HISTORY of PRESENT ILLNESS ELEMENTS: Location Timing Quality Context Severity Modifying Factors Duration Associated Signs/Symptoms
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Generalized Edema Resulting from Mixed Intestinal Infection by Entamoebia Histolytica and E
Case Report JOJ Case Stud Volume 12 Issue 2 -April 2021 Copyright © All rights are reserved by Ajite Adebukola DOI: 10.19080/JOJCS.2021.12.555833 Generalized Edema Resulting from Mixed Intestinal Infection by Entamoebia Histolytica and E. Coli in a Nigerian Female Adolescent: A Case Report Ajite Adebukola1,2*, Oluwayemi Oludare1,2 and Fatunla Odunayo2 1Department of Paediatrics, Ekiti State University, Nigeria 2Department of Paediatrics, Ekiti State University Teaching Hospital, Nigeria Submission: March 15, 2021; Published: April 08, 2021 *Corresponding author: Ajite Adebukola, Consultant Paediatrician, Department of Paediatrics, Ekiti State University, Ado Ekiti, Nigeria Abstract Amoebiasis, a clinical condition caused by Entamoeba histolytica does not usually present with generalized oedema known as anarsarca. We present a case of an adolescent female Nigerian who was admitted on account of chronic diarrhea and anarsarca in a tertiary hospital, Southwest Nigeria. There was no proteinuria. She however had cyst of E. histolytica and growth of E. coli in her stool; she also had E. coli isolated in her urine. She had hypoproteinaemia (35.2g/L) and hypoalbuminaemia (21.3g/L) as well as hypokalemia (2.97mmol/L). Symptoms resolved Entamoeba histolytica and Escherichia coli bacteria may be responsible for the worse clinical manifestations of Amoebiasis and biochemical parameters normalized following treatment with Nitrofurantoin, Tinidazole and Ciprofloxacin. A mixed infection of Keywords: Amoebiasis; Chronic diarrhea; Hypoproteinaemia; Anasarca Introduction Amoebiasis, caused by the protozoan Entamoeba histolytica of amenorrhoea. is an infection that frequently manifests clinically with symptoms recurrent generalized body swelling, and a seven-month history of abdominal pain, diarrhoea, dysentery and weight loss [1,2]. -

Ehrlichiosis and Anaplasmosis Are Tick-Borne Diseases Caused by Obligate Anaplasmosis: Intracellular Bacteria in the Genera Ehrlichia and Anaplasma
Ehrlichiosis and Importance Ehrlichiosis and anaplasmosis are tick-borne diseases caused by obligate Anaplasmosis: intracellular bacteria in the genera Ehrlichia and Anaplasma. These organisms are widespread in nature; the reservoir hosts include numerous wild animals, as well as Zoonotic Species some domesticated species. For many years, Ehrlichia and Anaplasma species have been known to cause illness in pets and livestock. The consequences of exposure vary Canine Monocytic Ehrlichiosis, from asymptomatic infections to severe, potentially fatal illness. Some organisms Canine Hemorrhagic Fever, have also been recognized as human pathogens since the 1980s and 1990s. Tropical Canine Pancytopenia, Etiology Tracker Dog Disease, Ehrlichiosis and anaplasmosis are caused by members of the genera Ehrlichia Canine Tick Typhus, and Anaplasma, respectively. Both genera contain small, pleomorphic, Gram negative, Nairobi Bleeding Disorder, obligate intracellular organisms, and belong to the family Anaplasmataceae, order Canine Granulocytic Ehrlichiosis, Rickettsiales. They are classified as α-proteobacteria. A number of Ehrlichia and Canine Granulocytic Anaplasmosis, Anaplasma species affect animals. A limited number of these organisms have also Equine Granulocytic Ehrlichiosis, been identified in people. Equine Granulocytic Anaplasmosis, Recent changes in taxonomy can make the nomenclature of the Anaplasmataceae Tick-borne Fever, and their diseases somewhat confusing. At one time, ehrlichiosis was a group of Pasture Fever, diseases caused by organisms that mostly replicated in membrane-bound cytoplasmic Human Monocytic Ehrlichiosis, vacuoles of leukocytes, and belonged to the genus Ehrlichia, tribe Ehrlichieae and Human Granulocytic Anaplasmosis, family Rickettsiaceae. The names of the diseases were often based on the host Human Granulocytic Ehrlichiosis, species, together with type of leukocyte most often infected. -

