Volume 17 (2010), Article 6
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Mother of the Nation: Femininity, Modernity, and Class in the Image of Empress Teimei
Mother of the Nation: Femininity, Modernity, and Class in the Image of Empress Teimei By ©2016 Alison Miller Submitted to the graduate degree program in the History of Art and the Graduate Faculty of the University of Kansas in partial fulfillment of the requirements for the degree of Doctor of Philosophy. ________________________________ Chairperson Dr. Maki Kaneko ________________________________ Dr. Sherry Fowler ________________________________ Dr. David Cateforis ________________________________ Dr. John Pultz ________________________________ Dr. Akiko Takeyama Date Defended: April 15, 2016 The Dissertation Committee for Alison Miller certifies that this is the approved version of the following dissertation: Mother of the Nation: Femininity, Modernity, and Class in the Image of Empress Teimei ________________________________ Chairperson Dr. Maki Kaneko Date approved: April 15, 2016 ii Abstract This dissertation examines the political significance of the image of the Japanese Empress Teimei (1884-1951) with a focus on issues of gender and class. During the first three decades of the twentieth century, Japanese society underwent significant changes in a short amount of time. After the intense modernizations of the late nineteenth century, the start of the twentieth century witnessed an increase in overseas militarism, turbulent domestic politics, an evolving middle class, and the expansion of roles for women to play outside the home. As such, the early decades of the twentieth century in Japan were a crucial period for the formation of modern ideas about femininity and womanhood. Before, during, and after the rule of her husband Emperor Taishō (1879-1926; r. 1912-1926), Empress Teimei held a highly public role, and was frequently seen in a variety of visual media. -

Tourists in Paradise Writing the Pure Land in Medieval Japanese Fiction
Japanese Journal of Religious Studies 33/2: 269–296 © 2006 Nanzan Institute for Religion and Culture R. Keller Kimbrough Tourists in Paradise Writing the Pure Land in Medieval Japanese Fiction Late-medieval Japanese fiction contains numerous accounts of lay and monastic travelers to the Pure Land and other extra-human realms. In many cases, the “tourists” are granted guided tours, after which they are returned to the mun- dane world in order to tell of their unusual experiences. This article explores several of these stories from around the sixteenth century, including, most prominently, Fuji no hitoana sōshi, Tengu no dairi, and a section of Seiganji engi. I discuss the plots and conventions of these and other narratives, most of which appear to be based upon earlier oral tales employed in preaching and fund-raising, in order to illuminate their implications for our understanding of Pure Land-oriented Buddhism in late-medieval Japan. I also seek to demon- strate the diversity and subjectivity of Pure Land religious experience, and the sometimes startling gap between orthodox doctrinal and popular vernacular representations of Pure Land practices and beliefs. keywords: otogizōshi – jisha engi – shaji engi – Fuji no hitoana sōshi – Bishamon no honji – Tengu no dairi – Seiganji engi – hell – travel R. Keller Kimbrough is an assistant professor of Japanese Literature at the University of Colorado at Boulder. 269 ccording to an anonymous work of fifteenth- or early sixteenth- century Japanese fiction by the name of Chōhōji yomigaeri no sōshi 長宝 寺よみがへりの草紙 [Back from the dead at Chōhōji Temple], the Japa- Anese Buddhist nun Keishin dropped dead on the sixth day of the sixth month of Eikyō 11 (1439), made her way to the court of King Enma, ruler of the under- world, and there received the King’s personal religious instruction and a trau- matic tour of hell. -

