Diseases and Disorders of the Gastrointestinal Tract
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Autologous Gluteal Lipograft
Aesth Plast Surg (2011) 35:216–224 DOI 10.1007/s00266-010-9590-y ORIGINAL ARTICLE Autologous Gluteal Lipograft Beatriz Nicareta • Luiz Haroldo Pereira • Aris Sterodimas • Yves Ge´rard Illouz Received: 14 January 2010 / Accepted: 15 July 2010 / Published online: 25 September 2010 Ó Springer Science+Business Media, LLC and International Society of Aesthetic Plastic Surgery 2010 Abstract In the past 25 years, several different tech- expressed the desire of further gluteal augmentation, 16 had niques of lipoinjection have been developed. The authors one more session of gluteal fat grafting. The remaining five performed a prospective study to evaluate the patient sat- patients did not have enough donor area and instead isfaction and the rate of complications after an autologous received gluteal silicone implants. At 12 months, 70% gluteal lipograft among 351 patients during January 2002 reported that their appearance after gluteal fat augmentation and January 2008. All the patients included in the study was ‘‘very good’’ to ‘‘excellent,’’ and 23% responded that requested gluteal augmentation and were candidates for their appearance was ‘‘good.’’ Only 7% of the patients the procedure. Overall satisfaction with body appearance thought their appearance was less than good. At 24 months, after gluteal fat augmentation was rated on a scale of 1 66% reported that their appearance after gluteal fat aug- (poor), 2 (fair), 3 (good), 4 (very good), and 5 (excellent). mentation was ‘‘very good’’ (36%) to ‘‘excellent’’ (30%), The evaluation was made at follow-up times of 12 and and 27% responded that their appearance was ‘‘good.’’ 24 months. The total amount of clean adipose tissue However, 7% of the patients continued to think that their transplanted to the buttocks varied from 100 to 900 ml. -
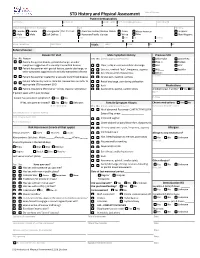
STD History and Physical Assessment Date of Service: Patient Demographics Last Name First Name Middle Initial Pref
STD History and Physical Assessment Date of Service: Patient Demographics Last Name First Name Middle Initial Pref. name/AKA/pronoun Date of Birth Sex (at birth) Gender (all that apply Race Ethnicity Female Female Transgender Pref. Pronoun: American Indian/Alaskan Native Asian African American Hispanic Male Male Self Define: Hawaiian/Pacific Islander White Other Non-Hispanic Street Address City State Zip County Home Telephone Cell Phone Vitals: Temp: Pulse: RR: BP: Referral Source: Reason for Visit Male Symptom History Previous STD Yes No Reason Yes No (check appropriate boxes) Chlamydia Gonorrhea Patient has genital lesions, genital discharge, or other Hep. C Herpes symptoms suggestive of a sexually transmitted disease Clear, milky or mucoid urethral discharge HIV HPV Patient has partner with genital lesions, genital discharge, or Dysuria , urethral “itch”, frequency, urgency PID Syphilis other symptoms suggestive of a sexually transmitted disease Sore throat and/or hoarseness Other: Patient has partner treated for a sexually transmitted disease Scrotal pain, swelling, redness Comments: Patient referred by local or state DIS. Review labs and refer to Rectal discharge, pain during defecation appropriate STD treatment SDO Rash Medications Patient requesting STD testing – denies reasons listed above Asymmetric, painful, swollen joints Antibiotics last 4 weeks? Yes No If patient seen within past 30 days: Name Purpose Patient has persistent symptoms? Yes No If Yes, was partner treated? Yes No Unknown Female Symptom History Chronic medications -

