Lima, Bogotá, June 21St, 2021 Secretariat of the Committee
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Gawc Link Classification FINAL.Xlsx
High Barcelona Beijing Sufficiency Abu Dhabi Singapore sufficiency Boston Sao Paulo Barcelona Moscow Istanbul Toronto Barcelona Tokyo Kuala Lumpur Los Angeles Beijing Taiyuan Lisbon Madrid Buenos Aires Taipei Melbourne Sao Paulo Cairo Paris Moscow San Francisco Calgary Hong Kong Nairobi New York Doha Sydney Santiago Tokyo Dublin Zurich Tokyo Vienna Frankfurt Lisbon Amsterdam Jakarta Guangzhou Milan Dallas Los Angeles Hanoi Singapore Denver New York Houston Moscow Dubai Prague Manila Moscow Hong Kong Vancouver Manila Mumbai Lisbon Milan Bangalore Tokyo Manila Tokyo Bangkok Istanbul Melbourne Mexico City Barcelona Buenos Aires Delhi Toronto Boston Mexico City Riyadh Tokyo Boston Munich Stockholm Tokyo Buenos Aires Lisbon Beijing Nanjing Frankfurt Guangzhou Beijing Santiago Kuala Lumpur Vienna Buenos Aires Toronto Lisbon Warsaw Dubai Houston London Port Louis Dubai Lisbon Madrid Prague Hong Kong Perth Manila Toronto Madrid Taipei Montreal Sao Paulo Montreal Tokyo Montreal Zurich Moscow Delhi New York Tunis Bangkok Frankfurt Rome Sao Paulo Bangkok Mumbai Santiago Zurich Barcelona Dubai Bangkok Delhi Beijing Qingdao Bangkok Warsaw Brussels Washington (DC) Cairo Sydney Dubai Guangzhou Chicago Prague Dubai Hamburg Dallas Dubai Dubai Montreal Frankfurt Rome Dublin Milan Istanbul Melbourne Johannesburg Mexico City Kuala Lumpur San Francisco Johannesburg Sao Paulo Luxembourg Madrid Karachi New York Mexico City Prague Kuwait City London Bangkok Guangzhou London Seattle Beijing Lima Luxembourg Shanghai Beijing Vancouver Madrid Melbourne Buenos Aires -
IN-Between Metropolitan Strategies Programme Interview #8 | Lima, Peru 8
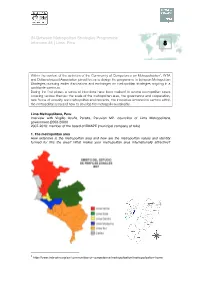
IN-Between Metropolitan Strategies Programme Interview #8 | Lima, Peru 8 Within the context of the activities of the Community of Competence on Metropolisation1, INTA and Deltametropool Association joined forces to design the programme In-between Metropolitan Strategies pursuing earlier discussions and exchanges on metropolitan strategies ongoing in a worldwide spectrum. During the first phase, a series of interviews have been realised to several metropolitan cases covering various themes: the scale of the metropolitan area, the governance and cooperation, new forms of urbanity and metropolitan environments, the innovative economical sectors within the metropolitan area and how to develop the metropolis sustainably. Lima Metropolitana, Peru Interview with Virgilio Acuña Peralta, Peruvian MP, councillor of Lima Metropolitana government (2003-2006) 2007-2010: member of the board of EMAPE (municipal company of tolls) 1.! The metropolitan area How extensive is the metropolitan area and how are the metropolitan values and identity formed for this the area? What makes your metropolitan area internationally attractive? 1 http://www.inta-aivn.org/en/communities-of-competence/metropolisation/metropolisation-home In Between Metropolitan Strategies Programme – Interview 7 Lima Metropolitana counts 9 millions inhabitants (including the Province of Callao) and 42 districts. The administrative region of Lima Metropolitana (excluding Callao) has a total surface of 2800 km2. The metropolitan area has an extension of 150km North-South and 60Km on the West (sea coast) - East (toward the Andes) direction. The development of the city with urban sprawl goes south, towards the seaside resorts, outside of the administrative limits of Lima Metropolitana (Province of Cañete, City of Ica) and to the Northern beach areas. -
Accountability Toolkit. U.N. Standards on Sexual And
accountABILITY: U.N. Standards on Sexual and Reproductive Health and Rights of Women and Girls with Disabilities © 2017 Women Enabled International Printed in the United States Cover image depicts three women in silhouette—one using a forearm crutch, one using a wheelchair, and one without any mobility aids—approaching a United Nations building in Geneva through a corridor of flags from countries around the world. Photo credit: “The “Allée des drapeaux” ("Flags Way") at the Palais des Nations, seat of the UN Office at Geneva (UNOG).” Photographer: Jean-Marc Ferré. Copyright © United Nations 2015. Any part of this publication may be copied, translated, or adapted with permission from the authors, provided that the parts copied are distributed free or at cost (not for profit) and Women Enabled International is acknowledged as the author. Any commercial reproduction requires prior written permission from the authors. Women Enabled International would appreciate receiving a copy of any materials in which information from this publication is used. Women Enabled International 1875 Connecticut Ave., NW, 10th Floor Washington, D.C. 20009 United States Tel. 1.202.630.3818 [email protected] www.womenenabled.org Contents Acknowledgments ..................................................................................................................... ii Using this Briefing Paper .......................................................................................................... 1 Sexual and Reproductive Health and Rights of Women and -