Japan Studies Review
JAPAN STUDIES REVIEW Volume Nineteen 2015 Interdisciplinary Studies of Modern Japan Steven Heine Editor Editorial Board John A. Tucker, East Carolina University Yumiko Hulvey, University of Florida Matthew Marr, Florida International University Ann Wehmeyer, University of Florida Hitomi Yoshio, Florida International University Copy and Production María Sol Echarren Rebecca Richko Ian Verhine Kimberly Zwez JAPAN STUDIES REVIEW VOLUME NINETEEN 2015 A publication of Florida International University and the Southern Japan Seminar CONTENTS Editor’s Introduction i Re: Subscriptions, Submissions, and Comments ii ARTICLES Going Postal: Empire Building through Miniature Messages on German and Japanese Stamps Fabian Bauwens 3 Old, New, Borrowed, and Blue: Hiroshi Senju’s Waterfall Paintings as Intersections of Innovation Peter L. Doebler 37 Delightfully Sauced: Wine Manga and the Japanese Sommelier’s Rise to the Top of the French Wine World Jason Christopher Jones 55 “Fairness” and Japanese Government Subsidies for Sickness Insurances Yoneyuki Sugita 85 ESSAYS A “Brief Era of Experimentation”: How the Early Meiji Political Debates Shaped Japanese Political Terminology Bradly Hammond 117 The Night Crane: Nun Abutsu’s Yoru No Tsuru Introduced, Translated, and Annotated Eric Esteban 135 BOOK REVIEWS Scream from the Shadows: The Women’s Liberation Movement in Japan By Setsu Shigematsu Reviewed by Julia C. Bullock 169 Critical Buddhism: Engaging with Modern Japanese Buddhist Thought By James Mark Shields Reviewed by Steven Heine 172 Banzai Babe Ruth: Baseball, Espionage, & Assassination During the 1934 Tour of Japan By Robert K. Fitts Reviewed by Daniel A. Métraux 175 Supreme Commander: MacArther’s Triumph in Japan By Seymour Morris Reviewed by Daniel A. Métraux 177 CONTRIBUTORS/EDITORS i EDITOR’S INTRODUCTION Welcome to the nineteenth volume of the Japan Studies Review (JSR), an annual peer-reviewed journal sponsored by the Asian Studies Program at Florida International University Seminar. -

Representations of Pleasure and Worship in Sankei Mandara Talia J
Mapping Sacred Spaces: Representations of Pleasure and Worship in Sankei mandara Talia J. Andrei Submitted in partial fulfillment of the Requirements for the degree of Doctor of Philosophy in the Graduate School of Arts and Sciences Columbia University 2016 © 2016 Talia J.Andrei All rights reserved Abstract Mapping Sacred Spaces: Representations of Pleasure and Worship in Sankei Mandara Talia J. Andrei This dissertation examines the historical and artistic circumstances behind the emergence in late medieval Japan of a short-lived genre of painting referred to as sankei mandara (pilgrimage mandalas). The paintings are large-scale topographical depictions of sacred sites and served as promotional material for temples and shrines in need of financial support to encourage pilgrimage, offering travelers worldly and spiritual benefits while inspiring them to donate liberally. Itinerant monks and nuns used the mandara in recitation performances (etoki) to lead audiences on virtual pilgrimages, decoding the pictorial clues and touting the benefits of the site shown. Addressing themselves to the newly risen commoner class following the collapse of the aristocratic order, sankei mandara depict commoners in the role of patron and pilgrim, the first instance of them being portrayed this way, alongside warriors and aristocrats as they make their way to the sites, enjoying the local delights, and worship on the sacred grounds. Together with the novel subject material, a new artistic language was created— schematic, colorful and bold. We begin by locating sankei mandara’s artistic roots and influences and then proceed to investigate the individual mandara devoted to three sacred sites: Mt. Fuji, Kiyomizudera and Ise Shrine (a sacred mountain, temple and shrine, respectively). -