The Abdominal Wall the Digestive Tract the Pancreas the Biliary
The abstracts which follow have been classified for the convenience of the reader under the following headings: Experimental Studies; Animal Tumors The Abdominal Wall The Cancer Cell The Digestive Tract General Clinical and Laboratory Observa- The Pancreas tions The Biliary Tract Diagnosis and Treatment Peritoneal, Retroperitoneal. and Mesenteric The Skin Tumors The Eye The Spleen The Ear The Female Genital Tract The Breast The Genito-Urinary Tract The Oral Cavity and Upper Respiratory The Nervous System Tract The Bones and Joints The Salivary Glands The Leukemias, Hodgkin's Disease, Lympho The Thyroid Gland sarcoma Intrathoracic Tumors As with any such scheme of classification, overlapping has been unavoidable. Shall an article on II Cutaneous Melanoma, an Histological Study" be grouped with the articles on Histology or with the Skin Tumors? Shall Traumatic Cerebral Tumors go under Trauma or The Nervous System? The reader's choice is likely to depend upon his personal interests; an editor may be governed by no such considerations. The attempt has been made, there fore, to put such articles in the group where they would seem most likely to be sought by the greatest number. It is hoped that this aim has not been entirely missed. As abstractors are never perfect, and as the opinions expressed may on occasion seem to an author not to represent adequately his position, opportunity is offered any such to submit his own views for publication. The JOURNAL will not only welcome correspondence of this nature but hopes in the future to have a large number of author abstracts, so that the writer of a paper may present his subject in his own way. -

Volume Rejuvenation of the Lower Third, Perioral, and Jawline
70 Volume Rejuvenation of the Lower Third, Perioral, and Jawline Edward D. Buckingham, MD1 Robert Glasgold, MD2 Theda Kontis, MD3 StephenP.Smith,Jr.,MD4 Yalon Dolev, MDCM, FRCS(c)5 Rebecca Fitzgerald, MD6 Samuel M. Lam, MD, FACS7 Edwin F. Williams, MD8 Taylor R. Pollei, MD8 1 Director, Buckingham Center for Facial Plastic Surgery, Austin, Texas Address for correspondence Edward D. Buckingham, MD, 2 Department of Surgery, Rutgers University-Robert Wood Johnson Department of Facial Plastic Surgery, Buckingham Center for Facial Medical School, Piscataway, New Jersey Plastic Surgery, 2745 Bee Caves Road #101, Austin, TX 78746 3 Department of Facial Plastic Surgery, Johns Hopkins Medical (e-mail: [email protected]). Institutions, Facial Plastic Surgicenter, LLC, Baltimore, Maryland 4 Department of Otolaryngology, The Ohio State University, Columbus, Ohio 5 Department of Facial Plastic and Reconstructive Surgery, ENT SpecialtyGroup,Westmount,Canada 6 Department of Dermatology, David Geffen School of Medicine, University of California Los Angeles, Los Angeles, California 7 Willow Bend Wellness Center, Plano, Texas 8 Williams Center for Excellence, Latham, New York Facial Plast Surg 2015;31:70–79. Abstract This is the third and final article discussing volumetric rejuvenation of the face. The previous two articles, Rejuvenation of the Upper Third and Management of the Middle Third, focused on the upper two-thirds of the face while this article focuses on the lower Keywords face, including the marionette area, jawline, and neck. Again, the authors of the ► facial rejuvenation previous two articles have provided a summary of rejuvenation utilizing a product of ► volume replacement which they are considered an expert. -

