Themed Visit to People with Dementia in Community Hospitals
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Emergency Department Activity
NHS Scotland - Emergency Department Activity Attendances and Performance against the 4-hour Waiting Time Standard This is an ISD Scotland National Statistics release. The Scottish Government waiting time standard for emergency departments is that 98 % of all attendances should be seen within 4 hours. The figures presented in these tables detail the performance of each individual site and NHS board against the standard. Time Period: Apr-10 to Mar-11 Source: A&E data mart, ISD Scotland Date: 07 May 2012 List of Tables Table 1: Attendances and performance against 4-hour standard, Apr-10 to Mar-11 Total attendances, number of attendances breaching standard and attendances meeting standard (number and percentage). Figures are given at site and NHS Board level. Table 2: Attendances, Apr-10 to Mar-11 Summary table of attendances only. Figures are given at site and NHS Board level. Table 3: Performance against 4-hour standard, Apr-10 to Mar-11 Summary table of percentage of attendances meeting standard. Figures are given at site and NHS Board level. Notes: 1) The waiting time is defined as the time of arrival until the time of discharge, admission or transfer. 2) New presentations only; excludes planned return and recall attendances. 3) There are two types of site that provide emergency care; • ED - Emergency Departments; sites that provide a 24 hour emergency medicine consultant led service • MIU/Other - sites including minor injuries units (MIU), small hospitals and health centres in rural areas that carry out emergency department related activity and are GP or Nurse led. They may or may not be open 24 hours. -

Contract Between Scottish Ministers
CONTRACT BETWEEN SCOTTISH MINISTERS AND GEOAMEY PECS LTD FOR THE SCOTTISH COURT CUSTODY AND PRISONER ESCORT SERVICE (SCCPES) REFERENCE: 01500 MARCH 2018 Official No part of this document may be disclosed orally or in writing, including by reproduction, to any third party without the prior written consent of SPS. This document, its associated appendices and any attachments remain the property of SPS and will be returned upon request. 1 | P a g e 01500 Scottish Court Custody and Prisoner Escort Service (SCCPES) FORM OF CONTRACT CONTRACT No. 01500 This Contract is entered in to between: The Scottish Ministers, referred to in the Scotland Act 1998, represented by the Scottish Prison Service at the: Scottish Prison Service Calton House 5 Redheughs Rigg Edinburgh EH12 9HW (hereinafter called the “Purchaser”) OF THE FIRST PART And GEOAmey PECS Ltd (07556404) The Sherard Building, Edmund Halley Road Oxford OX4 4DQ (hereinafter called the “Service Provider”) OF THE SECOND PART The Purchaser hereby appoints the Service Provider and the Service Provider hereby agrees to provide for the Purchaser, the Services (as hereinafter defined) on the Conditions of Contract set out in this Contract. The Purchaser agrees to pay to the Service Provider the relevant sums specified in Schedule C and due in terms of the Contract, in consideration of the due and proper performance by the Service Provider of its obligations under the Contract. The Service Provider agrees to look only to the Purchaser for the due performance of the Contract and the Purchaser will be entitled to enforce this Contract on behalf of the Scottish Ministers. -

Accident and Emergency: Performance Update
Accident and Emergency Performance update Prepared by Audit Scotland May 2014 Auditor General for Scotland The Auditor General’s role is to: • appoint auditors to Scotland’s central government and NHS bodies • examine how public bodies spend public money • help them to manage their finances to the highest standards • check whether they achieve value for money. The Auditor General is independent and reports to the Scottish Parliament on the performance of: • directorates of the Scottish Government • government agencies, eg the Scottish Prison Service, Historic Scotland • NHS bodies • further education colleges • Scottish Water • NDPBs and others, eg Scottish Police Authority, Scottish Fire and Rescue Service. You can find out more about the work of the Auditor General on our website: www.audit-scotland.gov.uk/about/ags Audit Scotland is a statutory body set up in April 2000 under the Public Finance and Accountability (Scotland) Act 2000. We help the Auditor General for Scotland and the Accounts Commission check that organisations spending public money use it properly, efficiently and effectively. Accident and Emergency | 3 Contents Summary 4 Key messages 7 Part 1. A&E waiting times 9 Part 2. Reasons for delays in A&E 20 Part 3. Action by the Scottish Government 37 Endnotes 41 Appendix 1. NHS Scotland A&E departments and minor injury units 43 Appendix 2. National context for A&E and unscheduled care, 2004 to 2014 45 Exhibit data When viewing this report online, you can access background data by clicking on the graph icon. The data file will -