Esoteric Buddhist Traditions in Medieval Japan Matthew D
issn 0304-1042 Japanese Journal of Religious Studies volume 47, no. 1 2020 articles 1 Editor’s Introduction Esoteric Buddhist Traditions in Medieval Japan Matthew D. McMullen 11 Buddhist Temple Networks in Medieval Japan Daigoji, Mt. Kōya, and the Miwa Lineage Anna Andreeva 43 The Mountain as Mandala Kūkai’s Founding of Mt. Kōya Ethan Bushelle 85 The Doctrinal Origins of Embryology in the Shingon School Kameyama Takahiko 103 “Deviant Teachings” The Tachikawa Lineage as a Moving Concept in Japanese Buddhism Gaétan Rappo 135 Nenbutsu Orthodoxies in Medieval Japan Aaron P. Proffitt 161 The Making of an Esoteric Deity Sannō Discourse in the Keiran shūyōshū Yeonjoo Park reviews 177 Gaétan Rappo, Rhétoriques de l’hérésie dans le Japon médiéval et moderne. Le moine Monkan (1278–1357) et sa réputation posthume Steven Trenson 183 Anna Andreeva, Assembling Shinto: Buddhist Approaches to Kami Worship in Medieval Japan Or Porath 187 Contributors Japanese Journal of Religious Studies 47/1: 1–10 © 2020 Nanzan Institute for Religion and Culture dx.doi.org/10.18874/jjrs.47.1.2020.1-10 Matthew D. McMullen Editor’s Introduction Esoteric Buddhist Traditions in Medieval Japan he term “esoteric Buddhism” (mikkyō 密教) tends to invoke images often considered obscene to a modern audience. Such popular impres- sions may include artworks insinuating copulation between wrathful Tdeities that portend to convey a profound and hidden meaning, or mysterious rites involving sexual symbolism and the summoning of otherworldly powers to execute acts of violence on behalf of a patron. Similar to tantric Buddhism elsewhere in Asia, many of the popular representations of such imagery can be dismissed as modern interpretations and constructs (White 2000, 4–5; Wede- meyer 2013, 18–36). -
Japanization in the Field of Classical Chinese Dictionaries
Title Japanization in the Field of Classical Chinese Dictionaries Author(s) Ikeda, Shoju Citation Journal of the Graduate School of Letters, 6, 15-25 Issue Date 2011-03 Doc URL http://hdl.handle.net/2115/44945 Type bulletin (article) File Information JGSL6-2.pdf Instructions for use Hokkaido University Collection of Scholarly and Academic Papers : HUSCAP Journal of the Graduate School of Letters,Hokkaido University Vol.6;pp.15-25,March 2011 15 Japanization in the Field of Classical Chinese Dictionaries Shoju IKEDA Abstract:How did dictionaries arranged by radical undergo Japanization?In the following I shall take up for consideration the Tenrei bansh썚omeigi,Shinsenjiky썚o,and Ruiju my썚ogi sh썚oand consider this question by examining in particular their relationship with the original version of the Chinese Yupian,compiled in 543 by Gu Yewang of the Liang.There is much that needs to be said about early Japanese dictionaries.In this paper I have focused on their relationship with the Yupian and have discussed questions such as its position as a source among Buddhist monks and its connections with questions pertaining to radicals,in particular the manner in which the arrangement of characters under individual radicals in the Yupian was modified. (Received on December 7,2010) 1.Dictionaries Arranged According to the Shape,Sound and Meaning of Chinese Characters and the Compilation of Early Dictionaries in Japan When considered in light of extant dictionaries,it would seem that dictionaries arranged by radical or classifier(shape)appeared first,followed by dictionaries arranged by meaning,and that dictionaries arranged by pronunciation(sound)came some time later. -

