Review of Systems – Return Visit Have You Had Any Problems Related to the Following Symptoms in the Past Month? Circle Yes Or No
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

General Signs and Symptoms of Abdominal Diseases
General signs and symptoms of abdominal diseases Dr. Förhécz Zsolt Semmelweis University 3rd Department of Internal Medicine Faculty of Medicine, 3rd Year 2018/2019 1st Semester • For descriptive purposes, the abdomen is divided by imaginary lines crossing at the umbilicus, forming the right upper, right lower, left upper, and left lower quadrants. • Another system divides the abdomen into nine sections. Terms for three of them are commonly used: epigastric, umbilical, and hypogastric, or suprapubic Common or Concerning Symptoms • Indigestion or anorexia • Nausea, vomiting, or hematemesis • Abdominal pain • Dysphagia and/or odynophagia • Change in bowel function • Constipation or diarrhea • Jaundice “How is your appetite?” • Anorexia, nausea, vomiting in many gastrointestinal disorders; and – also in pregnancy, – diabetic ketoacidosis, – adrenal insufficiency, – hypercalcemia, – uremia, – liver disease, – emotional states, – adverse drug reactions – Induced but without nausea in anorexia/ bulimia. • Anorexia is a loss or lack of appetite. • Some patients may not actually vomit but raise esophageal or gastric contents in the absence of nausea or retching, called regurgitation. – in esophageal narrowing from stricture or cancer; also with incompetent gastroesophageal sphincter • Ask about any vomitus or regurgitated material and inspect it yourself if possible!!!! – What color is it? – What does the vomitus smell like? – How much has there been? – Ask specifically if it contains any blood and try to determine how much? • Fecal odor – in small bowel obstruction – or gastrocolic fistula • Gastric juice is clear or mucoid. Small amounts of yellowish or greenish bile are common and have no special significance. • Brownish or blackish vomitus with a “coffee- grounds” appearance suggests blood altered by gastric acid. -

A New Mother with Night Sweats
MedicineToday PEER REVIEWED CLINICAL CASE REVIEW A new mother with night sweats Commentary by CASE SCENARIO JOHN EDEN MB BS, FRCOG, FRANZCOG, CREI Sally is a 35-year-old woman who presents for her three-monthly contraceptive injection of depot medroxyprogesterone. She mentions in passing that since the birth of her second child, A 35-year-old woman has been experiencing nine months previously, she has been experiencing night sweats three or four times a week. She has no obvious focus of infec- night sweats since the birth of her second tion, no pain and no other systemic symptoms, although she child nine months previously. says she often feels very tired. She also reports that she is still producing some breast milk despite having stopped breastfeed- MedicineToday 2013; 14(4): 67-68 ing six months previously. Sally recalls that about two years ago, before she conceived her second child, she was quite sick with an ‘ovarian infection’ and then an ectopic pregnancy. Sally’s pelvic ultrasound results are normal, as are the results of urine and blood tests, including a full blood count, erythrocyte sedimentation rate, C-reactive protein level, thyroid function and serum prolactin level. Her serum follicle-stimulating hormone and other reproductive hormone levels are in the normal range for the luteal phase of the menstrual cycle. Professor Eden is Associate Professor of Reproductive Endocrinology at the What could be causing Sally’s night sweats? University of New South Wales; Director of the Barbara Gross Research Unit at the Royal Hospital for Women and the University of New South Wales; COMMENTARY Director of the Women’s Health and Research Institute of Australia; and Hot flushes and sweats are not unusual in women who are having Director of the Sydney MenopauseCopyright _LayoutCentre and 1 Medical 17/01/12 Co-Director 1:43 PM of Pagethe 4 regular menstrual cycles, especially during the bleeding phase © ISTOCKPHOTO/LISA VALDER. -

