Hope, Minister of Finance (Absent) *Cde. G.B. Kennard, C.C.H. Minister of Agriculture (Absent - on leave) *Cde. M. Shahabuddeen, O. R., S.C., Attorney General and Minister of Justice (Absent) *Cde. R.E. Jackson, Minister of Foreign Affairs (Absent - on leave) *Cde. J.A .Tyndall, A.A., Minister of Trade and Consumer Protection *Non-elected Ministers 1 Ministers (2) Cde. -

Republic of Guyana APPLICATION for FIREARM LICENCE (BY an AMERINDIAN LIVING in a REMOTE VILLAGE OR COMMUNITY)
Republic of Guyana APPLICATION FOR FIREARM LICENCE (BY AN AMERINDIAN LIVING IN A REMOTE VILLAGE OR COMMUNITY) INSTRUCTION: Please complete application in CAPITAL LETTERS. Failure to complete all sections will affect processing of the application. If you need more space for any section, print an additional page containing the appropriate section, complete and submit with application. Last Name: Maiden Name: Photograph of First Name: Applicant Middle Name: Alias: FOR OFFICIAL USE ONLY Police Division: __________________ Date: ______/____/____ Form Number: _____________ yyyy/mm/dd Applicants are required to submit two (2) recent passport size photographs, along with the following documents to facilitate processing of the application: DOCUMENTS REQUIRED (Copies and original for verification, where applicable) 1. Birth Certificate, Naturalization or Registration Certificate (if applicable) 2. National Identification Card or Passport (if applicable) 3. Two (2) recent testimonials in support of the application 4. Evidence of farming activities 5. Evidence of occupation of land 6. Firearms Licensing Approval Board Medical Report NOTE: Applicants are advised that the submission of photographic evidence of their farms will be helpful. PROCESSING FEE All successful applicants are required to pay a processing fee. The fee applicable to Amerindians living in remote villages and communities is $ 2,500 (Shotgun). PLEASE REFER TO THE ATTACHED LIST OF REMOTE VILLAGES AND COMMUNITIES. 1 Application Process for a Firearm Licence The process from application to final approval or rejection for a firearm licence is as follows: 1. The applicant completes the Firearm Licence Application Form, and submits along with a Medical Report for Firearm Licence, and the required documentation to ONE of the following locations: a. -
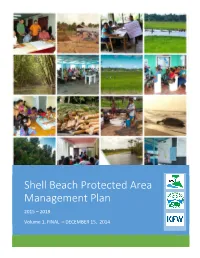
Shell Beach Protected Area Management Plan
Shell Beach Protected Area Management Plan 2015 – 2019 Volume 1, FINAL – DECEMBER 15, 2014 Volume 1. SBPA Management Plan - Final, December 15, 2014 Table of Contents Management Plan Approval Page .................................................................................................. iv Acronyms and Abbreviations ........................................................................................................... v Executive Summary ......................................................................................................................... vi 1 Management Plan Introduction .............................................................................................. 1 1.1 Management Plan Purpose .............................................................................................. 1 1.2 Management Planning Process ........................................................................................ 1 2 Shell Beach Protected Area (SBPA) ......................................................................................... 2 2.1 SBPA Establishment .......................................................................................................... 2 2.2 Description of Place and Biodiversity ............................................................................... 4 2.3 Description of Communities, Livelihoods, and Economic Activity ................................... 7 3 SBPA Management Framework ............................................................................................. -

Guyana REGION VI Sub-Regional Land Use Plan
