Phartnacotherapy of Peptic Ulcer Disease
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Imaginative Geographies of Mars: the Science and Significance of the Red Planet, 1877 - 1910
Copyright by Kristina Maria Doyle Lane 2006 The Dissertation Committee for Kristina Maria Doyle Lane Certifies that this is the approved version of the following dissertation: IMAGINATIVE GEOGRAPHIES OF MARS: THE SCIENCE AND SIGNIFICANCE OF THE RED PLANET, 1877 - 1910 Committee: Ian R. Manners, Supervisor Kelley A. Crews-Meyer Diana K. Davis Roger Hart Steven D. Hoelscher Imaginative Geographies of Mars: The Science and Significance of the Red Planet, 1877 - 1910 by Kristina Maria Doyle Lane, B.A.; M.S.C.R.P. Dissertation Presented to the Faculty of the Graduate School of The University of Texas at Austin in Partial Fulfillment of the Requirements for the Degree of Doctor of Philosophy The University of Texas at Austin August 2006 Dedication This dissertation is dedicated to Magdalena Maria Kost, who probably never would have understood why it had to be written and certainly would not have wanted to read it, but who would have been very proud nonetheless. Acknowledgments This dissertation would have been impossible without the assistance of many extremely capable and accommodating professionals. For patiently guiding me in the early research phases and then responding to countless followup email messages, I would like to thank Antoinette Beiser and Marty Hecht of the Lowell Observatory Library and Archives at Flagstaff. For introducing me to the many treasures held deep underground in our nation’s capital, I would like to thank Pam VanEe and Ed Redmond of the Geography and Map Division of the Library of Congress in Washington, D.C. For welcoming me during two brief but productive visits to the most beautiful library I have seen, I thank Brenda Corbin and Gregory Shelton of the U.S. -

Family Group Sheets Surname Index
PASSAIC COUNTY HISTORICAL SOCIETY FAMILY GROUP SHEETS SURNAME INDEX This collection of 660 folders contains over 50,000 family group sheets of families that resided in Passaic and Bergen Counties. These sheets were prepared by volunteers using the Societies various collections of church, ceme tery and bible records as well as city directo ries, county history books, newspaper abstracts and the Mattie Bowman manuscript collection. Example of a typical Family Group Sheet from the collection. PASSAIC COUNTY HISTORICAL SOCIETY FAMILY GROUP SHEETS — SURNAME INDEX A Aldous Anderson Arndt Aartse Aldrich Anderton Arnot Abbott Alenson Andolina Aronsohn Abeel Alesbrook Andreasen Arquhart Abel Alesso Andrews Arrayo Aber Alexander Andriesse (see Anderson) Arrowsmith Abers Alexandra Andruss Arthur Abildgaard Alfano Angell Arthurs Abraham Alje (see Alyea) Anger Aruesman Abrams Aljea (see Alyea) Angland Asbell Abrash Alji (see Alyea) Angle Ash Ack Allabough Anglehart Ashbee Acker Allee Anglin Ashbey Ackerman Allen Angotti Ashe Ackerson Allenan Angus Ashfield Ackert Aller Annan Ashley Acton Allerman Anners Ashman Adair Allibone Anness Ashton Adams Alliegro Annin Ashworth Adamson Allington Anson Asper Adcroft Alliot Anthony Aspinwall Addy Allison Anton Astin Adelman Allman Antoniou Astley Adolf Allmen Apel Astwood Adrian Allyton Appel Atchison Aesben Almgren Apple Ateroft Agar Almond Applebee Atha Ager Alois Applegate Atherly Agnew Alpart Appleton Atherson Ahnert Alper Apsley Atherton Aiken Alsheimer Arbuthnot Atkins Aikman Alterman Archbold Atkinson Aimone -

Appendix I Lunar and Martian Nomenclature
