Annu Al Diving F a Tality Ra Tes Among Insured D an Members
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Participant Guide
Participant Guide National High Adventure Sea Base, BSA Sea Base Scuba Programs Islamorada, Florida Scuba Adventure Scuba Certification Scuba Live Aboard Revised Date: 2.23.2021 Mission of the Boy Scouts of America The mission of the Boy Scouts of America is to prepare young people to make ethical and moral choices over their lifetime by instilling in them the values of the Scout Oath and Law. Scout Oath On my honor I will do my best to do my duty to God and my country and to obey the Scout Law; to help other people at all times; to keep myself physically strong, mentally awake, and morally straight. Scout Law A Scout is: Trustworthy. Loyal. Helpful. Friendly. Courteous. Kind. Obedient. Cheerful. Thrifty. Brave. Clean. Reverent. Mission Statement of Sea Base, BSA It is the mission of Sea Base to serve councils and units by providing an outstanding high adventure experience for older Boy Scouts, Varsity Scouts, Venturers, Sea Scouts and their leaders. Sea Base programs are designed to achieve the principal aims of the Boy Scouts of America: • To build character • To foster citizenship • To develop physical, mental, and emotional fitness Keys Blessing Bless the creatures of the Sea Bless this person I call me Bless the Keys, you make so grand Bless the sun that warms the land Bless the fellowship we feel As we gather for this meal Amen Page | 2 Table of Contents General Eligibility Requirements ................................................................................................................. 4 General Eligibility at a Glance -

Cocos Islands
2,48 € - De ware betekenis van ‘STRETCH’ De nieuwe Elasteks van BARE N° 220 - September 2008 Pakken die je passen alsof ze met een spuitbus zijn opgebracht; pakken die je lijf volgen in elke curve en elke bocht, hoe je ook staat, ligt of beweegt. Geen ruimte voor water en geen plaats voor de kou. Dat is comfort in 3D; dat is BARE. Alléén BARE gaat zo ver. Bondsnieuws EUF-certificatie Reportage Disaster Victim Indentification Je Bare dealer heeft precies de juiste maat voor je. Reportage De slanke knotslak Reportage Cocos Islands TWEEMAANDELIJKS INFORMATIEBLAD (NIET IN JULI EN AUGUSTUS) VAN DE NEDERLANDSTALIGE LIGA VOOR ONDERWATERONDERZOEK EN -SPORT ‘NELOS’ - LIGA VOOR ONDERWATERONDERZOEK EN -SPORT ‘NELOS’ VAN DE NEDERLANDSTALIGE (NIET IN JULI EN AUGUSTUS) TWEEMAANDELIJKS INFORMATIEBLAD BARE Wet ad NL Hypoc.indd 1 4/10/2008 4:04:14 PM GALILEO TERRA LUISTER GRATIS NAAR JE HART ONDER WATER ! Bij aankoop van een terra ontvangt u de HRM upgrade kit (t.w.v. € 200,-) geheel gratis ! UWATEC combineert vooruitstrevende technologie en modern design met het ontwikkelen van dé ultieme computer. PDIS (Profi le Dependent Intermediate Stop), een exclusiviteit van UWATEC, optimaliseert uw duik in complete veiligheid. De Galileo Sol is baanbrekend met zijn innovatieve hartslagmeter voor exacte decompressieberekeningen en een full tilt digitaal kompas voor nauwkeurige navigatie, inclusief markeringsgeheugen. Deze gebruikersvriendelijke, interactieve computer mag trots zijn op een buitengewoon breedbeeld dot matrix scherm met drie display opties en veelvoudige, door de gebruiker in te stellen, eigenschappen. De terra versie van de Galileo is op de markt gebracht en speciaal ontwikkeld voor de duik(ster) die alle progressieve eigenschappen van de Galileo sol wenst, maar de voorkeur geeft aan een traditionele manometer. -