Powerful Warriors and Influential Clergy Interaction and Conflict Between the Kamakura Bakufu and Religious Institutions
UNIVERSITY OF HAWAllllBRARI Powerful Warriors and Influential Clergy Interaction and Conflict between the Kamakura Bakufu and Religious Institutions A DISSERTATION SUBMITTED TO THE GRADUATE DIVISION OF THE UNIVERSITY OF HAWAI'I IN PARTIAL FULFILLMENT OF THE REQUIREMENTS FOR THE DEGREE OF DOCTOR OF PHILOSOPHY IN HISTORY MAY 2003 By Roy Ron Dissertation Committee: H. Paul Varley, Chairperson George J. Tanabe, Jr. Edward Davis Sharon A. Minichiello Robert Huey ACKNOWLEDGMENTS Writing a doctoral dissertation is quite an endeavor. What makes this endeavor possible is advice and support we get from teachers, friends, and family. The five members of my doctoral committee deserve many thanks for their patience and support. Special thanks go to Professor George Tanabe for stimulating discussions on Kamakura Buddhism, and at times, on human nature. But as every doctoral candidate knows, it is the doctoral advisor who is most influential. In that respect, I was truly fortunate to have Professor Paul Varley as my advisor. His sharp scholarly criticism was wonderfully balanced by his kindness and continuous support. I can only wish others have such an advisor. Professors Fred Notehelfer and Will Bodiford at UCLA, and Jeffrey Mass at Stanford, greatly influenced my development as a scholar. Professor Mass, who first introduced me to the complex world of medieval documents and Kamakura institutions, continued to encourage me until shortly before his untimely death. I would like to extend my deepest gratitude to them. In Japan, I would like to extend my appreciation and gratitude to Professors Imai Masaharu and Hayashi Yuzuru for their time, patience, and most valuable guidance. -

The Hachiman Cult and the Dokyo Incident Author(S): Ross Bender Source: Monumenta Nipponica, Vol
The Hachiman Cult and the Dokyo Incident Author(s): Ross Bender Source: Monumenta Nipponica, Vol. 34, No. 2 (Summer, 1979), pp. 125-153 Published by: Sophia University Stable URL: http://www.jstor.org/stable/2384320 Accessed: 17-03-2016 17:03 UTC Your use of the JSTOR archive indicates your acceptance of the Terms & Conditions of Use, available at http://www.jstor.org/page/ info/about/policies/terms.jsp JSTOR is a not-for-profit service that helps scholars, researchers, and students discover, use, and build upon a wide range of content in a trusted digital archive. We use information technology and tools to increase productivity and facilitate new forms of scholarship. For more information about JSTOR, please contact [email protected]. Sophia University is collaborating with JSTOR to digitize, preserve and extend access to Monumenta Nipponica. http://www.jstor.org This content downloaded from 77.80.42.241 on Thu, 17 Mar 2016 17:03:08 UTC All use subject to JSTOR Terms and Conditions The Hachiman Cult and the D6ky6 Incident by Ross BENDER XO I NE of the gravest assaults ever made on the Japanese imperial institution was launched by the Buddhist priest D6ky6' in the 760s. Dokyo, who came from a clan of the low-ranking provincial aristocracy, gained the affection of the retired Empress K6ken2 in 761 and proceeded to gather political power to himself; by the end of the decade he stood as the paramount figure in the court bureaucracy and had already begun to usurp imperial prerogatives. It was in 769 that an oracle from the shrine of Hachiman in Kyushu was reported to Nara: the god prophesied peace in the realm if Dokyo were proclaimed em- peror. -