GUYANA LANDS AND SURVEYS COMMISSION REGION VI Sub-Regional LAND USE PLAN Andrew R. Bishop, Commissioner Guyana Lands and Surveys Commission 22 Upper Hadfield Street, Durban Backlands, Georgetown Guyana September 2004 Acknowledgements The Guyana Lands and Surveys Commission wishes to thank all Agencies, Non- Governmental Organizations, Individuals and All Stakeholders who contributed to this Region VI Sub-Regional Land Use Plan. These cannot all be listed, but in particular we recognised the Steering Committee, the Regional Democratic Council, the Neighbourhood Democratic Councils, the members of the Public in Berbice, and most importantly, the Planning Team. i Table of Contents Acknowledgements ....................................................................................................... i Table of Contents ...................................................................................................... ii Figures ...................................................................................................... v Tables ...................................................................................................... v The Planning Team ..................................................................................................... vi The Steering Committee ................................................................................................... vii Support Staff .................................................................................................... vii List of Acronyms .................................................................................................. -
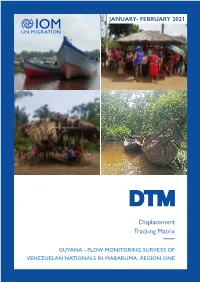
Displacement Tracking Matrix
JANUARY- FEBRUARY 2021 Displacement Tracking Matrix GUYANA - FLOW MONITORING SURVEYS OF VENEZUELAN NATIONALS IN MABARUMA, REGION ONE Displacement GUYANA - MABARUMA, REGION ONE Tracking Matrix January-February 2021 CONTENTS 1. EXECUTIVE SUMMARY . .3 2. CONCEPT . 4 3. INTRODUCTION. .4 4. METHODOLOGY. .6 5. POPULATION PROFILE. 6 6. MIGRATION ROUTE AND STATUS. .8 7. ECONOMIC AND LABOUR SITUATION . .12 8. HEALTH ACCESS. .15 9. NEEDS AND ASSISTANCE. 16 10. PROTECTION . 18 DISCLAIMERS AND COPYRIGHT The opinions expressed in the report are those of the authors and do not necessarily reflect the views of the International Organization for Migration (IOM). The designations employed and the presentation of material throughout the report do not imply the expression of any opinion whatsoever on the part of IOM concerning the legal status of any country, territory, city or area, or of its authorities, or concerning its frontiers or boundaries. IOM is committed to the principle that humane and orderly migration benefits migrants and society. As an intergovernmental organization, IOM acts with its partners in the international community to assist in the meeting of operational challenges of migration; advance understanding of migration issues; encourage social and economic development through migration; and uphold the human dignity and well-being of migrants. All rights reserved. No part of this publication may be reproduced, stored in a retrieval system, or transmitted in any form or by any means, electronic, mechanical, photocopying, recording, or otherwise without the prior written permission of the publisher. International Organization for Migration 107 -108 Duke Street UN Common House Kingston, Georgetown Guyana, South America Tel.: +592 -225-375 E-mail: [email protected] Website: www.iom.int This DTM activity was funded by the US Department of State – Bureau of Population, Refugees, and Migration (BPRM) and implemented by IOM. -
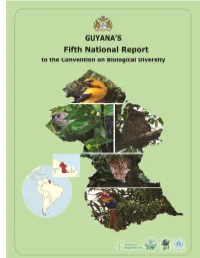
CBD Fifth National Report