Clinical Practice Guideline for the Management of Anorectal Abscess, Fistula-In-Ano, and Rectovaginal Fistula Jon D
PRACTICE GUIDELINES Clinical Practice Guideline for the Management of Anorectal Abscess, Fistula-in-Ano, and Rectovaginal Fistula Jon D. Vogel, M.D. • Eric K. Johnson, M.D. • Arden M. Morris, M.D. • Ian M. Paquette, M.D. Theodore J. Saclarides, M.D. • Daniel L. Feingold, M.D. • Scott R. Steele, M.D. Prepared on behalf of The Clinical Practice Guidelines Committee of the American Society of Colon and Rectal Surgeons he American Society of Colon and Rectal Sur- and submucosal locations.7–11 Anorectal abscess occurs geons is dedicated to ensuring high-quality pa- more often in males than females, and may occur at any Ttient care by advancing the science, prevention, age, with peak incidence among 20 to 40 year olds.4,8–12 and management of disorders and diseases of the co- In general, the abscess is treated with prompt incision lon, rectum, and anus. The Clinical Practice Guide- and drainage.4,6,10,13 lines Committee is charged with leading international Fistula-in-ano is a tract that connects the perine- efforts in defining quality care for conditions related al skin to the anal canal. In patients with an anorec- to the colon, rectum, and anus by developing clinical tal abscess, 30% to 70% present with a concomitant practice guidelines based on the best available evidence. fistula-in-ano, and, in those who do not, one-third will These guidelines are inclusive, not prescriptive, and are be diagnosed with a fistula in the months to years after intended for the use of all practitioners, health care abscess drainage.2,5,8–10,13–16 Although a perianal abscess workers, and patients who desire information about the is defined by the anatomic space in which it forms, a management of the conditions addressed by the topics fistula-in-ano is classified in terms of its relationship to covered in these guidelines. -

FDA Executive Summary General Issues Panel Meeting on Dermal Fillers
FDA Executive Summary General Issues Panel Meeting on Dermal Fillers Prepared for the Meeting of the General and Plastic Surgery Devices Advisory Panel March 23, 2021 1 Table of Contents Table of Contents ............................................................................................................................ 2 List of Tables .................................................................................................................................. 3 List of Figures ................................................................................................................................. 4 List of Acronyms ............................................................................................................................ 5 Executive Summary ........................................................................................................................ 6 I. Purpose of Meeting ............................................................................................................. 6 II. Structure of the Meeting ..................................................................................................... 6 III. Introduction ......................................................................................................................... 6 IV. Device Description .............................................................................................................. 8 Pre-clinical Evaluation ..................................................................................................... -

Noonan Syndrome with Plastic Bronchitis in an Adult
Kumar V, et al., J Pulm Med Respir Res 2021 7: 058 DOI: 10.24966/PMRR-0177/100058 HSOA Journal of Pulmonary Medicine and Respiratory Research Case Report having variable expression. Missense mutation in gene PTPN11 (on chromosome 12q24) accounts for half of cases of Noonan syndrome Noonan Syndrome with Plastic [3]. Predominance of maternal transmission is noted in familial cases. Bronchitis in an Adult This has been thought to be due to infertility in affected males which may be related to cryptorchidism. For this mild/subtle phenotype needs to be searched in parent of affected person. The incidence of Vikas Kumar1, Avinash Goswami2, Shweta Anand1, Dharam Dev Golani2, Mahak Golani3, Sandeep Sahu2, Abhishek Faye1, Plastic bronchitis is not well defined. Various lymphatic abnormalities Subhadeep Saha1, Arunachalam Meenakshisundaram1, Karnail have been observed in the patients of Noonan syndrome including Singh1 and Rupak Singla1* pulmonary and intestinal lymphangiectasia and lymphoedema [4]. Due to the lymphangitic abnormalities, plastic bronchitis may happen 1 Department of Tuberculosis and Respiratory Diseases, National Institute of in these patients [5]. Few paediatric cases were reported of Noonan TB and Respiratory Diseases, New Delhi, India syndrome with plastic bronchitis in the past. They were also having 2Department of Medicine, Deen Dayal Upadhyay Hospital, New Delhi, India cardiovascular abnormalities requiring Fontan operation [6,7]. We 3Department of Tuberculosis and Respiratory Diseases, Lady Hardinge are reporting first case of Noonan syndrome in an adult patient who Medical College, New Delhi, India presented to us with plastic bronchitis without any cardiovascular abnormality. Case Report Abstract A 36-year-old male, teacher, non-smoker, came to the hospital, Noonan syndrome is an autosomal dominant disease with low with the complaints of progressive shortness of breath and cough incidence. -