Spanish Impact on Peru (1520 - 1824)
Spanish Impact on Peru (1520 - 1824) San Francisco Cathedral (Lima) Michelle Selvans Setting the stage in Peru • Vast Incan empire • 1520 - 30: epidemics halved population (reduced population by 80% in 1500s) • Incan emperor and heir died of measles • 5-year civil war Setting the stage in Spain • Iberian peninsula recently united after 700 years of fighting • Moors and Jews expelled • Religious zeal a driving social force • Highly developed military infrastructure 1532 - 1548, Spanish takeover of Incan empire • Lima established • Civil war between ruling Spaniards • 500 positions of governance given to Spaniards, as encomiendas 1532 - 1548, Spanish takeover of Incan empire • Silver mining began, with forced labor • Taki Onqoy resistance (‘dancing sickness’) • Spaniards pushed linguistic unification (Quechua) 1550 - 1650, shift to extraction of mineral wealth • Silver and mercury mines • Reducciones used to force conversion to Christianity, control labor • Monetary economy, requiring labor from ‘free wage’ workers 1550 - 1650, shift to extraction of mineral wealth • Haciendas more common: Spanish and Creole owned land, worked by Andean people • Remnants of subsistence-based indigenous communities • Corregidores and curacas as go- betweens Patron saints established • Arequipa, 1600: Ubinas volcano erupted, therefor St. Gerano • Arequipa, 1687: earthquake, so St. Martha • Cusco, 1650: earthquake, crucifix survived, so El Senor de los Temblores • Lima, 1651: earthquake, crucifixion scene survived, so El Senor de los Milagros By 1700s, shift -

FGV Direito Rio in Rio De Janeiro, Brazil
FGV Direito Rio in Rio de Janeiro, Brazil FGV Direito Rio is one of the most well respected education institutions in one of the most exciting international cities in the world. There are more than 3,000 undergraduate students and almost 2,000 graduate and master’s students enrolled. During the 2019-20 academic year, no U of M Law students participated in the semester exchange. Summary of Course Offerings http://direitorio.fgv.br/graduacao/gradecurricular Semester Dates Fall semester: August through December 2020 Spring semester: February to July 2021 Language of instruction Portuguese; four to six courses are offered in English each semester Courses/Credits/Grades Up to 15 credits may be transferred per semester abroad Each class period is 100 minutes; each course has either 30 or 60 “course hours” Grading is from 0 (minimum) to 10 (maximum) with a passing grade being 7 2 ECTS Credits = 1 Minnesota Credit Registration Registration is done by the International Office prior to the student’s arrival. Participate in our Law School’s lottery for the term you will be away. Register for 12-15 credits. Before leaving for your semester abroad, contact the Law School registrar at [email protected] to convert your credits to Off-campus Legal Studies. Housing FGV Direito Rio does not have on-campus housing for international students. They will provide assistance once students arrive in locating and obtaining off-campus accommodations. Financial Aid and Tuition Payment Financial aid will remain in effect for the semester you are abroad. Please make arrangements to have the balance (after tuition is deducted) sent to you if disbursement occurs after you have departed the U.S. -