Emergency Departments
ED Site List 220711 v2.xls NHS Scotland - Emergency Departments Table 1: NHS Scotland - list of sites providing emergency care File NHS Board Site Type Location Name Location Address Comments Type Ayrshire & Arran ED Ayr Hospital DALMELLINGTON ROAD, AYR, KA6 6DX E Crosshouse Hospital KILMARNOCK ROAD, KILMARNOCK, AYRSHIRE, KA2 0BE E MIU/Other Arran War Memorial Hospital LAMLASH, ISLE OF ARRAN, KA27 8LF A Davidson Cottage Hospital THE AVENUE, GIRVAN, KA26 9DS A Closed from May-10 Girvan Community Hospital BRIDGEMILL, GIRVAN, AYRSHIRE, KA26 9HQ A Opened from May-10 Lady Margaret Hospital COLLEGE ST, MILLPORT, ISLE OF CUMBRAE, KA28 0HF A Opened from Oct-07 Borders ED Borders General Hospital MELROSE, TD6 9BS E MIU/Other Hawick Cottage Hospital VICTORIA ROAD, HAWICK, TD9 7AH A Hay Lodge Hospital NEIDPATH ROAD, PEEBLES, EH45 8JG A Kelso Hospital INCH ROAD, KELSO, TD5 7JP A Knoll Hospital STATION ROAD, DUNS, TD11 3EL A Dumfries & Galloway ED Dumfries & Galloway Royal Infirmary BANKEND ROAD, DUMFRIES, DG1 4AP E Galloway Community Hospital DALRYMPLE STREET, STRANRAER, DG9 7DQ E MIU/Other Castle Douglas Hospital ACADEMY STREET, CASTLE DOUGLAS, DG7 1EE A Kirkcudbright Hospital TOWNEND, KIRKCUDBRIGHT, DG6 4BE A Moffat Hospital HOLMEND, MOFFAT, DG10 9JY A Newton Stewart Hospital NEWTON STEWART, DG8 6LZ A Fife ED Victoria Hospital HAYFIELD ROAD, KIRKCALDY, KY2 5AH E MIU/Other Adamson Hospital BANK STREET, CUPAR, KY15 4JG A Queen Margaret Hospital WHITEFIELD ROAD, DUNFERMLINE, KY12 0SU E St Andrews Memorial Hospital ABBEY WALK, ST ANDREWS, KY16 9LG -

Emergency Departments
ED-site-list NHS Scotland - Emergency Departments Table 1: NHS Scotland - list of sites providing emergency care NHS Board Site Type Location Name Location Address File Type Comments Ayrshire & Arran ED Ayr Hospital DALMELLINGTON ROAD, AYR, KA6 6DX E Crosshouse Hospital KILMARNOCK ROAD, KILMARNOCK, AYRSHIRE, KA2 0BE E MIU/Other Arran War Memorial Hospital LAMLASH, ISLE OF ARRAN, KA27 8LF A Davidson Cottage Hospital THE AVENUE, GIRVAN, KA26 9DS A Closed from May-10 Girvan Community Hospital BRIDGEMILL, GIRVAN, AYRSHIRE, KA26 9HQ A Opened from May-10 Lady Margaret Hospital COLLEGE ST, MILLPORT, ISLE OF CUMBRAE, KA28 0HF A Opened from Oct-07 Borders ED Borders General Hospital MELROSE, TD6 9BS E MIU/Other Hawick Cottage Hospital VICTORIA ROAD, HAWICK, TD9 7AH A Hay Lodge Hospital NEIDPATH ROAD, PEEBLES, EH45 8JG A Kelso Hospital INCH ROAD, KELSO, TD5 7JP A Knoll Hospital STATION ROAD, DUNS, TD11 3EL A Dumfries & Galloway ED Dumfries & Galloway Royal Infirmary BANKEND ROAD, DUMFRIES, DG1 4AP E Galloway Community Hospital DALRYMPLE STREET, STRANRAER, DG9 7DQ E MIU/Other Castle Douglas Hospital ACADEMY STREET, CASTLE DOUGLAS, DG7 1EE A Kirkcudbright Hospital TOWNEND, KIRKCUDBRIGHT, DG6 4BE A Moffat Hospital HOLMEND, MOFFAT, DG10 9JY A Newton Stewart Hospital NEWTON STEWART, DG8 6LZ A Fife ED Queen Margaret Hospital WHITEFIELD ROAD, DUNFERMLINE, KY12 0SU E Victoria Hospital HAYFIELD ROAD, KIRKCALDY, KY2 5AH E MIU/Other Adamson Hospital BANK STREET, CUPAR, KY15 4JG A St Andrews Memorial Hospital ABBEY WALK, ST ANDREWS, KY16 9LG A Forth Valley -

