Review of Systems Health History Sheet Patient: ______DOB: ______Age: ______Gender: M / F
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Generalized Edema Resulting from Mixed Intestinal Infection by Entamoebia Histolytica and E
Case Report JOJ Case Stud Volume 12 Issue 2 -April 2021 Copyright © All rights are reserved by Ajite Adebukola DOI: 10.19080/JOJCS.2021.12.555833 Generalized Edema Resulting from Mixed Intestinal Infection by Entamoebia Histolytica and E. Coli in a Nigerian Female Adolescent: A Case Report Ajite Adebukola1,2*, Oluwayemi Oludare1,2 and Fatunla Odunayo2 1Department of Paediatrics, Ekiti State University, Nigeria 2Department of Paediatrics, Ekiti State University Teaching Hospital, Nigeria Submission: March 15, 2021; Published: April 08, 2021 *Corresponding author: Ajite Adebukola, Consultant Paediatrician, Department of Paediatrics, Ekiti State University, Ado Ekiti, Nigeria Abstract Amoebiasis, a clinical condition caused by Entamoeba histolytica does not usually present with generalized oedema known as anarsarca. We present a case of an adolescent female Nigerian who was admitted on account of chronic diarrhea and anarsarca in a tertiary hospital, Southwest Nigeria. There was no proteinuria. She however had cyst of E. histolytica and growth of E. coli in her stool; she also had E. coli isolated in her urine. She had hypoproteinaemia (35.2g/L) and hypoalbuminaemia (21.3g/L) as well as hypokalemia (2.97mmol/L). Symptoms resolved Entamoeba histolytica and Escherichia coli bacteria may be responsible for the worse clinical manifestations of Amoebiasis and biochemical parameters normalized following treatment with Nitrofurantoin, Tinidazole and Ciprofloxacin. A mixed infection of Keywords: Amoebiasis; Chronic diarrhea; Hypoproteinaemia; Anasarca Introduction Amoebiasis, caused by the protozoan Entamoeba histolytica of amenorrhoea. is an infection that frequently manifests clinically with symptoms recurrent generalized body swelling, and a seven-month history of abdominal pain, diarrhoea, dysentery and weight loss [1,2]. -

Review of Systems Form
Child’s name or label Since the last visit, how are your child’s symptoms? Better? Worse? The same? Please describe: Any new health problems, consultations, ER visits, hospital admissions, procedures or surgeries since your last visit? None Evaluations or tests done since the last visit: MRI EEG Blood work Child Study Team evaluation Neuropsychological testing ImPACT test Audiology Nutritionist consultation Questionnaires Physician Consultations:______________________ Other: ____________________ None If your child takes medications, please list the medications and doses here: 1.__________________________________________________ 4.__________________________________________ 2._________________________________________________ 5._________________________________________ 3.__________________________________________________ 6.__________________________________________ PEDS NEURO REVIEW OF SYSTEMS: Please list symptoms your child has since the last visit. Describe “yes” responses. NEUROLOGICAL KNOWN EYE CONDITIONS YES NO ___________________ HYPERACTIVITY YES NO ___________________ EAR, NOSE AND THROAT SEIZURES YES NO ___________________ HEARING LOSS OR DEFICIT YES NO ___________________ FAINTING YES NO ___________________ SLEEP APNEA YES NO ___________________ SNORING YES NO ___________________ CARDIOVASCULAR HEADACHES YES NO ___________________ RAPID OR IRREGULAR HEART BEAT YES NO ___________________ TICS YES NO ___________________ CHEST PAIN OR EXERCISE INTOLERANCE YES NO ___________________ INATTENTION -

NIH Public Access Author Manuscript Auton Neurosci
NIH Public Access Author Manuscript Auton Neurosci. Author manuscript; available in PMC 2016 March 01. NIH-PA Author ManuscriptPublished NIH-PA Author Manuscript in final edited NIH-PA Author Manuscript form as: Auton Neurosci. 2015 March ; 188: 86–89. doi:10.1016/j.autneu.2014.11.008. Exercise in the Postural Orthostatic Tachycardia Syndrome Qi Fu and Benjamin D. Levine Institute for Exercise and Environmental Medicine, Texas Health Presbyterian Hospital Dallas, The University of Texas Southwestern Medical Center, Dallas, TX, USA Abstract Patients with the Postural Orthostatic Tachycardia Syndrome (POTS) have orthostatic intolerance, as well as exercise intolerance. Peak oxygen uptake (VO2peak) is generally lower in these patients compared with healthy sedentary individuals, suggesting a lower physical fitness level. During acute exercise, POTS patients have an excessive increase in heart rate and reduced stroke volume for each level of absolute workload; however, when expressed at relative workload (%VO2peak), there is no difference in the heart rate response between patients and healthy individuals. The relationship between cardiac output and VO2 is similar between POTS patients and healthy individuals. Short-term (i.e., 3 months) exercise training increases cardiac size and mass, blood volume, and VO2peak in POTS patients. Exercise performance is improved after training. Specifically, stroke volume is greater and heart rate is lower at any given VO2 during exercise after training versus before training. Peak heart rate is the same but peak stroke volume and cardiac output are greater after training. Heart rate recovery from peak exercise is significantly faster after training, indicating an improvement in autonomic circulatory control. These results suggest that patients with POTS have no intrinsic abnormality of heart rate regulation during exercise. -