APPENDIX I LUNAR AND MARTIAN NOMENCLATURE LUNAR AND MARTIAN NOMENCLATURE A large number of names of craters and other features on the Moon and Mars, were accepted by the IAU General Assemblies X (Moscow, 1958), XI (Berkeley, 1961), XII (Hamburg, 1964), XIV (Brighton, 1970), and XV (Sydney, 1973). The names were suggested by the appropriate IAU Commissions (16 and 17). In particular the Lunar names accepted at the XIVth and XVth General Assemblies were recommended by the 'Working Group on Lunar Nomenclature' under the Chairmanship of Dr D. H. Menzel. The Martian names were suggested by the 'Working Group on Martian Nomenclature' under the Chairmanship of Dr G. de Vaucouleurs. At the XVth General Assembly a new 'Working Group on Planetary System Nomenclature' was formed (Chairman: Dr P. M. Millman) comprising various Task Groups, one for each particular subject. For further references see: [AU Trans. X, 259-263, 1960; XIB, 236-238, 1962; Xlffi, 203-204, 1966; xnffi, 99-105, 1968; XIVB, 63, 129, 139, 1971; Space Sci. Rev. 12, 136-186, 1971. Because at the recent General Assemblies some small changes, or corrections, were made, the complete list of Lunar and Martian Topographic Features is published here. Table 1 Lunar Craters Abbe 58S,174E Balboa 19N,83W Abbot 6N,55E Baldet 54S, 151W Abel 34S,85E Balmer 20S,70E Abul Wafa 2N,ll7E Banachiewicz 5N,80E Adams 32S,69E Banting 26N,16E Aitken 17S,173E Barbier 248, 158E AI-Biruni 18N,93E Barnard 30S,86E Alden 24S, lllE Barringer 29S,151W Aldrin I.4N,22.1E Bartels 24N,90W Alekhin 68S,131W Becquerei -

Volcan Peteroa
GEOLOGY AND GEOCHEMISTRY OF THE ACTIVE AZUFRE-PLANCHON-PETEROA VOLCANIC CENTER (35015 ' S, SOUTHERN ANDES): IMPLICATIONS FOR CORDILLERAN ARC MAGMATISM by Daniel Richard Tormey B.S. Civil Engineering and Geology, Stanford University (1983) Submitted to the Department of Earth, Atmospheric, and Planetary Sciences In Partial Fulfillment of the Requirements for the Degree of Doctor of Philosophy at the Massachusetts Institute of Technology February, 1989 ©Daniel Richard Tormey, 1989. All rights reserved The author hereby grants to M.I.T. permission to reproduce and distribute copies of this thesis document in whole or in part. Signature of Author: Department of Earth, Atmospheric, & Plane6fry Sciences, MIT 6 January 1989 Certified by: I . rederick A.Frey Thesis Supervisor Accepted by: S,, Dr. Thomas H. Jordan Chairman, Departmental Committee on Graduate Students ARCH?," AP 111989 Geology and Geochemistry of the Active Azufre-Planchon-Peteroa Volcanic Center (35015'S, Southern Andes): Implications for Cordilleran Arc Magmatism by Daniel Richard Tormey Submitted to the Department of Earth, Atmospheric, and Planetary Sciences on 6 January 1989 in partial fulfillment of the requirements for the degree of Doctor of Philosophy ABSTRACT Magmatism in convergent margin settings is the dominant mechanism of mass transfer from the mantle to the crust and of crustal growth during the Phanerozoic. The results of a detailed study of the Azufre-Planchon-Peteroa Volcanic Center and of regional comparison of volcanoes in the Southern Volcanic Zone of the Andes between 330S and 420S constrain the sources, processes, and rates operative during magmatism of the southern Andean volcanic front. The Azufre-Planchon-Peteroa Volcanic Center is located at 350 15'S, in a transition zone of crustal thickness. -
VV D C-A- R 78-03 National Space Science Data Center/ World Data Center a for Rockets and Satellites
VV D C-A- R 78-03 National Space Science Data Center/ World Data Center A For Rockets and Satellites {NASA-TM-79399) LHNAS TRANSI]_INT PHENOMENA N78-301 _7 CATAI_CG (NASA) 109 p HC AO6/MF A01 CSCl 22_ Unc.las G3 5 29842 NSSDC/WDC-A-R&S 78-03 Lunar Transient Phenomena Catalog Winifred Sawtell Cameron July 1978 National Space Science Data Center (NSSDC)/ World Data Center A for Rockets and Satellites (WDC-A-R&S) National Aeronautics and Space Administration Goddard Space Flight Center Greenbelt) Maryland 20771 CONTENTS Page INTRODUCTION ................................................... 1 SOURCES AND REFERENCES ......................................... 7 APPENDIX REFERENCES ............................................ 9 LUNAR TRANSIENT PHENOMENA .. .................................... 21 iii INTRODUCTION This catalog, which has been in preparation for publishing for many years is being offered as a preliminary one. It was intended to be automated and printed out but this form was going to be delayed for a year or more so the catalog part has been typed instead. Lunar transient phenomena have been observed for almost 1 1/2 millenia, both by the naked eye and telescopic aid. The author has been collecting these reports from the literature and personal communications for the past 17 years. It has resulted in a listing of 1468 reports representing only slight searching of the literature and probably only a fraction of the number of anomalies actually seen. The phenomena are unusual instances of temporary changes seen by observers that they reported in journals, books, and other literature. Therefore, although it seems we may be able to suggest possible aberrations as the causes of some or many of the phenomena it is presumptuous of us to think that these observers, long time students of the moon, were not aware of most of them. -