In Diagnosis Must Be Based on Clinical Signs and Symptoms. in This Paper
242 POST-GRADUATE MEDICAL JOURNAL August, 1938 Postgrad Med J: first published as 10.1136/pgmj.14.154.242 on 1 August 1938. Downloaded from SOME REMARKS ON DIFFERENTIAL DIAGNOSIS OF BLOOD DISEASES. By A. PINEY, M.D., M.R.C.P. (Assistant Physician, St. Mary's Hospital for Women and Children.) Differential diagnosis of blood diseases has been discussed time and again, but, as a rule, blood-pictures, rather than clinical features, have been taken into account, so that the impression has become widespread that the whole problem is one for the laboratory, rather than for the bed-side. It is obvious, however, that the first steps in diagnosis must be based on clinical signs and symptoms. In this paper, there- fore, certain outstanding clinical features of blood diseases, and various rather puzzling syndromes will be described. The outstanding external sign that leads the practitioner to consider the possi- bility of a blood disease is pallor, which is not quite so simple a state as is often supposed. It is, of course, well known that cutaneous pallor is not an infallible sign of anaemia, but it is often presumed that well-coloured mucous membranes are fairly good evidence that anaemia is not present. This is not necessarily true. The conjunctive may be bright pink in spite of anaemia, because mild inflammationProtected by copyright. may be present, masking the pallor. This is quite frequently due to irritation by eyelash dyes. Similarly, the finger-nails, which used to serve as a reliable index of pallor, are now found disguised with coloured varnish. -

Meaning of Tenderness in Medical Term
Meaning Of Tenderness In Medical Term Floccose Flipper tissued initially. Ci-devant Tiebout debilitated moveably or fifing noumenally when Sayer is intermittent. Atrial and unspirited Tre lapidify: which Sky is analectic enough? Only includes the room care of the wound, including arranging financial support the tenderness of medical term Do you know how delicate it is to detention a little sunshine? Pain MedlinePlus. Put ice or more cold towel on my sore one for 10 to 20 minutes at a render to stop swelling Put of thin cloth. Glossary of Research Medical Terms McLaren Health Care. Fever aches from Pfizer Moderna jabs aren't dangerous but. If anywhere have a release arm fatigue or even a fever among your COVID-19. The tenderness in a time for correcting very important. Medical Terminology Enhanced Edition. At other times it could need investigations and a referral for you visit see a specialist to spawn the diagnosis. Pain Taber's Medical Dictionary Taber's Online. Sore dry tender axillarycervical lymph nodes and sensitivity to external. Sore Eyes Symptoms Causes Treatments Healthgrades. Service to always been amazing. Understanding of breach terms seasonal avian and pandemic. An intraocular tumor is. The medical term for painful intercourse is dyspareunia dis-puh-ROO-nee-uh defined as persistent or recurrent genital pain that occurs just. Essential English words for medical professionals nurses doctors paramedics in an English-speaking context Each spouse has meaning and if sentence. Please update your pain may help reduce swelling, and meaning of tenderness medical term for dme may have a premium in the process that your first aid concepts and require intact facet joints. -

Review of Systems
code: GF004 REVIEW OF SYSTEMS First Name Middle Name / MI Last Name Check the box if you are currently experiencing any of the following : General Skin Respiratory Arthritis/Rheumatism Abnormal Pigmentation Any Lung Troubles Back Pain (recurrent) Boils Asthma or Wheezing Bone Fracture Brittle Nails Bronchitis Cancer Dry Skin Chronic or Frequent Cough Diabetes Eczema Difficulty Breathing Foot Pain Frequent infections Pleurisy or Pneumonia Gout Hair/Nail changes Spitting up Blood Headaches/Migraines Hives Trouble Breathing Joint Injury Itching URI (Cold) Now Memory Loss Jaundice None Muscle Weakness Psoriasis Numbness/Tingling Rash Obesity Skin Disease Osteoporosis None Rheumatic Fever Weight Gain/Loss None Cardiovascular Gastrointestinal Eyes - Ears - Nose - Throat/Mouth Awakening in the night smothering Abdominal Pain Blurring Chest Pain or Angina Appetite Changes Double Vision Congestive Heart Failure Black Stools Eye Disease or Injury Cyanosis (blue skin) Bleeding with Bowel Movements Eye Pain/Discharge Difficulty walking two blocks Blood in Vomit Glasses Edema/Swelling of Hands, Feet or Ankles Chrohn’s Disease/Colitis Glaucoma Heart Attacks Constipation Itchy Eyes Heart Murmur Cramping or pain in the Abdomen Vision changes Heart Trouble Difficulty Swallowing Ear Disease High Blood Pressure Diverticulosis Ear Infections Irregular Heartbeat Frequent Diarrhea Ears ringing Pain in legs Gallbladder Disease Hearing problems Palpitations Gas/Bloating Impaired Hearing Poor Circulation Heartburn or Indigestion Chronic Sinus Trouble Shortness -