Clinical Characteristics and Incidence of Perianal Diseases in Patients with Ulcerative Colitis
Annals of Original Article Coloproctology Ann Coloproctol 2018;34(3):138-143 pISSN 2287-9714 eISSN 2287-9722 https://doi.org/10.3393/ac.2017.06.08 www.coloproctol.org Clinical Characteristics and Incidence of Perianal Diseases in Patients With Ulcerative Colitis Yong Sung Choi1, Do Sun Kim2, Doo Han Lee2, Jae Bum Lee2, Eun Jung Lee2, Seong Dae Lee2, Kee Ho Song2, Hyung Joong Jung2 Departments of 1Gastroenterology and 2Surgery, Daehang Hospital, Seoul, Korea Purpose: While perianal disease (PAD) is a characteristic of patients with Crohn disease, it has been overlooked in pa- tients with ulcerative colitis (UC). Thus, our study aimed to analyze the incidence and the clinical features of PAD in pa- tients with UC. Methods: We reviewed the data on 944 patients with an initial diagnosis of UC from October 2003 to October 2015. PAD was categorized as hemorrhoids, anal fissures, abscesses, and fistulae after anoscopic examination by experienced proctol- ogists. Data on patients’ demographics, incidence and types of PAD, medications, surgical therapies, and clinical course were analyzed. Results: The median follow-up period was 58 months (range, 12–142 months). Of the 944 UC patients, the cumulative in- cidence rates of PAD were 8.1% and 16.0% at 5 and 10 years, respectively. The incidence rates of bleeding hemorrhoids, anal fissures, abscesses, and fistulae at 10 years were 6.7%, 5.3%, 2.6%, and 3.4%, respectively. The cumulative incidence rates of perianal sepsis (abscess or fistula) were 2.2% and 4.5% at 5 and 10 years, respectively. In the multivariate analyses, male sex (risk ratio [RR], 4.6; 95% confidence interval [CI], 1.7–12.5) and extensive disease (RR, 4.2; 95% CI, 1.6–10.9) were significantly associated with the development of perianal sepsis. -

Perianal Abscess in a 2-Year-Old Presenting with a Febrile Seizure and Swelling of the Perineum Gregory M
Oxford Medical Case Reports, 2019;01, 26–28 doi: 10.1093/omcr/omy116 Case Report CASE REPORT Perianal abscess in a 2-year-old presenting with a febrile seizure and swelling of the perineum Gregory M. Taylor, DO* and Andrew H. Erlich, DO Emergency Medicine Physician, Beaumont Hospital, Teaching Hospital of Michigan State University, Department of Emergency Medicine, Farmington Hills, MI, USA *Correspondence address. Beaumont Hospital, Teaching Hospital of Michigan State University, Farmington Hills, MI, USA. E-mail: Gregory.Taylor@ Beaumont.org Abstract An anorectal abscess, specifically a perianal abscess, is a relatively uncommon infection in children. It is a purulent fluid collection under the soft tissue outside the anus. Some of these abscesses may spontaneously drain and heal by themselves, while others may result in sepsis and require surgical intervention. The transition to a systemic illness requiring hospital admission is considered rare. We present the case of a 2-year-old male presenting with a febrile seizure and found to be systemically ill secondary to a perianal abscess. To our knowledge, this is the first case reported in the literature of a febrile seizure secondary to a perianal abscess. INTRODUCTION Vitals on arrival to the ED were as follows: 103.1°F, blood pressure of 96/78 mmHg, respiratory rate 27 breaths/min, heart A perianal abscess occurs most often in male children <1 year rate 126 beats/min, weight 12.8 kg and 100% oxygen saturation of age; however, they can occur at any age and in either sex [1]. on room air. As soon as he was brought back to the treatment In one study, an incidence was reported of up to 4.3% [1]. -