Astrobiology and the Possibility of Life on Earth and Elsewhere…
Space Sci Rev DOI 10.1007/s11214-015-0196-1 Astrobiology and the Possibility of Life on Earth andElsewhere... Hervé Cottin1 · Julia Michelle Kotler2,3 · Kristin Bartik4 · H. James Cleaves II5,6,7,8 · Charles S. Cockell9 · Jean-Pierre P. de Vera10 · Pascale Ehrenfreund11 · Stefan Leuko12 · Inge Loes Ten Kate13 · Zita Martins14 · Robert Pascal15 · Richard Quinn16 · Petra Rettberg12 · Frances Westall17 Received: 24 September 2014 / Accepted: 6 August 2015 © Springer Science+Business Media Dordrecht 2015 Abstract Astrobiology is an interdisciplinary scientific field not only focused on the search of extraterrestrial life, but also on deciphering the key environmental parameters that have enabled the emergence of life on Earth. Understanding these physical and chemical parame- ters is fundamental knowledge necessary not only for discovering life or signs of life on other planets, but also for understanding our own terrestrial environment. Therefore, astrobiology pushes us to combine different perspectives such as the conditions on the primitive Earth, the B H. Cottin [email protected] 1 LISA, UMR CNRS 7583, Université Paris Est Créteil et Université Paris Diderot, Institut Pierre Simon Laplace, 61, av du Général de Gaulle, 94010 Créteil Cedex, France 2 Leiden Institute of Chemistry, P.O. Box 9502, 2300 Leiden, The Netherlands 3 Faculty of Applied Sciences, City of Oxford College, Oxpens Road, Oxford, OX1 1SA, UK 4 EMNS, Ecole Polytechnique, Université libre de Bruxelles, 1050 Bruxelles, Belgium 5 Blue Marble Space Institute of Science, -

Investigating the Optimal Integration of Airborne, Ship-Borne, Satellite and Terrestrial Gravity Data for Use in Geoid Determination
INVESTIGATING THE OPTIMAL INTEGRATION OF AIRBORNE, SHIP-BORNE, SATELLITE AND TERRESTRIAL GRAVITY DATA FOR USE IN GEOID DETERMINATION BY Rachelle Lee Winefield A thesis submitted to the Victoria University of Wellington in fulfilment of the requirements for the degree of Master of Science Geophysics School of Geography, Environmental and Earth Science Victoria University of Wellington 2016 “Gravity is a habit that is hard to shake off.” - Terry Pratchett Abstract Each gravity observation technique has different parameters and contributes to different pieces of the gravity spectrum. This means that no one gravity dataset is able to model the Earth’s gravity field completely and the best gravity map is one derived from many sources. Therefore, one of the challenges in gravity field modelling is combining multiple types of heterogeneous gravity datasets. The aim of this study is to determine the optimal method to produce a single gravity map of the Canterbury case study area, for the purposes of use in geoid modelling. This objective is realised through the identification and application of a four-step integration process: purpose, data, combination and assessment. This includes the evaluation of three integration methods: natural neighbour, ordinary kriging and least squares collocation. As geoid modelling requires the combination of gravity datasets collected at various altitudes, it is beneficial to be able to combine the dataset using an integration method which operates in a three- dimensional space. Of the three integration methods assessed, least squares collocation is the only integration method which is able to perform this type of reduction. The resulting product is a Bouguer anomaly map of the Canterbury case study area, which combines satellite altimetry, terrestrial, ship-borne, airborne, and satellite gravimetry using least squares collocation. -