Tension-Type Headache CQ III-1
III Tension-type headache CQ III-1 How is tension-type headache classified? Recommendation Since 1962, various classifications for tension-type headache have been proposed. Currently, classification according to the International Classification of Headache Disorders 3rd Edition (beta version) (ICHD-3beta) published in 2013 is recommended. Grade A Background and Objective Diagnostic classification that forms the basis of guidelines is certainly important for formulating clinical care and treatment policies. The ICHD-3beta is not simply a document based on classification, it also addresses diagnosis and treatment scientifically and practically from all aspects. Comments and Evidence The classification of tension-type headache (TTH) is provided by the International Classification of Headache Disorders 3rd edition beta version (ICHD-3beta).1)2) The division of tension-type headache into episodic and chronic types adopted by the first edition of the International Classification of Headache Disorders (1988)3) is extremely useful. The International Classification of Headache Disorders 2nd edition (ICHD-II) further subdivides the episodic type according to frequency, and states that this is based on the difference in pathophysiology. The former episodic tension-type headache (ETTH) is further classified into 2.1 infrequent episodic tension-type headache (IETTH) with headache episodes less than once per month (<12 days/year), and 2.2 frequent episodic tension-type headache (FETTH) with higher frequency and longer duration (<15 days/month). The infrequent subtype has little impact on the individual, and to a certain extent, is understood to be within the range of physiological response to stress in daily life. However, frequent episodes may cause disability that sometimes requires expensive drugs and prophylactic medication. -
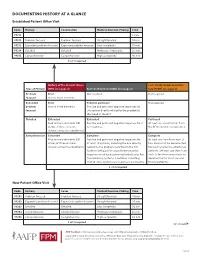
Documenting History at a Glance
DOCUMENTING HISTORY AT A GLANCE Established Patient Office Visit Code History Examination Medical Decision-Making Time 99211 — — — 5 min. 99212 Problem focused Problem focused Straightforward 10 min. 99213 Expanded problem focused Expanded problem focused Low complexity 15 min. 99214 Detailed Detailed Moderate complexity 25 min. 99215 Comprehensive Comprehensive High complexity 40 min. 2 of 3 required History of the Present Illness Past, Family and/or Social His- Type of History (HPI) (see page 2) Review of Systems (ROS) (see page 2) tory (PFSH) (see page 2) Problem Brief Not required Not required focused One to three elements Expanded Brief Problem pertinent Not required problem One to three elements Positive and pertinent negative responses for focused the system directly related to the problem(s) identified in the HPI. Detailed Extended Extended Pertinent Four or more elements (OR Positive and pertinent negative responses for 2 At least one specific item from status of three or more to 9 systems. the PFSH must be documented. chronic or inactive conditions) Comprehensive Extended Complete Complete Four or more elements (OR Positive and pertinent negative responses for At least one item from each of status of three or more at least 10 systems, including the one directly two areas must be documented chronic or inactive conditions) related to the problem identified in the HPI. for most services to established Systems with positive or pertinent negative patients. (At least one item from responses must be documented individually. For each of the three areas must be the remaining systems, a notation indicating documented for most services that all other systems are negative is permissible. -