i ii GUYANA’S FIFTH NATIONAL REPORT TO THE CONVENTION ON BIOLOGICAL DIVERSITY Approved by the Cabinet of the Government of Guyana May 2015 Funded by the Global Environment Facility Environmental Protection Agency Ministry of Natural Resources and the Environment Georgetown September 2014 i ii Table of Contents ACKNOWLEDGEMENT ........................................................................................................................................ V ACRONYMS ....................................................................................................................................................... VI EXECUTIVE SUMMARY ......................................................................................................................................... I 1. INTRODUCTION .............................................................................................................................................. 1 1.1 DESCRIPTION OF GUYANA .......................................................................................................................................... 1 1.2 RATIFICATION AND NATIONAL REPORTING TO THE UNCBD .............................................................................................. 2 1.3 BRIEF DESCRIPTION OF GUYANA’S BIOLOGICAL DIVERSITY ................................................................................................. 3 SECTION I: STATUS, TRENDS, THREATS AND IMPLICATIONS FOR HUMAN WELL‐BEING ...................................... 12 2. IMPORTANCE OF BIODIVERSITY -
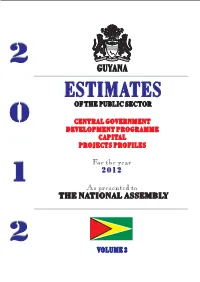
Estimates of the Public Sector for the Year 2012 Volume 3
2 2 GUYANA P P U U B B ESTIMATES L L OF THE PUBLIC SECTOR I I C C S S 0 CENTRAL GOVERNMENT E E DEVELOPMENT PROGRAMME C C T CAPITAL V T GUY O O OL PROJECTS PROFILES R R UME ANA 2 2 For the year 0 0 2012 1 1 3 2 2 1 As presented to E E S S THE NATIONAL ASSEMBLY T T I I M M A A T T E Presented to Parliament in March, 2012 E by the Honourable Dr. Ashni Singh, Minister of Finance. S Produced and Compiled by the Office of the Budget, Ministry of Finance S 2 VOLUME 3 Printed by Guyana National Printers Limited INDEX TO CENTRAL GOVERNMENT CAPITAL PROJECTS DIVISION AGENCYPROGRAMME PROJECT TITLE REF. # 1 OFFICE OF THE PRESIDENT 011 - Head Office Administration Office and Residence of the President 1 1 OFFICE OF THE PRESIDENT 011 - Head Office Administration Information Communication Technology 2 1 OFFICE OF THE PRESIDENT 011 - Head Office Administration Minor Works 3 1 OFFICE OF THE PRESIDENT 011 - Head Office Administration Land Transport 4 1 OFFICE OF THE PRESIDENT 011 - Head Office Administration Purchase of Equipment 5 1 OFFICE OF THE PRESIDENT 011 - Head Office Administration Civil Defence Commission 6 1 OFFICE OF THE PRESIDENT 011 - Head Office Administration Joint Intelligence Coordinating Centre 7 1 OFFICE OF THE PRESIDENT 011 - Head Office Administration Land Use Master Plan 8 1 OFFICE OF THE PRESIDENT 011 - Head Office Administration Guyana Office for Investment 9 1 OFFICE OF THE PRESIDENT 011 - Head Office Administration Government Information Agency 10 1 OFFICE OF THE PRESIDENT 011 - Head Office Administration Guyana Energy Agency 11 -

1.2 Original Project Development Objectives (PDO) and Key Indicators
Document of The World Bank Public Disclosure Authorized Report No: ICR00001863 IMPLEMENTATION COMPLETION AND RESULTS REPORT (IDA-P088030) ON A Public Disclosure Authorized GRANT IN THE AMOUNT OF SDR 7.5 MILLION (US$ 11.3 MILLION EQUIVALENT) TO THE REPUBLIC OF GUYANA FOR A WATER SECTOR CONSOLIDATION PROJECT Public Disclosure Authorized SEPTEMBER 22, 2011 Urban, Water and Disaster Risk Management Department Caribbean Country Management Unit Latin America and Caribbean Region Public Disclosure Authorized CURRENCY EQUIVALENTS (Exchange Rate Effective 05-10-11) Currency Unit= 1.0 = US$ 0.0049 US$ 1.00 = GYD 206 FISCAL YEAR January1 – December 31 ABBREVIATIONS AND ACRONYMS CAS Country Assistance Strategy DFID Department for International Development (U.K.) GoG Government of Guyana GS&WC Georgetown Sewerage and Water Commissioners GUYWA Guyana Water Authority GWI Guyana Water Incorporated IDB Inter-American Development Bank IDA International Development Association MC