SMAS Nasolabial Fold
ORIGINAL ARTICLE Analysis of the effects of subcutaneous musculoaponeurotic system facial support on the nasolabial crease Michael J Sundine MD FACS FAAP, Bruce F Connell MD MJ Sundine, BF Connell. Analysis of the effects of subcutaneous Analyse des effets du support du système musculoaponeurotic system facial support on the nasolabial crease. Can J Plast Surg 2010;18(1):11-14. musculo-aponévrotique sous-cutané facial sur le pli nasogénien The idea that traction on the subcutaneous musculoaponeurotic system (SMAS) deepens the nasolabial crease has been propagated through the La notion selon laquelle une traction exercée sur le système musculo- plastic surgery literature. This notion is contrary to the senior author’s aponévrotique sous-cutané approfondit le pli nasogénien s’est propagée experience. The purpose of the present study was to investigate the effects dans la littérature en chirurgie plastique. Or, cette notion ne concorde pas of mobilization of the SMAS on the nasolabial fold and crease. avec les observations de l’auteur principal. Le but de la présente étude était Intraoperative examination on the effect of traction on the SMAS was d’évaluer les effets d’une mobilisation du système musculo-aponévrotique performed. Ten consecutive primary facelift patients underwent facelift sous-cutané sur le pli et le sillon nasogéniens. L’auteur a procédé à un procedures with SMAS support. Following mobilization of the SMAS, examen peropératoire de l’effet de la traction sur le système. Dix patients traction was placed on the SMAS without traction on the skin. In all cases, consécutifs soumis à un redrapage facial primaire on subit l’intervention the nasolabial fold was effaced and the nasolabial crease did not deepen. -

Sexually Transmitted Diseases Treatment Guidelines, 2015
Morbidity and Mortality Weekly Report Recommendations and Reports / Vol. 64 / No. 3 June 5, 2015 Sexually Transmitted Diseases Treatment Guidelines, 2015 U.S. Department of Health and Human Services Centers for Disease Control and Prevention Recommendations and Reports CONTENTS CONTENTS (Continued) Introduction ............................................................................................................1 Gonococcal Infections ...................................................................................... 60 Methods ....................................................................................................................1 Diseases Characterized by Vaginal Discharge .......................................... 69 Clinical Prevention Guidance ............................................................................2 Bacterial Vaginosis .......................................................................................... 69 Special Populations ..............................................................................................9 Trichomoniasis ................................................................................................. 72 Emerging Issues .................................................................................................. 17 Vulvovaginal Candidiasis ............................................................................. 75 Hepatitis C ......................................................................................................... 17 Pelvic Inflammatory -

ESMO Colorectal Cancer Guide for Patients English
Colorectal Cancer What is colorectal cancer? Let us explain it to you. www.anticancerfund.org www.esmo.org ESMO/ACF Patient Guide Series based on the ESMO Clinical Practice Guidelines COLORECTAL CANCER: A GUIDE FOR PATIENTS PATIENT INFORMATION BASED ON ESMO CLINICAL PRACTICE GUIDELINES This guide for patients has been prepared by the Anticancer Fund as a service to patients, to help patients and their relatives better understand the nature of colorectal cancer and appreciate the best treatment choices available according to the subtype of colorectal cancer. We recommend that patients ask their doctors about what tests or types of treatments are needed for their type and stage of disease. The medical information described in this document is based on the clinical practice guidelines of the European Society for Medical Oncology (ESMO) for the management of colorectal cancer. This guide for patients has been produced in collaboration with ESMO and is disseminated with the permission of ESMO. It has been written by a medical doctor and reviewed by two oncologists from ESMO including the leading author of the clinical practice guidelines for professionals. It has also been reviewed by patient representatives from ESMO’s Cancer Patient Working Group. More information about the Anticancer Fund: www.anticancerfund.org More information about the European Society for Medical Oncology: www.esmo.org For words marked with an asterisk, a definition is provided at the end of the document. Colorectal Cancer: a guide for patients - Information based on ESMO Clinical Practice Guidelines - v.2016.1 Page 1 This document is provided by the Anticancer Fund with the permission of ESMO.