The Durability of the Bakuhan Taisei Is Stunning
Tokugawa Yoshimune versus Tokugawa Muneharu: Rival Visions of Benevolent Rule by Tim Ervin Cooper III A dissertation submitted in partial satisfaction of the Requirements for the degree of Doctor of Philosophy in History in the Graduate Division of the University of California, Berkeley Committee in charge: Professor Mary Elizabeth Berry, Chair Professor Irwin Scheiner Professor Susan Matisoff Fall 2010 Abstract Tokugawa Yoshimune versus Tokugawa Muneharu: Rival Visions of Benevolent Rule by Tim Ervin Cooper III Doctor of Philosophy in History University of California, Berkeley Professor Mary Elizabeth Berry, Chair This dissertation examines the political rivalry between the eighth Tokugawa shogun, Yoshimune (1684‐1751, r. 1716‐45), and his cousin, the daimyo lord of Owari domain, Tokugawa Muneharu (1696‐1764, r. 1730‐39). For nearly a decade, Muneharu ruled Owari domain in a manner that directly contravened the policies and edicts of his cousin, the shogun. Muneharu ignored admonishments of his behavior, and he openly criticized the shogun’s Kyōhō era (1716‐36) reforms for the hardship that they brought people throughout Japan. Muneharu’s flamboyance and visibility transgressed traditional status boundaries between rulers and their subjects, and his lenient economic and social policies allowed commoners to enjoy the pleasures and profits of Nagoya entertainment districts that were expanding in response to the Owari lord’s personal fondness for the floating world. Ultimately, Muneharu’s fiscal extravagance and moral lenience—benevolent rule (jinsei), as he defined it—bankrupted domain coffers and led to his removal from office by Yoshimune. Although Muneharu’s challenge to Yoshimune’s political authority ended in failure, it nevertheless reveals the important role that competing notions of benevolence (jin) were coming to play in the rhetoric of Tokugawa rulership. -

Creating Heresy: (Mis)Representation, Fabrication, and the Tachikawa-Ryū
Creating Heresy: (Mis)representation, Fabrication, and the Tachikawa-ryū Takuya Hino Submitted in partial fulfillment of the Requirement for the degree of Doctor of Philosophy in the Graduate School of Arts and Sciences COLUMBIA UNIVERSITY 2012 © 2012 Takuya Hino All rights reserved ABSTRACT Creating Heresy: (Mis)representation, Fabrication, and the Tachikawa-ryū Takuya Hino In this dissertation I provide a detailed analysis of the role played by the Tachikawa-ryū in the development of Japanese esoteric Buddhist doctrine during the medieval period (900-1200). In doing so, I seek to challenge currently held, inaccurate views of the role played by this tradition in the history of Japanese esoteric Buddhism and Japanese religion more generally. The Tachikawa-ryū, which has yet to receive sustained attention in English-language scholarship, began in the twelfth century and later came to be denounced as heretical by mainstream Buddhist institutions. The project will be divided into four sections: three of these will each focus on a different chronological stage in the development of the Tachikawa-ryū, while the introduction will address the portrayal of this tradition in twentieth-century scholarship. TABLE OF CONTENTS List of Abbreviations……………………………………………………………………………...ii Acknowledgements………………………………………………………………………………iii Dedication……………………………………………………………………………….………..vi Preface…………………………………………………………………………………………...vii Introduction………………………………………………………………………….…………….1 Chapter 1: Genealogy of a Divination Transmission……………………………………….……40 Chapter -