Management Contract NRW Non Revenue Water O&M Operations and Maintenance PAD Project Appraisal Document PDO Project Development Objectives PIU Project Implementation Unit WTP Water Treatment Plant Vice President: Pamela Cox Country Director: Francoise Clottes Sector Manager: GuangZhe Chen Project Team Leader: Patricia Lopez ICR Team Leader: John Morton ii Guyana Water Sector Consolidation Project CONTENTS Data Sheet A. Basic Information ....................................................................................................... v B. Key Dates .................................................................................................................. -

Green State Development Strategy: Vision 2040
Diversified, Resilient, Low-carbon, People-centred VOLUME I POLICY RECOMMENDATIONS, FINANCIAL MECHANISM & IMPLEMENTATION An inclusive and prosperous Guyana that provides a good quality of life for all its citizens “ based on sound education and social protection, low-carbon resilient development, new economic opportunities, justice, and political empowerment. ” Executive Summary Background The Green State Development Strategy: Vision 2040 is Guyana’s twenty-year, national development policy that reflects the guiding vision and principles of the ‘green agenda’: “An inclusive and prosperous Guyana that provides a good quality of life for all its citizens based on sound education and social protection, low-carbon and resilient development, providing new economic opportunities, justice and political empowerment.” The central objective is development that provides a better quality of life for all Guyanese derived from the country’s natural wealth – its diversity of people and abundant natural resources (land, water, forests, mineral and aggregates, biodiversity). The vision of the ‘green agenda’ is centred on principles of a green economy defined by sustainable, low-carbon and resilient development that uses its resources efficiently, and sustained over generations. The development philosophy emphasises the importance of a more cohesive society based on principles of equity and tolerance between ethnic groups – recognising that diversity of culture and heritage is the underlying strength of the country’s human capital. Development objectives therefore seek to improve the health, education and overall well-being of Guyanese citizens, to lift people out of poverty through an economy that generates decent jobs and that provides opportunities for sustaining livelihoods over the long term. For decades, geopolitical events, natural disasters and global commodity price swings have weighed upon Guyana’s development. -

To Operators Conducting Domestic Air Transport During Covid- 19 Pandemic
AIC B21/20 PHONE : 592-261-2269 FAX : 592-261-2279 AFS WHITE : SYCJYOYX AERONAUTICAL INFORMATION SERVICE EMAIL : aisguyana@gcaa- gy.org st Control Tower Complex, Timehri 01 AUGUST, 2020 EAST BANK DEMERARA GUYANA TO OPERATORS CONDUCTING DOMESTIC AIR TRANSPORT DURING COVID- 19 PANDEMIC. AUTHORITY The Director General of the Guyana Civil Aviation Authority (GCAA) hereby issues this Directive under the authority of section 143 (1) (a) of the Civil Aviation Act 2018. APPLICABILITY This DIRECTIVE is applicable to all air operators conducting air transport operations within Guyana. EFFECTIVITY This DIRECTIVE is effective from 00:00hrs UTC on 01ST August 2020 until 23:59hrs UTC on 15th August 2020. PURPOSE The purpose of this DIRECTIVE is to enhance Public Health in wake of the Novel Coronavirus (COVID-19) global pandemic. DEFINITION For the purpose of this Directive, the following definition shall apply: Operator: means a person, organisation or enterprise, engaged in or offering to engage in, aircraft operations, and any person who causes or authorises the operation of aircraft, in the capacity of owner, lessee or otherwise, whether with or without the control of the aircraft. ……………………………………………………………………………………………. DIRECTIVE RESTRICTION OF FLIGHTS WITHIN GEORGETOWN FLIGHT INFORMATION REGION 1. With effect from 00:00hrs UTC on 01st August 2020 until 23:59hrs UTC on 15th August 2020, the following conditions shall apply to all flights within Guyana: a) Transportation of foreign nationals to and from all border locations is suspended. These includes the following; North West – Mabaruma, Port Kaituma, Mathew's Ridge, Baramita, Bemichi and also Moruka(accessible via Port Kaituma and Bemichi) West - Eteringbang, Arau and Kaikan. -