Bathynomus Giganteus) Using Reflex Impairment
Florida State University Libraries 2016 Post-Release Mortality of Deep Sea Bycatch Species Brendan Suneel Talwar Follow this and additional works at the FSU Digital Library. For more information, please contact [email protected] FLORIDA STATE UNIVERSITY COLLEGE OF ARTS & SCIENCES POST-RELEASE MORTALITY OF DEEP SEA BYCATCH SPECIES By BRENDAN SUNEEL TALWAR A Thesis submitted to the Department of Biological Science in partial fulfillment of the requirements for the degree of Master of Science 2016 Brendan Suneel Talwar defended this thesis on March 31, 2016. The members of the supervisory committee were: R. Dean Grubbs Professor Directing Thesis Edward J. Brooks Committee Member Don Levitan Committee Member Joseph Travis Committee Member The Graduate School has verified and approved the above-named committee members, and certifies that the thesis has been approved in accordance with university requirements. ii This thesis is dedicated to Sydney and Sara. iii ACKNOWLEDGMENTS This thesis represents the hard work, generosity, and support of countless friends, family members, advisors, and students. Let me begin by acknowledging everyone that helped see it through, from heavily invested volunteers to strangers who donated the funds to get this work off the ground- this would not have been possible without you. I offer my sincerest thanks to my advisor, Dean Grubbs, for his guidance, support, and incredible expertise. The independence I was afforded within the Grubbs Lab pushed me to become heavily invested in my work and ultimately gain more from my Master’s degree than I thought possible, a testament to his mentorship. I must also thank Edd Brooks and Travis Perry for the opportunities that they have given me since the beginning of my career. -
Diving in Guam
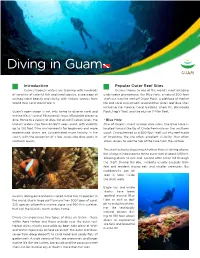
Diving in Guam Introduction Popular Outer Reef Sites Guam’s tropical waters are teaming with hundreds Guam is home to one of the world’s most amazing of varieties of colorful fish and coral species, a seascape of underwater phenomena, the Blue Hole, a natural 300-foot unimaginable beauty and clarity, with historic wrecks from shaft cut into the reef off Orote Point. A plethora of marine World War I and World War II. life and coral also inhabit several other outer reef dive sites including the Crevice, Coral Gardens, Shark Pit, Barracuda Guam’s open ocean is not only home to diverse coral and Rock, Hap’s Reef, and the elusive 11-Mile Reef. marine life; it’s one of Micronesia’s most affordable places to dive. Home to a variety of dives for all certification levels, the • Blue Hole island’s waters stay from 82-86°F year-round, with visibility One of Guam’s most unique dive sites, the Blue Hole is up to 150 feet. Dive environments for beginners and more located toward the tip of Orote Peninsula on the southern experienced divers are concentrated more heavily in the coast. Characterized as a 300-foot shaft cut into reef made south, with the exception of a few accessible dive spots in of limestone, the site offers excellent visibility that often northern Guam. allows divers to see the top of the hole from the surface. The shaft actually drops much further than air diving allows, but a large window opens to the outer wall at about 125 feet, allowing divers to exit and ascend after a free fall through the shaft. -

SNUBA® Waiver
DO NOT ALTER FORM Reviewed by: Participant Record and Liability Release (SNUBA® Guide Name) Name (complete): Birth Date: / / (Month/Day/Year) Street Address: City: State/Country: Zip Code: Phone: E-mail: Emergency Contact: Emergency Number: Please answer the following questions on your past or present medical history with a YES or NO. If you answer yes, you will not be able to participate. Be honest with your responses. Do not put your health at risk. 1. Are you pregnant or do you believe you might be pregnant? 2. Do you have a history of heart attacks, strokes or heart disease? 3. Have you ever had heart surgery, angina or blood vessel surgery? 4. Do you have asthma and are currently using an inhaler? 5. Are you currently under the influence of mind-altering drugs or alcohol? 6. Do you have any form of lung disease? 7. Do you have epilepsy, seizures or convulsions or take medications to prevent them? Please answer the following questions on your past or present medical history with a YES or NO. A positive response does not necessarily disqualify you from SNUBA. Be honest with your responses. Do not put your health at risk. 8. Do you have a history of blackouts or fainting? 9. Do you currently have a head cold (congestion), sinusitis or bronchitis? 10. Do you have a history of diabetes affecting your ability to participate in a strenuous activity? 11. Do you have a history of asthma or wheezing with breathing or exercise? 12. Have you ever had a diving accident or decompression sickness? 13. -