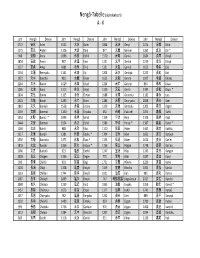
Nengo Alpha.Xlsx
Nengô‐Tabelle (alphabetisch) A ‐ K Jahr Nengō Devise Jahr Nengō Devise Jahr Nengō Devise Jahr Nengō Devise 1772 安永 An'ei 1521 大永 Daiei 1864 元治 Genji 1074 承保 Jōhō 1175 安元 Angen 1126 大治 Daiji 877 元慶 Genkei 1362 貞治 Jōji * 968 安和 Anna 1096 永長 Eichō 1570 元亀 Genki 1684 貞享 Jōkyō 1854 安政 Ansei 987 永延 Eien 1321 元亨 Genkō 1219 承久 Jōkyū 1227 安貞 Antei 1081 永保 Eihō 1331 元弘 Genkō 1652 承応 Jōō 1234 文暦 Benryaku 1141 永治 Eiji 1204 元久 Genkyū 1222 貞応 Jōō 1372 文中 Bunchū 983 永観 Eikan 1615 元和 Genna 1097 承徳 Jōtoku 1264 文永 Bun'ei 1429 永享 Eikyō 1224 元仁 Gennin 834 承和 Jōwa 1185 文治 Bunji 1113 永久 Eikyū 1319 元応 Gen'ō 1345 貞和 Jōwa * 1804 文化 Bunka 1165 永万 Eiman 1688 元禄 Genroku 1182 寿永 Juei 1501 文亀 Bunki 1293 永仁 Einin 1184 元暦 Genryaku 1848 嘉永 Kaei 1861 文久 Bunkyū 1558 永禄 Eiroku 1329 元徳 Gentoku 1303 嘉元 Kagen 1469 文明 Bunmei 1160 永暦 Eiryaku 650 白雉 Hakuchi 1094 嘉保 Kahō 1352 文和 Bunna * 1046 永承 Eishō 1159 平治 Heiji 1106 嘉承 Kajō 1444 文安 Bunnan 1504 永正 Eishō 1989 平成 Heisei * 1387 嘉慶 Kakei * 1260 文応 Bun'ō 988 永祚 Eiso 1120 保安 Hōan 1441 嘉吉 Kakitsu 1317 文保 Bunpō 1381 永徳 Eitoku * 1704 宝永 Hōei 1661 寛文 Kanbun 1592 文禄 Bunroku 1375 永和 Eiwa * 1135 保延 Hōen 1624 寛永 Kan'ei 1818 文政 Bunsei 1356 延文 Enbun * 1156 保元 Hōgen 1748 寛延 Kan'en 1466 文正 Bunshō 923 延長 Enchō 1247 宝治 Hōji 1243 寛元 Kangen 1028 長元 Chōgen 1336 延元 Engen 770 宝亀 Hōki 1087 寛治 Kanji 999 長保 Chōhō 901 延喜 Engi 1751 宝暦 Hōreki 1229 寛喜 Kanki 1104 長治 Chōji 1308 延慶 Enkyō 1449 宝徳 Hōtoku 1004 寛弘 Kankō 1163 長寛 Chōkan 1744 延享 Enkyō 1021 治安 Jian 985 寛和 Kanna 1487 長享 Chōkyō 1069 延久 Enkyū 767 神護景雲 Jingo‐keiun 1017 寛仁 Kannin 1040 長久 Chōkyū 1239 延応 En'ō -

Political and Ritual Usages of Portraits of Japanese
POLITICAL AND RITUAL USAGES OF PORTRAITS OF JAPANESE EMPERORS IN EIGHTEENTH AND NINETEENTH CENTURIES by Yuki Morishima B.A., University of Washington, 1996 B.F.A., University of Washington, 1996 M.S., Boston University, 1999 M.A., University of Pittsburgh, 2007 Submitted to the Graduate Faculty of the Kenneth P. Dietrich School of Arts and Sciences in partial fulfillment of the requirements for the degree of Doctor of Philosophy University of Pittsburgh 2013 UNIVERSITY OF PITTSBURGH DIETRICH SCHOOL OF ARTS AND SCIENCES This dissertation was presented by Yuki Morishima It was defended on November 13, 2013 and approved by Katheryn Linduff, Professor, Art and Architecture Evelyn Rawski, Professor, History Kirk Savage, Professor, Art and Architecture Dissertation Advisor: Karen Gerhart, Professor, Art and Architecture ii Copyright © by Yuki Morishima 2013 iii POLITICAL AND RITUAL USAGES OF PORTRAITS OF JAPANESE EMPERORS IN EIGHTEENTH AND NINETEENTH CENTURIES Yuki Morishima, PhD University of Pittsburgh, 2013 This dissertation examines portraits of Japanese emperors from the pre-modern Edo period (1603-1868) through the modern Meiji period (1868-1912) by questioning how the socio- political context influenced the production of imperial portraits. Prior to Western influence, pre- modern Japanese society viewed imperial portraits as religious objects for private, commemorative use; only imperial family members and close supporters viewed these portraits. The Confucian notion of filial piety and the Buddhist tradition of tsuizen influenced the production of these commemorative or mortuary portraits. By the Meiji period, however, Western portrait practice had affected how Japan perceived its imperial portraiture. Because the Meiji government socially and politically constructed the ideal role of Emperor Meiji and used the portrait as a means of propaganda to elevate the emperor to the status of a divinity, it instituted controlled public viewing of the images of Japanese emperors.