Buenos Aires to Lima By
FH {SR--27 The Bolivar Hotel Lima, Peru August 31, 1942 Dear hr. <oer s It is surprising how simple and relatively unexciting it seems to fly. Saturday, August 22, I climbed aboard a seven-ton, two-motored anagra plane and took off for the first time in my.life on the first lap of a 6,000 mile air journey--Buenos Aires to iiami. We were off and away without a bump. In a few minutes we were roaring high above the pampa. There is no reason to get poetic about a bird's eye view of the rGentine plains. For two and a half hours, at seven thousand feet, we moved over the flat gra. in belt. I amused myself by looking at the edge of the ing and watching one field after another come into view. That way one 5or the feeling of mo- tion.. any of the fields, I knew, were as large as five hundred or a thousand acres. One could count the chacras below. Every primitive bin or two meant a chacra. One could look right down upon th yel'low ,aize in thcorntrojes, uncovered and unpro- tected from the elements. Estancias were umistakable too, for stately groves of trees numbered them. Trees stood out best of all. In two hours flyin time the .green of the green fields bec-ame lighter, ore delicate, and I kno: that C6rdoba could not be very far away. Surely enoush, 6rdoba came into view, restin in a natural de- pression at the foot of the sierras and at the edge of the pampa. -

DEADLY DELAYS Maternal Mortality in Peru a Rights-Based Approach to Safe Motherhood
DEADLY DELAYS Maternal Mortality in Peru A Rights-Based Approach to Safe Motherhood A Report by Physicians for Human Rights ©2007 Physicians for Human Rights All rights reserved. Printed in the United States of America ISBN: 1-879707-54-3 Library of Congress Control Number: 2007939731 Cover Photo: Christopher Drake Design: Glenn Ruga/Visual Communications, www.vizcom.org Physicians for huMan rights hysicians for Human Rights (PHR) mobilizes health As one of the original steering committee members professionals to advance the health and dignity of of the International Campaign to Ban Landmines, PHR Pall people through action that promotes respect shared the 1997 Nobel Peace Prize. for, protection of, and the fulfillment of human rights. Since 1986, PHR members have worked to stop torture, Physicians for Human Rights disappearances, and political killings by governments 2 Arrow Street, Suite 301 and opposition groups and to investigate and expose Cambridge, MA 02138 violations, including deaths, injuries, and trauma inflicted Tel. (617) 301.4200 on civilians during conflicts; suffering and deprivation, Fax. (617) 301.4250 including denial of access to healthcare caused by ethnic www.physiciansforhumanrights.org and racial discrimination; mental and physical anguish inflicted on women by abuse; exploitation of children Physicians for Human Rights in labor practices; loss of life or limb from landmines 1156 15th Street, NW, Suite 1001 and other indiscriminate weapons; harsh methods of Washington, DC 20005 incarceration in prisons and detention centers, and poor Tel. (202) 728.5335 health stemming from vast inequalities in societies. PHR Fax. (202) 728.3053 has undertaken significant work on health systems and www.physiciansforhumanrights.org on healthcare workforce issues in particular. -

Fall 2010 Pathways.Pdf
pathfinder pioneer advocacy news friends of pathfinder 14 6 2 e 5 . Gifts That Provide ofit ostag on, MA P D Miguel Gutiérrez Dear Pathfinders, Cheryl Tomchin I ermit No A Non-pr U.S. P Bost P Income to You for Life and Help Change Pathfinder’s Peru Beyond Peru, Dr. Gutiérrez has Ten years ago, world leaders gathered to make a historic promise at the United Nations Millennium Summit: The Tomchin Family drawn to Pathfinder’s work when been a strong voice for reproductive to achieve the Millennium Development Goals by 2015. While important progress has been made, the world she learned it was one of the only the Lives of Those Country Representative, rights in Latin America. The region is still not on track to fulfill its promises, most notably in one major area: improving maternal health. Why? Charitable Foundation organizations in India that delivers Dr. Miguel Gutiérrez, has high rates of unsafe abortion— In part, because our leaders are not willing to address politically sensitive topics such as abortion. made their first gift comprehensive reproductive Served by Pathfinder around 94 percent of all abortions health services for women includ- has long been an are unsafe—resulting in injury to Pathfinder in 2006 ing contraception, prenatal care, We know that unsafe abortion is one of the leading causes of maternal death. According to the WHO, nearly one-fifth, A Publication of Pathfinder International Fall 2010 and death of countless women. safe delivery, and safe abortion. advocate for safe abortion or roughly 78,000 maternal deaths annually, are the direct result of complications from unsafe abortion. -