2 WHVS 4: 2009 Voluntary Standard for Recreational SCUBA Diving And
WD - 2 WHVS 4: 2009 Keywords: conservation; coral reefs; environment; marine recreation; preferred practices for good environmental behavior; SCUBA diving, snorkeling, SNUBA diving. Voluntary Standard for Recreational SCUBA diving and Snorkeling Activities in West Hawaii Waters Prepared by: Members of the West Hawaii Community with the assistance of the Coral Reef Alliance. Abstract: This voluntary standard specifies requirements for environmental performance, conservation practices and operational safety that enhance SCUBA and SNUBA diving, and snorkeling activities while minimizing environmental impacts of recreational usage on fragile marine ecosystems in the waters of West Hawaii - particularly near-shore coral reefs, related coastal environments and impacts on marine species such as cetaceans, turtles, monk seals, and other animals. This standard was developed by community members within West Hawaii representing key interest groups with the assistance of the Coral Reef Alliance (CORAL) and the West Hawaii Standards Taskforce (WHST). WHST and CORAL disclaim all liability for its use, application, or adaptation. This standard is subject to revision at any time and must be reviewed every five years and if not revised either reaffirmed or withdrawn. Copyright © 2009 Contents 1.0 Scope 2.0 Referenced Documents 3.0 Definitions 4.0 Requirements 4.1 Operational Practices 4.2 Training and Briefing requirements Annex A. Environmental briefing outline and checklist for SCUBA and Snorkeling B. Environmental pledge for SCUBA divers and snorklers -

Snuba: Automating Weak Supervision to Label Training Data
Snuba: Automating Weak Supervision to Label Training Data Paroma Varma Christopher Re´ Stanford University Stanford University [email protected] [email protected] ABSTRACT benign, malignant if area > 210.8: As deep learning models are applied to increasingly diverse return False Label if area < 150: Aggregator problems, a key bottleneck is gathering enough high-quality return Abstain training labels tailored to each task. Users therefore turn Labeled Data 25% benign, 75%benign, ... ?, ?, ?, ? if perim > 120: to weak supervision, relying on imperfect sources of labels return True like pattern matching and user-defined heuristics. Unfor- if perim > 80 Terminate? return Abstain tunately, users have to design these sources for each task. Heuristic Generation Training Labels This process can be time consuming and expensive: domain Unlabeled Data Snuba experts often perform repetitive steps like guessing optimal numerical thresholds and developing informative text pat- Figure 1: Snuba uses a small labeled and a large unlabeled terns. To address these challenges, we present Snuba,a dataset to iteratively generate heuristics. It uses existing la- system to automatically generate heuristics using a small bel aggregators to assign training labels to the large dataset. labeled dataset to assign training labels to a large, unla- beled dataset in the weak supervision setting. Snuba gen- pervision, or methods that can assign noisy training labels erates heuristics that each labels the subset of the data it to unlabeled data, like crowdsourcing [9, 22, 60], distant su- is accurate for, and iteratively repeats this process until the pervision [8,32], and user-defined heuristics [38,39,50]. Over heuristics together label a large portion of the unlabeled the past few years, we have been part of the broader effort data. -