Service Mapping
Moray CHSCP November 2011 RCOP in Moray APPENDIX 5: SERVICE MAPPING Service Mapping 2010-2011 This service mapping document seeks to identify and map provision within the Moray health and social care system, regardless of provider, which currently provides care and support services to older people. The aim of this mapping is to establish what activity is being carried out and by whom. It has been used as the basis for gaps analysis and service development SERVICE MAPPING Contents Appendix 5: service mapping .................................................................................... 1 SERVICE MAPPING ....................................................................................................... 2 Contents ..................................................................................................................... 2 Introduction ................................................................................................................ 6 A: Primary Healthcare................................................................................................. 10 1 GP Practices ......................................................................................................... 10 1.1 Overview ....................................................................................................... 10 1.2 Quality .......................................................................................................... 13 1.2.1 2009/10 Scottish GP Patient Experience Survey ........................................... -

ROH Representative Policy
Policy on Supplier Representatives Policy author Matthew Revell Accountable Executive Lead Jonathan Lofthouse Approving body Policy reference ROH/XXX/NNN [Assigned by Governance Team] POLICY APPROVAL DATE: ESSENTIAL READING FOR THE FOLLOWING STAFF GROUPS: May 2017 1 – All Trust Staff working in Theatres and Pharmacy POLICY 2 – Staff working in partnership with supplier IMPLEMENTATION DATE: representatives June 2016 DATE POLICY TO STAFF GROUPS WHICH SHOULD BE AWARE OF THE POLICY FOR BE REVIEWED: REFERENCE PURPOSES: June 2017 1 – Staff involved with purchasing or procurement DOCUMENT CONTROL AND HISTORY Version Date Date of Next Reason for change (e.g. full rewrite, No Approved implementation Review amendment to reflect new legislation, Date updated flowchart, etc.) 1 June 2017 New Policy Policy on Supplier Representation April 2017 2 | P a g e Policy on Supplier Representatives KEY POINTS 1. Supplier Representatives must not enter any area without an appointment. 2. Supplier Representatives must be registered on the Medical Industry Accredited System. 3. If the meeting is to discuss ANY new product or service then Procurement and Supplies must be informed. 4. Cold calling is not acceptable. 5. Pharmacy representatives must report to Pharmacy. 6. No electro-medical equipment can be used until tested by EBME. 7. Representatives visiting Theatre areas must comply with the Theatre protocol. 8. No sample products can be trialed until the appropriate trials and indemnity documentation has been completed. 9. Contractors undertaking work on the Trust’s sites must adhere to the Control of Contractors Policy. Do’s and Don’ts Do meet the supplier representative at an arranged point and don’t allow them to wander around clinical areas unaccompanied. -
MASTER) Hospital List (Updated October 2015
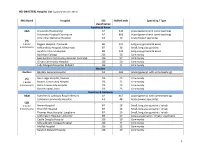
HEI (MASTER) Hospital List (updated October 2015) NHS Board Hospital ISD Staffed beds Speciality / Type classification Ayrshire & Arran A&A University Hospital Ayr A2 343 Acute (general with some teaching) University Hospital Crosshouse A2 666 Acute (general with some teaching) Arran War Memorial Hospital A3 19 Acute (mixed speciality) (9) 3 acute Biggart Hospital, Prestwick B6 121 Long stay geriatric & acute 6 community Kirklandside Hospital, Kilmarnock B7 36 Small, long stay geriatric Ayrshire Central Hospital B8 142 Long stay geriatric & acute Davidson Cottage J26 26 Community East Ayrshire Community Hospital, Cumnock J26 57 Community Girvan Community Hospital J26 20 Community Lady Margaret Hospital, Millport J26 9 Community Borders Borders Borders General Hospital A2 265 Acute (general, with some teaching) (5) Hay Lodge Hospital, Peebles J26 23 Community 1 acute Hawick Community Hospital J26 22 Community 4 community Kelso Community Hospital J26 23 Community Knoll Hospital, Duns J26 23 Community Dumfries & Galloway D&G Dumfries & Galloway Royal Infirmary A2 367 Acute (general, with some teaching) Galloway Community Hospital A3 48 Acute (mixed speciality) (10) 2 acute Annan Hospital B7 18 Small, long stay geriatric / rehab 8 community Thornhill Hospital B7 13 Small, long stay geriatric / rehab Thomas Hope Hospital, Langholm B7 10 Small, long stay geriatric / rehab Lochmaben Hospital, Lockerbie B9 17 Long stay geriatric / rehab / psychiatry Castle Douglas Hospital J26 19 Community Kirkcudbright Cottage Hospital J26 9 Community Moffat Hospital J26 12 Community Newton Stewart Hospital J26 19 Community 1 HEI (MASTER) Hospital List (updated October 2015) Fife Fife Victoria Hospital, Kirkcaldy A2 621 Acute (general with some teaching) (7) Queen Margaret Hospital, Dunfermline A3 196 Acute (mixed speciality) 2 acute 5 community Cameron Hospital, Leven B7 95 Small, long stay geriatric Adamson Hospital, Cupar J26 19 Community Glenrothes Hospital J26 74 Community Randolph Wemyss Memorial Hospital J26 16 Community St. -