Practical Cardiac Auscultation
LWW/CCNQ LWWJ306-08 March 7, 2007 23:32 Char Count= Crit Care Nurs Q Vol. 30, No. 2, pp. 166–180 Copyright c 2007 Wolters Kluwer Health | Lippincott Williams & Wilkins Practical Cardiac Auscultation Daniel M. Shindler, MD, FACC This article focuses on the practical use of the stethoscope. The art of the cardiac physical exam- ination includes skillful auscultation. The article provides the author’s personal approach to the patient for the purpose of best hearing, recognizing, and interpreting heart sounds and murmurs. It should be used as a brief introduction to the art of auscultation. This article also attempts to illustrate heart sounds and murmurs by using words and letters to phonate the sounds, and by presenting practical clinical examples where auscultation clearly influences cardiac diagnosis and treatment. The clinical sections attempt to go beyond what is available in standard textbooks by providing information and stethoscope techniques that are valuable and useful at the bedside. Key words: auscultation, murmur, stethoscope HIS article focuses on the practical use mastered at the bedside. This article also at- T of the stethoscope. The art of the cardiac tempts to illustrate heart sounds and mur- physical examination includes skillful auscul- murs by using words and letters to phonate tation. Even in an era of advanced easily avail- the sounds, and by presenting practical clin- able technological bedside diagnostic tech- ical examples where auscultation clearly in- niques such as echocardiography, there is still fluences cardiac diagnosis and treatment. We an important role for the hands-on approach begin by discussing proper stethoscope selec- to the patient for the purpose of evaluat- tion and use. -

Mosby: Mosby's Nursing Video Skills
Mosby: Mosby's Nursing Video Skills Procedural Guideline for Assessing Apical Pulse Procedure Steps 1. Verify the health care provider’s orders. 2. Gather the necessary equipment and supplies. 3. Perform hand hygiene. 4. Provide for the patient’s privacy. 5. Introduce yourself to the patient and family if present. 6. Identify the patient using two identifiers. 7. Assess for factors that can affect the apical pulse rate and rhythm, such as medical history, disease processes, age, exercise, position changes, medications, temperature, or sympathetic stimulation. 8. Gloves are only worn if nurse will be in contact with bodily fluids or the patient is in protective precautions. 9. Help the patient into a supine or sitting position, and expose the sternum and the left side of the chest. 10. Locate the point of maximal impulse (PMI, or apical impulse). To do this, find the angle of Louis, which feels like a bony prominence just below the suprasternal notch. 11. Slide your fingers down each side of the angle to find the second intercostal space (ICS). Carefully move your fingers down the left side of the sternum to the fifth intercostal space and over to the left midclavicular line. 12. Feel the PMI as a light tap about 1 to 2 centimeters in diameter, reflecting the apex of the heart. 13. If the PMI is not where you would expect, as in a patient whose left ventricle is enlarged, inch your fingers along the fifth intercostal space until you feel the PMI. 14. Remember where you felt the PMI: over the apex of the heart in the fifth intercostal space at the left midclavicular line. -

Review of Systems
code: GF004 REVIEW OF SYSTEMS First Name Middle Name / MI Last Name Check the box if you are currently experiencing any of the following : General Skin Respiratory Arthritis/Rheumatism Abnormal Pigmentation Any Lung Troubles Back Pain (recurrent) Boils Asthma or Wheezing Bone Fracture Brittle Nails Bronchitis Cancer Dry Skin Chronic or Frequent Cough Diabetes Eczema Difficulty Breathing Foot Pain Frequent infections Pleurisy or Pneumonia Gout Hair/Nail changes Spitting up Blood Headaches/Migraines Hives Trouble Breathing Joint Injury Itching URI (Cold) Now Memory Loss Jaundice None Muscle Weakness Psoriasis Numbness/Tingling Rash Obesity Skin Disease Osteoporosis None Rheumatic Fever Weight Gain/Loss None Cardiovascular Gastrointestinal Eyes - Ears - Nose - Throat/Mouth Awakening in the night smothering Abdominal Pain Blurring Chest Pain or Angina Appetite Changes Double Vision Congestive Heart Failure Black Stools Eye Disease or Injury Cyanosis (blue skin) Bleeding with Bowel Movements Eye Pain/Discharge Difficulty walking two blocks Blood in Vomit Glasses Edema/Swelling of Hands, Feet or Ankles Chrohn’s Disease/Colitis Glaucoma Heart Attacks Constipation Itchy Eyes Heart Murmur Cramping or pain in the Abdomen Vision changes Heart Trouble Difficulty Swallowing Ear Disease High Blood Pressure Diverticulosis Ear Infections Irregular Heartbeat Frequent Diarrhea Ears ringing Pain in legs Gallbladder Disease Hearing problems Palpitations Gas/Bloating Impaired Hearing Poor Circulation Heartburn or Indigestion Chronic Sinus Trouble Shortness -