Conservation Diver Course
Conservation Diver Course Conservation Diver Course 1 Inhoud 1 Introduction ..................................................................................................................................... 5 2 Taxonomy ........................................................................................................................................ 7 2.1 Introduction ..................................................................................................................................... 7 2.2 What is taxonomy? .......................................................................................................................... 8 2.3 A brief history of taxonomy ............................................................................................................. 9 2.4 Scientific names ............................................................................................................................. 10 2.5 The hierarchical system of classification ....................................................................................... 12 2.5.1 Species ................................................................................................................................... 13 2.5.2 Genus ..................................................................................................................................... 13 2.5.3 Family .................................................................................................................................... 14 2.5.4 Order .................................................................................................................................... -

BAHAMAS the ONE and ONLY RESORT Two Tickets to Paradise
2017 2017 BAHAMAS THE ONE AND ONLY RESORT Two Tickets to Paradise Our gratitude for what you do knows no boundaries. Hubbell Lighting attributes our success to the countless hours you spend helping customers find the right products for every project. That’s why we’ve planned this great escape to the carefree Caribbean to reward you. Our vibrant, festive journey includes 4 nights & 5 days on the tranquil shores of Paradise Island, Bahamas. The itinerary is the perfect blend of indulgence, camaraderie and adventure. Breathtaking sights, decadent accommodations, tropical drinks, golf, shopping, and exhilarating outdoor activities await you. More Than Just Another Pretty Place Just southeast of Florida lie 700 islands, cays, and islets known as the Commonwealth of the Bahamas. The warm and winterless expanse of islands is home primarily to African Americans (90%) who are descendants of freed slaves from Bermuda and the United States. While English is the official language, many Bahamians speak an English based Creole dialect. The culture is rich with the influence of African, Caribbean and European influences. Folklore and legends abound in the colorful islands, including tales of the lost city of Atlantis. Throughout the islands, you’ll be serenaded by African rhythms, Caribbean calypso, English folk songs and the unique Bahamian goombay traditional music, combining African musical traditions with European colonial influences. Junkanoo is uniquely Bahamian and exists nowhere else. It’s an incredibly energetic, colorful parade made up of brightly costumed Bahamians dancing and “rushin” to the music of cowbells, drums, horns and whistles. The popular belief is that John Canoe, an African tribal chief, created Junkanoo when he demanded the right to celebrate with his people even after he was brought to the West Indies as a slave in the 16th century. -

Vuosikertomus 2020
Sukeltajaliitto ry:n VUOSIKERTOMUS 2020 VUOSIKERTOMUS 2020 Kerran sukeltaja, aina sukeltaja VUOSIKERTOMUS 2020 Sukeltajaliitto ry TP 1 SUKELTAJALIITTO NUMEROINA SukeltajaliittoSukeltajaliitto ry:n VUOSIKERTOMUS 2020 JÄSENIÄ SEUROISSA SEUROJA 147 Sisällys 8185 4 Puheenjohtajan katsaus - Ordförandes översikt 6 Vuoden kohokohdat HENKILÖJÄSENIÄ 8 Ansioituneet 369 10 Organisaatio SUORITETTUJA 12 Jäsenyydet ja edustukset SUKELLUSKURSSEJA 14 Viestintä VAPAAEHTOISIA 16 Vaikuttamistyö 580 LIITON TEHTÄVISSÄ NOIN 18 Palvelut jäsenille 20 Valiokunnat YHTEISÖJÄSENIÄ 180 28 Jäsenet 10 32 Talous SUORITETTUJA KOULUTTAJAKURSSEJA 127 Vuonna 2020 julkaistiin Sukeltajaliiton tasa-arvo- ja yhdenvertaisuussuunnitelma, Elina Rajala jonka teemoja kuvittavat erilaiset sammakkohahmot. Julkaisija Visuaalinen ilme Takakannen kuva Sukeltajaliitto ry ja kuvitukset: Ari Nieminen Elina Rajala Valimotie 10 00380 Helsinki Etukannen kuva Arvomme ovat vaikuttavuus, www.sukeltaja.fi Tommi Pasanen avoimuus ja vastuullisuus. 2 3 Mika Saareila PUHEENJOHTAJAN KATSAUS - ORDFÖRANDES ÖVERSIKT Sukeltajaliitto ry:n VUOSIKERTOMUS 2020 Erikoinen vuosi 2020 Ett ovanligt år 2020 TAKANA ON vuosi, jonka kukaan ei aavistanut tulevan. VI HAR upplevt ett år som ingen kunde förutse. Corona- Pandemiaksi yltynyt koronaepidemia laittoi maailman pol- pandemin slog av fötterna under hela världen. I början av villeen. Vuoden alussa ei olisi voinut uskonut, että suurin året skulle ingen av oss ha trott att en stor del av Dykarför- osa Sukeltajaliiton ja sen seurojen uimahallitoiminnasta bundets och -