El Ermitaño and Pampa De Cueva As Case Studies for a Regional Urbanization Strategy
Article Place-Making through the Creation of Common Spaces in Lima’s Self-Built Settlements: El Ermitaño and Pampa de Cueva as Case Studies for a Regional Urbanization Strategy Samar Almaaroufi 1, Kathrin Golda-Pongratz 1,2,* , Franco Jauregui-Fung 1 , Sara Pereira 1, Natalia Pulido-Castro 1 and Jeffrey Kenworthy 1,3,* 1 Department of Architecture, Civil Engineering and Geomatics, Frankfurt University of Applied Sciences, 60318 Frankfurt, Germany; samarmaaroufi@gmail.com (S.A.); [email protected] (F.J.-F.); [email protected] (S.P.); [email protected] (N.P.-C.) 2 UIC School of Architecture, Universitat Internacional de Catalunya, 08017 Barcelona, Spain 3 Curtin University Sustainability Policy Institute, Curtin University, Bentley 6102, Australia * Correspondence: [email protected] (K.G.-P.); jeff[email protected] (J.K.) Received: 30 October 2019; Accepted: 2 December 2019; Published: 10 December 2019 Abstract: Lima has become the first Peruvian megacity with more than 10 million people, resulting from the migration waves from the countryside throughout the 20th century, which have also contributed to the diverse ethnic background of today’s city. The paper analyzes two neighborhoods located in the inter-district area of Northern Lima: Pampa de Cueva and El Ermitaño as paradigmatic cases of the city’s expansion through non-formal settlements during the 1960s. They represent a relevant case study because of their complex urbanization process, the presence of pre-Hispanic heritage, their location in vulnerable hillside areas in the fringe with a protected natural landscape, and their potential for sustainable local economic development. The article traces back the consolidation process of these self-built neighborhoods or barriadas within the context of Northern Lima as a new centrality for the metropolitan area. -

December 2017
Immigrant Visa Issuances By Post December 2017 (FY 2018) Post Visa Class Issuances Abidjan CR1 5 Abidjan DV1 9 Abidjan DV2 3 Abidjan DV3 2 Abidjan F11 1 Abidjan F12 1 Abidjan F21 1 Abidjan F22 2 Abidjan F23 1 Abidjan F41 1 Abidjan F42 1 Abidjan F43 2 Abidjan FX1 3 Abidjan FX2 1 Abidjan IR2 6 Abidjan IR5 5 Abu Dhabi CR1 6 Abu Dhabi CR2 3 Abu Dhabi DV1 12 Abu Dhabi DV2 4 Abu Dhabi DV3 5 Abu Dhabi E11 1 Abu Dhabi E14 1 Abu Dhabi E15 1 Abu Dhabi E21 3 Abu Dhabi E31 10 Abu Dhabi E34 7 Abu Dhabi E35 7 Abu Dhabi F11 1 Abu Dhabi F21 2 Abu Dhabi F24 1 Abu Dhabi F33 5 Abu Dhabi F41 6 Abu Dhabi F42 4 Abu Dhabi F43 5 Abu Dhabi FX1 3 Abu Dhabi I51 15 Abu Dhabi I52 13 Abu Dhabi I53 23 Abu Dhabi IR1 4 Abu Dhabi IR2 4 Abu Dhabi IR5 7 Page 1 of 57 Immigrant Visa Issuances By Post December 2017 (FY 2018) Post Visa Class Issuances Accra CR1 45 Accra CR2 1 Accra DV1 24 Accra DV2 9 Accra DV3 14 Accra E31 1 Accra E34 1 Accra F11 19 Accra F12 9 Accra F21 22 Accra F22 20 Accra F23 3 Accra F24 2 Accra F31 6 Accra F32 6 Accra F33 10 Accra F41 11 Accra F42 7 Accra F43 7 Accra FX1 10 Accra FX2 15 Accra FX3 9 Accra IB3 1 Accra IR1 76 Accra IR2 101 Accra IR3 4 Accra IR5 79 Addis Ababa CR1 52 Addis Ababa DV1 109 Addis Ababa DV2 23 Addis Ababa DV3 24 Addis Ababa E11 2 Addis Ababa E14 2 Addis Ababa E15 4 Addis Ababa F11 10 Addis Ababa F12 1 Addis Ababa F21 27 Addis Ababa F22 25 Addis Ababa F24 10 Addis Ababa F25 1 Addis Ababa F41 3 Addis Ababa F42 2 Page 2 of 57 Immigrant Visa Issuances By Post December 2017 (FY 2018) Post Visa Class Issuances Addis Ababa F43 5 Addis -