Review of Systems – Return Visit Have You Had Any Problems Related to the Following Symptoms in the Past Month? Circle Yes Or No
REVIEW OF SYSTEMS – RETURN VISIT HAVE YOU HAD ANY PROBLEMS RELATED TO THE FOLLOWING SYMPTOMS IN THE PAST MONTH? CIRCLE YES OR NO Today’s Date: ______________ Name: _______________________________ Date of Birth: __________________ GENERAL GENITOURINARY Fatigue Y N Blood in Urine Y N Fever / Chills Y N Menstrual Irregularity Y N Night Sweats Y N Painful Menstrual Cycle Y N Weight Gain Y N Vaginal Discharge Y N Weight Loss Y N Vaginal Dryness Y N EYES Vaginal Itching Y N Vision Changes Y N Painful Sex Y N EAR, NOSE, & THROAT SKIN Hearing Loss Y N Hair Loss Y N Runny Nose Y N New Skin Lesions Y N Ringing in Ears Y N Rash Y N Sinus Problem Y N Pigmentation Change Y N Sore Throat Y N NEUROLOGIC BREAST Headache Y N Breast Lump Y N Muscular Weakness Y N Tenderness Y N Tingling or Numbness Y N Nipple Discharge Y N Memory Difficulties Y N CARDIOVASCULAR MUSCULOSKELETAL Chest Pain Y N Back Pain Y N Swelling in Legs Y N Limitation of Motion Y N Palpitations Y N Joint Pain Y N Fainting Y N Muscle Pain Y N Irregular Heart Beat Y N ENDOCRINE RESPIRATORY Cold Intolerance Y N Cough Y N Heat Intolerance Y N Shortness of Breath Y N Excessive Thirst Y N Post Nasal Drip Y N Excessive Amount of Urine Y N Wheezing Y N PSYCHOLOGY GASTROINTESTINAL Difficulty Sleeping Y N Abdominal Pain Y N Depression Y N Constipation Y N Anxiety Y N Diarrhea Y N Suicidal Thoughts Y N Hemorrhoids Y N HEMATOLOGIC / LYMPHATIC Nausea Y N Easy Bruising Y N Vomiting Y N Easy Bleeding Y N GENITOURINARY Swollen Lymph Glands Y N Burning with Urination Y N ALLERGY / IMMUNOLOGY Urinary -

How to Recognize a Suspected Cardiac Defect in the Neonate
Neonatal Nursing Education Brief: How to Recognize a Suspected Cardiac Defect in the Neonate https://www.seattlechildrens.org/healthcare- professionals/education/continuing-medical-nursing-education/neonatal- nursing-education-briefs/ Cardiac defects are commonly seen and are the leading cause of death in the neonate. Prompt suspicion and recognition of congenital heart defects can improve outcomes. An ECHO is not needed to make a diagnosis. Cardiac defects, congenital heart defects, NICU, cardiac assessment How to Recognize a Suspected Cardiac Defect in the Neonate Purpose and Goal: CNEP # 2092 • Understand the signs of congenital heart defects in the neonate. • Learn to recognize and detect heart defects in the neonate. None of the planners, faculty or content specialists has any conflict of interest or will be presenting any off-label product use. This presentation has no commercial support or sponsorship, nor is it co-sponsored. Requirements for successful completion: • Successfully complete the post-test • Complete the evaluation form Date • December 2018 – December 2020 Learning Objectives • Describe the risk factors for congenital heart defects. • Describe the clinical features of suspected heart defects. • Identify 2 approaches for recognizing congenital heart defects. Introduction • Congenital heart defects may be seen at birth • They are the most common congenital defect • They are the leading cause of neonatal death • Many neonates present with symptoms at birth • Some may present after discharge • Early recognition of CHD -