ED Pub 4Hr 2009-10
NHS Scotland - Emergency Department Activity Attendances and Performance against the 4-hour Waiting Time Standard This is an ISD Scotland National Statistics release. The Scottish Government waiting time standard for emergency departments is that 98 % of all attendances should be seen within 4 hours. The figures presented in these tables detail the performance of each individual site and NHS board against the standard. Time Period: 2009/10 (Apr-09 to Mar-10) Source: A&E data mart, ISD Scotland Date: 04 August 2011 List of Tables Table 1: Attendances and performance against 4-hour standard, 2009/10 Total attendances, number of attendances breaching standard and attendances meeting standard (number and percentage). Figures are given at site and NHS Board level. Table 2: Attendances, 2009/10 Summary table of attendances only. Figures are given at site and NHS Board level. Table 3: Performance against 4-hour standard, 2009/10 Summary table of percentage of attendances meeting standard. Figures are given at site and NHS Board level. Notes: 1) The waiting time is defined as the time of arrival until the time of discharge, admission or transfer. 2) New presentations only; excludes planned return and recall attendances. 3) There are two types of site that provide emergency care; • ED - Emergency Departments; sites that provide a 24 hour emergency medicine consultant led service • MIU/Other - sites including minor injuries units (MIU), small hospitals and health centres in rural areas that carry out emergency department related activity and are GP or Nurse led. They may or may not be open 24 hours. 4) The information presented is based on data under development, the quality and accuracy are being monitored. -
Annual Report & Accounts 2018-19
Grampian Health Board Endowment Fund (Operating as NHS Grampian Endowment Funds) Trustees’ Report and Accounts Year Ended 31 March 2019 Charity Number SC017296 NHS Grampian Endowment Funds Foreword from the Chair In 2018/2019 the Endowment Fund has continued to support the health and welfare of people in Grampian through our grant making, working in partnership with NHS Grampian and other key stakeholders. Financially, this has been a stable year for the Endowment Fund with donations remaining at an encouraging level, although legacies, always less predictable, show a downturn from a very high figure in the previous year. Our return on investment has yielded a positive return which was in line with predictions set at the start of the year. Due to the generosity of our donors and stable investment activity, the Endowment Fund was able to commit almost £4 million in charitable expenditure to activities, services and equipment during 2018/19. Reflecting the population we serve, the Endowment fund grant giving activity was diverse as the following examples illustrate. We supported community groups through the Small Grants Scheme. These have ranged from rehabilitation exercise classes to singing groups to Men’s Sheds. We supported staff training and development. This year this included the purchase of neonatal resuscitation manikins for use at Aberdeen Maternity Hospital and Dr Gray’s and ligature manikins for Royal Cornhill Hospital. We supported the purchase of a range of equipment to improve patient experience. The Lithotripter for urology patients was delivered in January 2019 and is providing the most up to date technology for the treatment for renal stones, replacing a mobile service with a permanent facility at ARI. -