Ehrlichiosis and Anaplasmosis Are Tick-Borne Diseases Caused by Obligate Anaplasmosis: Intracellular Bacteria in the Genera Ehrlichia and Anaplasma
Ehrlichiosis and Importance Ehrlichiosis and anaplasmosis are tick-borne diseases caused by obligate Anaplasmosis: intracellular bacteria in the genera Ehrlichia and Anaplasma. These organisms are widespread in nature; the reservoir hosts include numerous wild animals, as well as Zoonotic Species some domesticated species. For many years, Ehrlichia and Anaplasma species have been known to cause illness in pets and livestock. The consequences of exposure vary Canine Monocytic Ehrlichiosis, from asymptomatic infections to severe, potentially fatal illness. Some organisms Canine Hemorrhagic Fever, have also been recognized as human pathogens since the 1980s and 1990s. Tropical Canine Pancytopenia, Etiology Tracker Dog Disease, Ehrlichiosis and anaplasmosis are caused by members of the genera Ehrlichia Canine Tick Typhus, and Anaplasma, respectively. Both genera contain small, pleomorphic, Gram negative, Nairobi Bleeding Disorder, obligate intracellular organisms, and belong to the family Anaplasmataceae, order Canine Granulocytic Ehrlichiosis, Rickettsiales. They are classified as α-proteobacteria. A number of Ehrlichia and Canine Granulocytic Anaplasmosis, Anaplasma species affect animals. A limited number of these organisms have also Equine Granulocytic Ehrlichiosis, been identified in people. Equine Granulocytic Anaplasmosis, Recent changes in taxonomy can make the nomenclature of the Anaplasmataceae Tick-borne Fever, and their diseases somewhat confusing. At one time, ehrlichiosis was a group of Pasture Fever, diseases caused by organisms that mostly replicated in membrane-bound cytoplasmic Human Monocytic Ehrlichiosis, vacuoles of leukocytes, and belonged to the genus Ehrlichia, tribe Ehrlichieae and Human Granulocytic Anaplasmosis, family Rickettsiaceae. The names of the diseases were often based on the host Human Granulocytic Ehrlichiosis, species, together with type of leukocyte most often infected. -

Pulmonary Hypertension and Exercise Intolerance in Patients with Heart Failure Javed Butler, MD, Don B
View metadata, citation and similar papers at core.ac.uk brought to you by CORE provided by Elsevier - Publisher Connector Journal of the American College of Cardiology Vol. 34, No. 6, 1999 © 1999 by the American College of Cardiology ISSN 0735-1097/99/$20.00 Published by Elsevier Science Inc. PII S0735-1097(99)00408-8 Pulmonary Hypertension and Exercise Intolerance in Patients With Heart Failure Javed Butler, MD, Don B. Chomsky, MD, John R. Wilson, MD, FACC Nashville, Tennessee OBJECTIVES This study was undertaken to investigate the relationship between pulmonary hypertension and exercise performance in patients with heart failure. BACKGROUND The exercise capacity of patients with heart failure is frequently reduced. Pulmonary hypertension may contribute to this exercise intolerance by impairing blood flow through the pulmonary circulation. METHOD Three hundred twenty patients with heart failure underwent upright treadmill exercise testing with hemodynamic monitoring. The incidence of pulmonary hypertension and the relation- ship between pulmonary vascular resistance (PVR) and exercise cardiac output and minute oxygen consumption (VO2) were examined. RESULTS Pulmonary vascular resistance was normal (Ͻ1.5 Wood Units; Group 1) in 28% of the patients, mildly elevated (1.5 to 2.49 Wood Units; Group 2) in 36%, moderately elevated (2.5 to 3.49 Wood Units; Group 3) in 17% and severely elevated (Ͼ3.5 Wood Units; Group 4) in 19%. Increasing PVR was associated with significantly lower peak exercise VO2 (Group 1: 13.9 Ϯ 3.7; 2:13.7 Ϯ 3.4; 3: 11.8 Ϯ 2.4; 4: 11.5 Ϯ 2.6 L/min, p Ͻ 0.01 Groups 3 and 4 vs. -