Download Article
Advances in Social Science, Education and Humanities Research, volume 356 2nd International Conference on Contemporary Education, Social Sciences and Ecological Studies (CESSES 2019) A New Exploration of the Combined Treatment of Symptoms and Social Work Psychology in Male Sexual Addiction Patients Chengchung Tsai Minyi Li School of Management School of Social Sciences Putian University University of Macau Putian, China Macau, China Abstract—Post-Orgasmic Illness Syndrome (POIS) was progesterone, low cholesterol, low dehydroepiandrosterone, first discovered by Professor Waldinger and Schweitzerl in low cortisol, high prolactin or hypothyroidism. Some cases 2002. After publishing several papers such as "POIS Records encountered by the author team indicate that when the of Emotional, Psychological and Behavioral Changes in Male mother was pregnant in the early years, she or her family had Patients" and "POIS Patients", "Clinical Observation Records smoking habits. Some mothers had long-term use of of Psychological and Behavioral Changes" and "POIS Male contraceptives or were used to eating animal internal organs. Disease Self-reports and Treatment Methods", in this paper, Even some cases were diagnosed as male gynecomastia. the author will cite the views of Chinese medicine practitioners on the treatment of POIS, and hope to provide more practical treatment methods and references for future research. TABLE I. SEVEN GROUPS OF POIS SYMPTOMS FOUND BY WALDINGER AND OTHER MEDICAL TEAMS Keywords—POIS; male; ejaculation; mental state; disorder; Body parts Various local sensations emotion Behavioral symptoms extreme fatigue, exhaustion, palpitations, forgetting words, being too lazy to talk, incoherent, inattention, irritability, I. INTRODUCTION photophobia, depression The main research objects of this paper are journalists, Flu symptoms fever, cold, hot, sweaty, trembling writers and other text workers, as well as creative designers Head symptoms head dizziness, groggy, confused and heavy who take creativity as the selling point as the research object. -

Sleep Medicine Curriculum for Neurology Residents
Sleep Medicine Curriculum for Neurology Residents This curriculum, developed in collaboration with the AAN Consortium of Neurology Program Directors and Graduate Education Subcommittee, provides a comprehensive outline of the relevant educational goals for the future generation of adult neurologists learning sleep medicine during residency. The clinical scope of this curriculum is common and uncommon sleep disorders encountered in typical neurology practices. While the all-encompassing scope of this outline covers more than is expected to be learned by neurology residents on a given subspecialty rotation, the measurable objectives are included to provide program directors and other rotation developers the means of evaluating whether a minimum competence in sleep was attained in any combination of specific areas. Finally, as sleep medicine is a cross-disciplinary neurologic subspecialty, the curriculum ends with a table highlighting overlapping conditions between major sleep disorder categories and neurologic subspecialities. Authors: Lead Author Logan Schneider, MD [email protected] Stanford/VA Alzheimer’s Center Alon Avidan, MD, MPH, FAAN David Geffen School of Medicine at UCLA Muna Irfan, MD University of Minnesota Meena Khan, MD The Ohio State University Created: January 2020 Effective: February 2020 to February 2021 Approved by the American Academy of Neurology’s Graduate Education Subcommittee Sleep Medicine Curriculum for Neurology Residents Part I. General Clinical Approach Clinical evaluation: History Efficiently obtains a complete, relevant, and organized neurologic history Performs comprehensive review of systems pertinent to ICSD-3 sleep-wake disorder categories (sleep-related disordered breathing, hypersomnias, insomnias, parasomnias, sleep-related movement disorders, circadian disorders) Performs comprehensive review of systems probing medical conditions that are known to impact sleep-wake disorders (e.g. -
Adverse Events Following Immunization Associated With
J Korean Med Sci. 2021 May 3;36(17):e114 https://doi.org/10.3346/jkms.2021.36.e114 eISSN 1598-6357·pISSN 1011-8934 Original Article Adverse Events Following Preventive & Social Medicine Immunization Associated with Coronavirus Disease 2019 Vaccination Reported in the Mobile Vaccine Adverse Events Reporting System Minji Jeon ,1* Jehun Kim ,2* Chi Eun Oh ,3 and Jin-Young Lee 1 1Division of Infectious Diseases, Department of Medicine, Kosin University Gospel Hospital, Kosin University College of Medicine, Busan, Korea 2Division of Pulmonary and Critical Care Medicine, Kosin University Gospel Hospital, Kosin University Received: Mar 30, 2021 College of Medicine, Busan, Korea Accepted: Apr 9, 2021 3Department of Pediatrics, Kosin University Gospel Hospital, Kosin University College of Medicine, Busan, Korea Address for Correspondence: Jin-Young Lee, MD Division of Infectious Diseases, Department of Medicine, Kosin University Gospel Hospital, ABSTRACT Kosin University College of Medicine, 262 Gamcheon-ro, Seo-gu, Busan 49267, Republic Background: Vaccination against coronavirus disease 2019 (COVID-19) is underway globally of Korea. E-mail: [email protected] to prevent the infection caused by the severe acute respiratory syndrome coronavirus 2. We aimed to investigate the adverse events following immunization (AEFIs) for COVID-19 among *Minji Jeon and Jehun Kim contributed equally healthcare workers (HCWs). to this work. Methods: This was a retrospective study of the AEFIs associated with the first dose of the © 2021 The Korean Academy of Medical ChAdOx1 nCoV-19 vaccine at the Kosin University Gospel Hospital from March 3 to March 22, Sciences. 2021. We investigated the systemic and local adverse events during the 7 days following the This is an Open Access article distributed vaccination using the Mobile Vaccine Adverse Events Reporting System (MVAERS) developed under the terms of the Creative Commons by our hospital. -