Creditor Matrix
Case 19-10488 Doc 15 Filed 03/11/19 Page 1 of 103 Creditor Matrix NAME ADDRESS 1 ADDRESS 2 ADDRESS 3 ADDRESS 4 CITY STATE ZIP COUNTRY 1 MILLION 4 ANNA 15301 DALLAS PKWY #1100 ADDISON TX 75001 119 LEAWOOD LLC TOWN CENTER CROSSING PO BOX 3536 COLUMBUS OH 43260-3536 1515 N HALSTED LLC PO BOX 851319 MINNEAPOLIS MN 55485-1319 1515 N HALSTED, LLC C/O BUCKSBAUM RETAIL PROPERTIES 71 S WACKER DR, STE 2310 CHICAGO IL 60606 22 INTERIORS 3940 LAUREL CANYON BLVD. #1022 STUDIO CITY CA 91604 223-1 DL HOLDINGS LLC-LA92800 C/O INWOOD NATIONAL BANK PO BOX 9124 DALLAS TX 75209 23RD GROUP LLC 4994 PARKWAY PLAZA BLVD. STE 400 CHARLOTTE NC 28217 24 SEVEN STAFFING INC. PO BOX 5786 HICKSVILLE NY 11802-5786 3 GGG'S TRUCK LINES INC. PO BOX 4003 SOUTH GATE CA 90280 3 GGG'S TRUCK LINES INC. C/O NATIONAL BANKERS TRUST PO BOX 1752 MEMPHIS TN 38101-1752 360 CATERING AND EVENTS LLC. 5439 PERSHING AVENUE FORT WORTH TX 76107 3BS CO. LTD. 64/282 ROYALNINE BUILDING 25 FL RAMA 9 RD BANGKAPI HUAYKWANG TH BANGKOK THAILAND 3S CORPORATION 1251 E WALNUT CARSON CA 90746 4 LEATHER REPAIR 2785 WEIGL ROAD SAGINAW MI 48609 4698 CLAY TERRACE PARTNERS LLC PO BOX 643726 PITTSBURGH PA 15264-3726 4TH STREET HOLDINGS LLC C/O BOND RETAIL 5 THIRD STREET, STE 1225 SAN FRANCISCO CA 94103 770 TAMALPAIS DRIVE INC. C/O MADISON MARQUETTE-MGMT OFFICE 100 CORTE MADERA TOWN CENTER CORTE MADERA CA 94925 80 TWENTY LLC ATTN: ALP ONURLU 657 MISSION ST., STE 402 SAN FRANCISCO CA 94105 A&G REALTY PARTNERS, LLC ATTN: ANDREW GRAISER 445 BROADHOLLOW ROAD, SUITE 410 MELVILLE NY 11747 A&S HOME FASHION CORP. -

National Reports by Country 2019
National Reports by country 2019 Australia Belgium Canada China Chinese Taipei Finland Germany Ireland Israel Japan Norway Poland USA Report for the year 2019 and future activities SOLAS Australia compiled by: Andrew Bowie and Ruhi Humphries This report has two parts: - Part 1: reporting of activities in the period of January 2019 - Jan/Feb 2020 - Part 2: reporting on planned activities for 2020 and 2021. The information provided will be used for reporting, fundraising, network ing, strategic development and updating of the live web-based implementation plan. As much as possible, please indicate the specific SOLAS 2015-2025 Science Plan Themes addressed by each activity or specify an overlap between Themes or Cross-Cutting Themes. 1 Greenhouse gases and the oceans; 2 Air-sea interfaces and fluxes of mass and energy; 3 Atmospheric deposition and ocean biogeochemistry; 4 Interconnections between aerosols, clouds, and marine ecosystems; 5 Ocean biogeochemical control on atmospheric chemistry; Integrated studies of high sensitivity systems; Environmental impacts of geoengineering; Science and society. IM PORTANT: This report should reflect the efforts of the SOLAS community in the entire country you are representing (all universities, institutes, lab, units, groups , cities). First things first…Please tell us what the IPO may do to help you in your current and future SOLAS activities. ? PART 1 - Activities from January 2019 to Jan/Feb 2020 1. Scientific highlight Describe one scientific highlight with a title, text (max. 300 words), a figure with legend and full references. Please focus on a result that would not have happened without SOLAS, and we are most interested in results of international collaborations. -
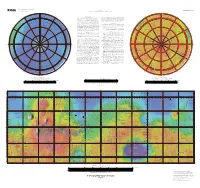
Topographic Map of Mars
U.S. DEPARTMENT OF THE INTERIOR OPEN-FILE REPORT 02-282 U.S. GEOLOGICAL SURVEY Prepared for the NATIONAL AERONAUTICS AND SPACE ADMINISTRATION 180° 0° 55° –55° Russell Stokes 150°E NOACHIS 30°E 210°W 330°W 210°E NOTES ON BASE smooth global color look-up table. Note that the chosen color scheme simply 330°E Darwin 150°W This map is based on data from the Mars Orbiter Laser Altimeter (MOLA) 30°W — 60° represents elevation changes and is not intended to imply anything about –60° Chalcoporous v (Smith and others 2001), an instrument on NASA’s Mars Global Surveyor Milankovic surface characteristics (e.g. past or current presence of water or ice). These two (MGS) spacecraft (Albee and others 2001). The image used for the base of this files were then merged and scaled to 1:25 million for the Mercator portion and Rupes map represents more than 600 million measurements gathered between 1999 1:15,196,708 for the two Polar Stereographic portions, with a resolution of 300 and 2001, adjusted for consistency (Neumann and others 2001 and 2002) and S dots per inch. The projections have a common scale of 1:13,923,113 at ±56° TIA E T converted to planetary radii. These have been converted to elevations above the latitude. N S B LANI O A O areoid as determined from a martian gravity field solution GMM2 (Lemoine Wegener a R M S s T u and others 2001), truncated to degree and order 50, and oriented according to IS s NOMENCLATURE y I E t e M i current standards (see below). -

Ændringer Og Udfordringer
Ændringer og udfordringer Rapport fra workshop 1 på Nationalmuseet 29. september 2010 Redigeret af Hans Christian Gulløv, Caroline Paulsen og Birgit Rønne Ændringer og udfordringer Rapport fra workshop 1 på Nationalmuseet 29. september 2010 Copyright © Nationalmuseet og forfatterne Redigeret af Hans Christian Gulløv, Caroline Paulsen og Birgit Rønne Layout Anne Marie Brammer Tryk: Rosendahls - Schultz Grafisk ISBN: 978-87-7602-159-7 Udgivet med støtte fra Augustinusfonden og Nationalmuseet En digital version af publikationen findes på Nationalmuseets hjemmeside: http://nordligeverdener.natmus.dk/ Forsidefoto: Landskab på Flatøy, Helgeland, Norge. Foto: Flemming Kaul Nordlige Verdener – ændringer og udfordringer Rapport fra workshop 1 på Nationalmuseet 29. september 2010 Redigeret af Hans Christian Gulløv, Caroline Paulsen og Birgit Rønne København 2011 2 Indhold • Ændringer og udfordringer – status for Nordlige Verdener 4 Hans Christian Gulløv • Perspektiver og skalaer: Analytiske udfordringer til 6 ’Nordlige Verdener’ | Kirsten Hastrup Forskningssøjle A Klimaændringer og samfund: Når klimagrænser flytter sig 18 • Senistidens Danmark | Morten Fischer Mortensen 20 • ’Små træer’ fra Nordøstgrønland | Claudia Baittinger 26 • Qajaa, en frossen arkæologisk perle 30 Jørgen Hollesen, Henning Matthiesen og Jan Bruun Jensen • Konserverings- og tørringsmetoder tilpasset arkæologiske 34 materialer fundet i nordlige områder | Poul Jensen • Kampen om Vejret – Den tyske snehulestation på 37 Shannon Ø 1943/44 | Tilo Krause og Jens Fog Jensen • Samfundsændringer -

NAMES of U. S. PEACE DELEGA TES ANNOUNCED It Was Announced at the Ex- Tary of State, the Hon
PVBLISHED DAILY under order of THE PRESZZDENT of THE UNITED STATEX by COMMITTEE on PUBLIC INFORMATION GEORGE CREEL, Chairman * * * COMPLETE Record of U. S. GOVERNMENT Activities VOL. 2 WASHINGTON, SATURDAY, NOVEMBER 30, 1918. No. 476 NAMES OF U. S. PEACE DELEGA TES ANNOUNCED It was announced at the Ex- tary of State, the Hon. Henry these appointments before be- ecutive Offices last night that White, recently ambassador to cause the number of repre- the representatives of the France, -1Mr. Edward M. House, sentatives each of the chief United States at the Peace and Gen. Tasker H. Bliss. belligerents was to send had, Conferences would be the It was explained that it had until a day or two ago, been President himself, the Secre- not been possible to announce under discussion. CONSERVATION WEEK PROGRAM NO CENSORSHIP OF FILMS FOR EXECUTIVE ORDER EXCEPTING FOR WORLD RELIEF ANNOUNCED EXPORT AFTER DECEMBER 9 CERTAIN PERSONS FROM BEING BY THE FOOD ADMINISTRATION The Committee ort Public Information CLASSIFIED AS ALIEN ENEMIES authorizes the following announcement: STARTS-WITH WORD FROM HOOVER At a conference called yesterday by Dr. ATTORNEY GENERAL'S CERTIFICATE L. S. Rowe, Assistant Secretary of the Treasury, and participated in by the Cus- To Be- Read in All Churches on toms, the War Trade Board, and the Com- Privilege of Applying for Naturali- mittee on Public Information, it was de- Sunday-Meetings of Many Or- cided that on and after Monday, Decem- zation to Be Extended All Those ganizations Scheduled - Must her 9, there will be no egnsorship of films Who, After Investigation, Are for export either by the Customs or by the Save to Keep U.