![1 the PARLIAMENTARY DEBATES OFFICIAL REPORTS [Volume 7]](https://docslib.b-cdn.net/cover/3868/1-the-parliamentary-debates-official-reports-volume-7-1223868.webp)
1 the PARLIAMENTARY DEBATES OFFICIAL REPORTS [Volume 7]
216th Sitting April 1980 THE PARLIAMENTARY DEBATES OFFICIAL REPORTS [Volume 7] PROCEEDINGS AND DEBATES OF THE FIRST SESSION OF THE NATIONAL ASSEMBLY OF THE THIRD PARLIAMENT OF GUYANA UNDER THE CONSTITUTION OF THE CO-OPERATIVE REPUBLIC OF GUYANA 216th Sitting 2 p.m. Thursday, 17th April, 1980 MEMBERS OF THE NATIONAL ASSEMBLY (63) Speaker Cde. Sase Narain, O.R., J.P., Speaker Members of the Government – People’s National Congress (46) Prime Minister (1) Cde. L.F.S. Burnham, O.E., S.C., (Absent – on leave) Prime Minister Deputy Prime Minister (1) Cde. P.A. Reid, O.E., (Absent) Deputy Prime Minister and Minister of National Development Senior Ministers (11) Cde. H.D. Hoyte, S.C., Minister of Economic Development and Co-operatives Cde. S.S. Naraine, A.A., Minister of Works and Transport Cde. B. Ramsaroop, Minister of Parliamentary Affairs and Leader of the House Cde. C.V Mingo, Minister of Home Affairs *Cde. H. Green, Minister of Health, Housing and Labour *Cde. H.O. Jack, Minister of Energy and Natural Resources *Cde. F.E. Hope, (Absent) Minister of Finance *Cde. G.B. Kennard, C.C.H., (Absent – on leave) Minister of Agriculture *Cde. M. Shahabuddeen, O.R., S.C., Attorney General and Minister of Justice *Cde. R.E. Jackson, (Absent - on leave) Minister of Foreign Affairs *Cde. J.A. Tyndall, A.A., (Absent) Minister of Trade and Consumer Protection *Non-elected Ministers 1 Ministers (2) Cde. O.E. Clarke, Minister – Regional (East Berbice/Corentyne) Cde. C.A. Nascimento, Minister, Office of the Prime Minister (Absent – on leave) Ministers of State (10) Cde. -

Eradicating Poverty and Unifying Guyana
NATIONAL DEVELOPMENT STRATEGY Eradicating Poverty and Unifying Guyana A Civil Society Document - AN OVERVIEW - I GUYANA - BASIC INFORMATION • Guyana, with an area of 83,000 square miles or 215,000 square kilometres, is located on the northern coast of South America, and is the only English-speaking country on that continent. It is bounded on the north by the Atlantic Ocean, on the east by Surinam, on the south and south-west by Brazil, and on the west and north-west by Venezuela. • Guyana is physically divided into four types of landforms: (i) a flat coastal, clayey belt which is about 4.5 feet below sea level, and in which most of its agricultural activity occurs; (ii) a sand belt, to the south of the coastal belt, which includes the Intermediate Savannas; (iii) an undulating, central peneplain which comprises more than half of the country’s area, and in which are located lush, almost pristine, tropical forests, and extensive mineral deposits. This landform stretches from the sand belt to the country’s southern boundary and encompasses, also, the Rupununi Savannas which border Brazil; and (iv) the highlands which are to be found in the midwestern area. This portion of the Guiana Highlands includes the Pakaraima mountain range. • Guyana has a plentitude of natural resources: fertile agricultural lands on the coastal plain and in the riverain areas; vast areas of tropical hardwood forests of various ecosystems and with a multitude of plant and animal species; abundant fish and shrimping grounds, both in its numerous rivers and in the Atlantic Ocean to its north; and a wide variety of minerals, including gold, diamonds, a range of semi-precious stones, bauxite and manganese.