Anorexia/Cachexia Heart Failure Symptom Management Guideline for Adults, Age 19 and Older in British Columbia
Anorexia/Cachexia Heart Failure Symptom Management Guideline For adults, age 19 and older in British Columbia What is anorexia? Anorexia is a syndrome characterized by some or all of the following symptoms: loss of appetite, nausea, early satiety, weakness, fatigue, food aversion, and significant physical and/or psychological symptoms. Causes of anorexia are multifactorial and include fatigue, dyspnea, medication side-effects, nausea, depression, anxiety and sodium restricted diets, which may all be found in patients with heart failure. What is cachexia? Cachexia is a syndrome characterized by severe body weight, fat and muscle loss and increased protein catabolism due to underlying disease. The prevalence of cachexia is 16–42% in the heart failure population and is associated with a 50%, 18 month mortality risk independent of variables such as ejection fraction, age and functional ability. How is cachexia diagnosed? Chronic condition with >5% weight loss in <12 months; or body mass index (BMI) <20kg/m2; and 3 out of 5 additional criteria: 1) Fatigue, 2) Decreased muscle strength, 3) Anorexia, 4) Low muscle mass, 5) Abnormal biochemistry *Blood testing to diagnose cachexia in advanced stages of disease is not advocated. Reminder: Malnutrition also affects prognosis in patients with heart failure and is often found in early transitions of the disease. However this symptom management guideline will focus on the assessment and treatment of anorexia and cachexia. Approach to Managing Anorexia/Cachexia Assessment History: When did weight loss begin? How much weight was lost? Obtain baseline (dry) weight. How is [the patients] appetite? What do they eat or drink on a typical day? How has weight loss affected mood? Ask about: nausea, early satiety, dyspnea, poor oral hygiene, dysphagia, malabsorption, bowel habits. -

Cutaneous Manifestations of Abdominal Arteriovenous Fistulas
Cutaneous Manifestations of Abdominal Arteriovenous Fistulas Jessica Scruggs, MD; Daniel D. Bennett, MD Abdominal arteriovenous (A-V) fistulas may be edema.1-3 We report a case of abdominal aortocaval spontaneous or secondary to trauma. The clini- fistula presenting with lower extremity edema, ery- cal manifestations of abdominal A-V fistulas are thema, and cyanosis that had been previously diag- variable, but cutaneous findings are common and nosed as venous stasis dermatitis. may be suggestive of the diagnosis. Cutaneous physical examination findings consistent with Case Report abdominal A-V fistula include lower extremity A 51-year-old woman presented to the emergency edema with cyanosis, pulsatile varicose veins, department with worsening lower extremity swelling, and scrotal edema. redness, and pain. Her medical history included a We present a patient admitted to the hospital diagnosis of congestive heart failure, chronic obstruc- with lower extremity swelling, discoloration, and tive pulmonary disease, hepatitis C virus, tobacco pain, as well as renal insufficiency. During a prior abuse, and polysubstance dependence. Swelling, red- hospitalization she was diagnosed with venous ness, and pain of her legs developed several years stasis dermatitis; however, CUTISher physical examina- prior, and during a prior hospitalization she had been tion findings were not consistent with that diagno- diagnosed with chronic venous stasis dermatitis as sis. Imaging studies identified and characterized well as neurodermatitis. an abdominal aortocaval fistula. We propose that On admission, the patient had cool lower extremi- dermatologists add abdominal A-V fistula to the ties associated with discoloration and many crusted differential diagnosis of patients presenting with ulcerations. Aside from obesity, her abdominal exam- lower extremity edema with cyanosis, and we ination was unremarkable and no bruits were noted. -