Strengthening the Protection of Sexual and Reproductive Health and Rights in the African Region Through Human Rights
Strengthening the protection of sexual and reproductive health and rights in the African region through human rights Editors Charles Ngwena Professor of Law, Centre for Human Rights, University of Pretoria Ebenezer Durojaye Associate Professor of Law, University of the Western Cape 2014 Strengthening the protection of sexual and reproductive health and rights in the African region through human rights Published by: Pretoria University Law Press (PULP) The Pretoria University Law Press (PULP) is a publisher at the Faculty of Law, University of Pretoria, South Africa. PULP endeavours to publish and make available innovative, high-quality scholarly texts on law in Africa. PULP also publishes a series of collections of legal documents related to public law in Africa, as well as text books from African countries other than South Africa. This book was peer reviewed prior to publication. For more information on PULP, see www.pulp.up.ac.za Printed and bound by: BusinessPrint, Pretoria To order, contact: PULP Faculty of Law University of Pretoria South Africa 0002 Tel: +27 12 420 4948 Fax: +27 12 362 5125 [email protected] www.pulp.up.ac.za Cover: Yolanda Booyzen, Centre for Human Rights ISBN: 978-1-920538-31-6 © 2014 TABLE OF CONTENTS Acknowledgments v Foreword: Commissioner Soyata Maiga viii (Special Rapporteur on the Rights of Women in Africa) INTRODUCTION Strengthening the protection of sexual and reproductive 1 1 health and rights in the African region through human rights: An introduction Charles Ngwena and Ebenezer Durojaye PART I: REPRODUCTIVE -

Global Rescue Will Evacuate You to Your Home Hospital of Choice
Mumbai. Qogir. Shanghai. Karachi. Istanbul. Delhi. São Paulo. Moscow. Medical Evacuation. Seoul. Beijing. Mount Everest. Mexico City. Tokyo. Ja- karta. New York City. Lagos. Kinshasa. Nepal. Tehran. London. Manaslu. Security Evacuation. Lima. Bogotá. Hong Kong. Bangkok . Makalu. Cairo. Dhaka. Ho Chi Minh City. Annapurna. Rio de Janeiro. Tianjin. Chongqing. Baghdad. Lhotse. Bangalore.Kolkata. Yangon. Santiago. Pakistan. Singapore. Guangzhou. Nanga Parbat. Saint Petersburg. Wuhan. Chennai. Medical Evacuation. Riyadh. Alexandria. Surat. Hyderabad. Shenyang. Ahmedabad. Ankara. Field Rescue. Cho Oyu. Johannesburg. Los Angeles. Kangchenjunga. Abidjan. Yokohama. Busan. Cape Town. Durban. Berlin. Pune. Pyongyang. Madrid. Kanpur. Jaipur. Field Rescue. Buenos Aires. Dhaulagiri. Nairobi. Jeddah. Mumbai. Qogir. Shanghai. Security Evacuation. Karachi. Istanbul. Delhi. São Paulo. Moscow. Seoul. Beijing. Mount Everest. Mexico City. Tokyo. Jakarta. New York City. Lagos. Kinshasa. Nepal. Tehran. London. Manaslu. Lima. Bogotá. Hong Kong. Bangkok Makalu. Cairo. Dhaka. Ho Chi Minh City. Annapurna. Rio de Janeiro. Tianjin. Chongqing. Baghdad. Lhotse. Bangalore. Field Rescue. Kolkata. Yangon. Santiago. Pakistan. Singapore. Guangzhou. Nanga Parbat. Security Evacuation. Saint Petersburg. Wuhan. Medical Evacuation. Chennai. Riyadh. Alexandria. Surat. Hyderabad. Shenyang. Ahmedabad. Ankara. Cho Oyu. Johannesburg. Los Angeles. Kangchenjunga. Abidjan. Yokohama. Busan. Cape Town. Durban. Berlin. Pune. Pyongyang. Madrid. Kanpur. Jaipur. Buenos Aires. Dhaulagiri. Nairobi.Global Jeddah. Mumbai. Qogir. Shanghai. Rescue Karachi. Istanbul. Delhi. São Paulo. Moscow. Medical Evacuation. Seoul. Beijing. Mount Everest. Mexico City. Tokyo. Jakarta. New York City. Lagos. Kinshasa. Nepal. Tehran. London. Manaslu. Security Evacuation. Lima. Bogotá. Hong CriticalKong. Bangkok . ServicesMakalu. Cairo. Dhaka.Provided Ho Chi Minh to City. Stratfor Annapurna. Rio deEnterprises, Janeiro. Tianjin. Chongqing. LLC Baghdad. Lhotse. Bangalore.Kolkata. Yangon. Santiago. Pakistan. Singapore. Guangzhou.