Scotland) 15 June 2021
Version 1.6 (Scotland) 15 June 2021 ISARIC/WHO Clinical Characterisation Protocol UK (Scotland) Recruitment Procedures for FRONTLINE CLINICAL RESEARCH STAFF The most up to date versions of the protocol and case report form are available at isaric4c.net/protocols/ A virtual site visit is available at isaric4c.net/virtual_site_visit/ AIM: Please recruit the following patients only: • Vaccine failure (positive COVID test - rather than displaying symptoms – >28d after having received a vaccine) • Reinfection (proven after proven) • Co-infection (flu/RSV) • COVID associated hyper inflammation (MIS-A/MIS-C/PINS-TS) at any age • Samples from patients with pathogens of public health interest including people identified as infected with SARS-CoV “variants of concern” • All children CONSENT: once the form is signed by a participant it is hazardous. To record consent, we suggest an independent witness observes the completed form then signs a fresh copy outside of the isolation area. Consent can also be obtained by telephone from participants or from relatives for proxy consent. RECRUITMENT PACKS: Sample collection kits will be supplied to sites. Sample collections kits can be requested from: [email protected] Each kit will have a specific kit ID number, with each component within showing this kit ID and its own respective component ID for audit purposes. Pods and bio-bags for shipping will also be supplied to sites. These can be requested from [email protected] OBTAIN SAMPLES according to the schedule. You can find out which tier you are operating at in the front page of the site file. If you have capacity to recruit at TIER 2: Day 1 2 3 4 5 6 7 8 9 28 days after discharge Samples R S S C Sample priority 1 2 3 4 R: recruitment sample; S: serial sample; C: convalescent sample. -

Palliative Care in Community Hospitals in Scotland
PALLIATIVE CARE IN COMMUNITY HOSPITALS IN SCOTLAND A FRAMEWORK FOR GOOD PRACTICE 2003 PALLIATIVE CARE IN COMMUNITY HOSPITALS IN SCOTLAND A FRAMEWORK FOR GOOD PRACTICE 2003 Published by Scottish Association of Community Hospitals and Scottish Partnership for Palliative Care ©2003 Contents Forward 2 Executive Summary 4 Introduction 6 Part 1 Palliative Care What is palliative care? 7 Who delivers palliative care? 8 What is the basis of palliative care? 8 When should palliative care begin? 10 Part 2 Community Hospitals What is a community hospital? 11 Geographical spread of community hospitals 12 The importance of managed clinical networks 14 Community hospitals “out-of-hours” issues 14 Part 3 Palliative Care in Community Hospitals Current provision of palliative care in community hospitals 17 Quality issues 20 Palliative care “out-of-hours” 21 Links with palliative care and other specialist colleagues 21 Needs of patients, relatives & providers 22 Recommendations 24 Conclusion 25 Appendices Appendix A – Stocktake of Current Provision of palliative Care in Community Hospitals in Scotland 26 Appendix B – Definitions of Extended Primary Care Teams and Intermediate Care 64 Appendix C – Regional Breakdown of Identified Needs – Training Facilities 65 PALLIATIVE CARE IN COMMUNITY HOSPITALS IN SCOTLAND Foreword Studies continue to confirm what experienced general patient has a right to expect. Palliative care is more than practitioners have long suspected, namely that people an exercise in prescribing, crucially important as the relief with mortal illness would prefer to die at home, or at of pain and suffering is. Its success depends on more least to be cared for there as long as possible, but than the availability of syringe drivers, nebulisers and red disappointingly few achieve this wish.