Bradycardia; Pulse Present
Bradycardia; Pulse Present History Signs and Symptoms Differential • Past medical history • HR < 60/min with hypotension, acute • Acute myocardial infarction • Medications altered mental status, chest pain, • Hypoxia / Hypothermia • Beta-Blockers acute CHF, seizures, syncope, or • Pacemaker failure • Calcium channel blockers shock secondary to bradycardia • Sinus bradycardia • Clonidine • Chest pain • Head injury (elevated ICP) or Stroke • Digoxin • Respiratory distress • Spinal cord lesion • Pacemaker • Hypotension or Shock • Sick sinus syndrome • Altered mental status • AV blocks (1°, 2°, or 3°) • Syncope • Overdose Heart Rate < 60 / min and Symptomatic: Exit to Hypotension, Acute AMS, Ischemic Chest Pain, Appropriate NO Acute CHF, Seizures, Syncope, or Shock Protocol(s) secondary to bradycardia Typically HR < 50 / min YES Airway Protocol(s) AR 1, 2, 3 if indicated Respiratory Distress Reversible Causes Protocol AR 4 if indicated Hypovolemia Hypoxia Chest Pain: Cardiac and STEMI Section Cardiac Protocol Adult Protocol AC 4 Hydrogen ion (acidosis) if indicated Hypothermia Hypo / Hyperkalemia Search for Reversible Causes B Tension pneumothorax 12 Lead ECG Procedure Tamponade; cardiac Toxins Suspected Beta- IV / IO Protocol UP 6 Thrombosis; pulmonary Blocker or Calcium P Cardiac Monitor (PE) Channel Blocker Thrombosis; coronary (MI) A Follow Overdose/ Toxic Ingestion Protocol TE 7 P If No Improvement Transcutaneous Pacing Procedure P (Consider earlier in 2nd or 3rd AVB) Notify Destination or Contact Medical Control Revised AC 2 01/01/2021 Any local EMS System changes to this document must follow the NC OEMS Protocol Change Policy and be approved by OEMS 1 Bradycardia; Pulse Present Adult Cardiac Adult Section Protocol Pearls • Recommended Exam: Mental Status, HEENT, Skin, Heart, Lungs, Abdomen, Back, Extremities, Neuro • Identifying signs and symptoms of poor perfusion caused by bradycardia are paramount. -
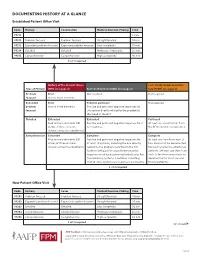
Documenting History at a Glance
DOCUMENTING HISTORY AT A GLANCE Established Patient Office Visit Code History Examination Medical Decision-Making Time 99211 — — — 5 min. 99212 Problem focused Problem focused Straightforward 10 min. 99213 Expanded problem focused Expanded problem focused Low complexity 15 min. 99214 Detailed Detailed Moderate complexity 25 min. 99215 Comprehensive Comprehensive High complexity 40 min. 2 of 3 required History of the Present Illness Past, Family and/or Social His- Type of History (HPI) (see page 2) Review of Systems (ROS) (see page 2) tory (PFSH) (see page 2) Problem Brief Not required Not required focused One to three elements Expanded Brief Problem pertinent Not required problem One to three elements Positive and pertinent negative responses for focused the system directly related to the problem(s) identified in the HPI. Detailed Extended Extended Pertinent Four or more elements (OR Positive and pertinent negative responses for 2 At least one specific item from status of three or more to 9 systems. the PFSH must be documented. chronic or inactive conditions) Comprehensive Extended Complete Complete Four or more elements (OR Positive and pertinent negative responses for At least one item from each of status of three or more at least 10 systems, including the one directly two areas must be documented chronic or inactive conditions) related to the problem identified in the HPI. for most services to established Systems with positive or pertinent negative patients. (At least one item from responses must be documented individually. For each of the three areas must be the remaining systems, a notation indicating documented for most services that all other systems are negative is permissible. -

Arrhythmia What Is It?
Arrhythmia What is it? Most of us have felt our heart race or skip a beat. It’s fairly normal every once and a while. But for some people, it’s a sign of arrhythmia – a disorder of your heart rate or rhythm – that needs to be checked out by a specialist. If you have an arrhythmia (there are multiple types), your heart either beats: • too fast • too slow or • with an irregular pattern Did You Know? This change in your heart rhythm is usually caused by a “glitch” Our heart beats an average of in your heart’s electrical activity, which tells the heart when to 70 to 80 times a minute and contract and pump blood to the body. Your heart doesn’t beat over 100,000 times a day! It’s with the regularity of a Swiss watch, and many factors can cause no wonder millions of people an irregularity. notice palpitations such as skipping a beat, fluttering or a Some of these factors include: racing heart. • having had a heart attack • having heart failure • blood chemistry imbalances • abnormal hormone levels • alcohol, caffeine and other substances or medicines • a variety of inherited abnormalities 8 Tips for Staying Heart Healthy with Arrhythmias Living with an arrhythmia varies tremendously from one person to the next. It will depend on the type of arrhythmia you have, how serious it is and the recommended treatment. Some people can take a single medication to correct their heart’s rhythm; others undergo electrophysiology studies or require a pacemaker or implantable defibrillator. No matter what kind of arrhythmia you have, there are things you can do to keep your heart healthy and ticking as it should.