Join the Movement
THE UNDERSEA ® JOURNAL KEEPING PADI PROFESSIONALS INFORMED, INSPIRED AND INVOLVED SINCE 1967 THIRD QUARTER 2011 PROJECT AWARE RELAUNCH RELAUNCH AWARE PROJECT » NEW REBREATHER COURSES COURSES NEW REBREATHER » ECO-TOURISM TRAVEL TRAVEL ECO-TOURISM » BUSINESS: GOING GREEN BUSINESS: THIRD JOIN THE QUARTER MOVEMENT 2011 CONTENTSTHE UNDERSEA JOURNAL THIRD QUARTER 2011 Features Departments 46l LIVING SEAS: PROJECT 6 l In the Field AWARE PADI Worldwide President Protecting Our Ocean and COO Drew Richard- Planet One Dive at a son calls on PADI Members Time to join Project AWARE in its BY JENNY MILLER GARMENDIA e"orts to force meaningful pol- Project AWARE has launched icy change that will guarantee its new logo, mission and the future health of the plan- vision – and calls on you to et’s oceans. help address critical issues facing the world’s oceans: 11 l PADI Life shark conservation and A look at DEMA Show 2011. marine debris. 83 l Training Bulletin 54 l BUSINESS OF DIVING Why Conservation? 92 l RISK MANAGEMENT BY MEGAN DENNY Training Scuba Make your business more Divers: A Fatality and profitable by using eco- Risk Analysis friendly ideas that reduce 46 BY JOHN KINSELLA your costs and help the !e third part in our series environment. analyzing the findings in 64 Dr. Drew Richardson’s paper 62 l TRAINING Rebreather Training Scuba Divers: A Fatal- Launch ity and Risk Analysis. !is issue, BY KARL SHREEVES we examine fatalities that !e PADI organization occurred outside PADI-sanc- introduces new courses this tioned training programs and quarter: PADI Rebreather those that involved PADI div- Diver, Advanced Rebreather ing professionals. -

Water Sports Descriptions
Water sports descriptions All inclusive products Kayaks Come by yourself or with a friend to enjoy one of the most popular all inclusive watersports at the hotel, with our Kayaks you’ll be able to enjoy and feel the adrenaline of the waves and have a watersports challenge. Kayaks can be used as many times as the customer wants for up to 60min per use. No deposit needed. Zayaks Float on your stomach and paddle with your legs and hands to see the world below. This amazing board offers a clear view port that you put your head into and give you the chance to see the world below. Easier than snorkeling and more fun, with Zayak there is no more clearing your mask, and swallowing sea water, just lay on it and start enjoying. Hobie Cat If you have experiences sailing this is the activity for you! Take advantage of riding our hobbie cat around the cost, and enjoy a quite trip on the surroundings of the beach. If you don’t have experience, ask for our private classes and after couple of classes you can start riding the hobbie cat by yourself. Paddle Board Paddle board is the best way to discover the hotel coastline! As a mix between windsurfing and kayaking, paddle boarding is the perfect way to be on the sea. Ask for your paddle board at the hotel watersport center and you are ready to go! Diving test (Free) This is a complementary activity for those who want to try diving without getting out of the hotel; the diving test is the best way to venture you into diving in a completely quiet and control environment.