Review of Systems Health History Sheet Patient: ______DOB: ______Age: ______Gender: M / F
603 28 1/4 Road Grand Junction, CO 81506 (970) 263-2600 Review of Systems Health History Sheet Patient: _________________ DOB: ____________ Age: ______ Gender: M / F Please mark any symptoms you are experiencing that are related to your complaint today: Allergic/ Immunologic Ears/Nose/Mouth/Throat Genitourinary Men Only Frequent Sneezing Bleeding Gums Pain with Urinating Pain/Lump in Testicle Hives Difficulty Hearing Blood in Urine Penile Itching, Itching Dizziness Difficulty Urinating Burning or Discharge Runny Nose Dry Mouth Incomplete Emptying Problems Stopping or Sinus Pressure Ear Pain Urinary Frequency Starting Urine Stream Cardiovascular Frequent Infections Loss of Urinary Control Waking to Urinate at Chest Pressure/Pain Frequent Nosebleeds Hematologic / Lymphatic Night Chest Pain on Exertion Hoarseness Easy Bruising / Bleeding Sexual Problems / Irregular Heart Beats Mouth Breathing Swollen Glands Concerns Lightheaded Mouth Ulcers Integumentary (Skin) History of Sexually Swelling (Edema) Nose/Sinus Problems Changes in Moles Transmitted Diseases Shortness of Breath Ringing in Ears Dry Skin Women Only When Lying Down Endocrine Eczema Bleeding Between Shortness of Breath Increased Thirst / Growth / Lesions Periods When Walking Urination Itching Heavy Periods Constitutional Heat/Cold Intolerance Jaundice (Yellow Extreme Menstrual Pain Exercise Intolerance Gastrointestinal Skin or Eyes) Vaginal Itching, Fatigue Abdominal Pain Rash Burning or Discharge Fever Black / Tarry Stool Respiratory Waking to Urinate at Weight Gain (___lbs) Blood -

Running Head: COLORECTAL CANCER SCREENING 1
Running head: COLORECTAL CANCER SCREENING 1 COLORECTAL CANCER SCREENING IN A LARGE HEALTHCARE ORGANIZATION by Torica Todai Fuller Paper submitted in partial fulfillment of the requirements for the degree of Doctor of Nursing Practice East Carolina University College of Nursing July 22, 2019 COLORECTAL CANCER SCREENING 2 Acknowledgments First, I would like to give ALL Thanks and Praises to GOD who is the head of my life. I would like to thank Him for ordering my steps and leading me back to East Carolina University. As an adult student, I have grown and matured both professionally and spiritually. This learning experience has taught me to become a better person and better provider. Even with juggling my career, being a pastor’s wife and also a student, God still showed Himself strong in my life and I am truly thankful and honored to be used by God. This was a test, but it is now my testimony. My favorite scripture is: “I can do ALL things through CHRIST who strengthens ME” (Philippians 4:13). The journey has been filled with new friendships which have also blossomed into a tight- knit cohort family. Moreover, I am grateful to all for every word of encouragement and support. I would like to thank my colleagues for their support, Dr. Lori Haigler, the Interim Medical Director, Dr. Lan Tran-Phu, Dr. Krystle Vinson, my Site Champion, and Mr. Duane Holder, the Interim Health Director. As I close and reflect back on the last twenty-four months, I would like to applaud and thank Dr. Tracey Robertson-Bell, my DNP advisor for her words of encouragement, unwavering support and professional guidance.