Review of Systems
code: GF004 REVIEW OF SYSTEMS First Name Middle Name / MI Last Name Check the box if you are currently experiencing any of the following : General Skin Respiratory Arthritis/Rheumatism Abnormal Pigmentation Any Lung Troubles Back Pain (recurrent) Boils Asthma or Wheezing Bone Fracture Brittle Nails Bronchitis Cancer Dry Skin Chronic or Frequent Cough Diabetes Eczema Difficulty Breathing Foot Pain Frequent infections Pleurisy or Pneumonia Gout Hair/Nail changes Spitting up Blood Headaches/Migraines Hives Trouble Breathing Joint Injury Itching URI (Cold) Now Memory Loss Jaundice None Muscle Weakness Psoriasis Numbness/Tingling Rash Obesity Skin Disease Osteoporosis None Rheumatic Fever Weight Gain/Loss None Cardiovascular Gastrointestinal Eyes - Ears - Nose - Throat/Mouth Awakening in the night smothering Abdominal Pain Blurring Chest Pain or Angina Appetite Changes Double Vision Congestive Heart Failure Black Stools Eye Disease or Injury Cyanosis (blue skin) Bleeding with Bowel Movements Eye Pain/Discharge Difficulty walking two blocks Blood in Vomit Glasses Edema/Swelling of Hands, Feet or Ankles Chrohn’s Disease/Colitis Glaucoma Heart Attacks Constipation Itchy Eyes Heart Murmur Cramping or pain in the Abdomen Vision changes Heart Trouble Difficulty Swallowing Ear Disease High Blood Pressure Diverticulosis Ear Infections Irregular Heartbeat Frequent Diarrhea Ears ringing Pain in legs Gallbladder Disease Hearing problems Palpitations Gas/Bloating Impaired Hearing Poor Circulation Heartburn or Indigestion Chronic Sinus Trouble Shortness -

Impact of Atrial Fibrillation on Exercise Capacity And
ORIGINAL RESEARCH Impact of Atrial Fibrillation on Exercise Capacity and Mortality in Heart Failure With Preserved Ejection Fraction: Insights From Cardiopulmonary Stress Testing Mohamed B. Elshazly, MD; Todd Senn, MD; Yuping Wu, PhD; Bruce Lindsay, MD; Walid Saliba, MD; Oussama Wazni, MD; Leslie Cho, MD Background-—Atrial fibrillation (AF) has been objectively associated with exercise intolerance in patients with heart failure with reduced ejection fraction; however, its impact in patients with heart failure with preserved ejection fraction has not been fully scrutinized. Methods and Results-—We identified 1744 patients with heart failure and ejection fraction ≥50% referred for cardiopulmonary stress testing at the Cleveland Clinic (Cleveland, OH), 239 of whom had AF. We used inverse probability of treatment weighting to balance clinical characteristics between patients with and without AF. A weighted linear regression model, adjusted for unbalanced variables (age, sex, diagnosis, hypertension, and b-blocker use), was used to compare metabolic stress parameters and 8-year total mortality (social security index) between both groups. Weighted mean ejection fraction was 58Æ5.9% in the entire population. After adjusting for unbalanced weighted variables, patients with AF versus those without AF had lower mean peak oxygen consumption (18.5Æ6.2 versus 20.3Æ7.1 mL/kg per minute), oxygen pulse (12.4Æ4.3 versus 12.9Æ4.7 mL/beat), and circulatory power (2877Æ1402 versus 3351Æ1788 mm HgÁmL/kg per minute) (P<0.001 for all comparisons) but similar submaximal exercise capacity (oxygen consumption at anaerobic threshold, 12.0Æ5.1 versus 12.4Æ6.0mL/kg per minute; P =0.3). Both groups had similar peak heart rate, whereas mean peak systolic blood pressure was lower in the AF group (150Æ35 versus 160Æ51 mm Hg; P<0.001). -

Review of Systems – Return Visit Have You Had Any Problems Related to the Following Symptoms in the Past Month? Circle Yes Or No
REVIEW OF SYSTEMS – RETURN VISIT HAVE YOU HAD ANY PROBLEMS RELATED TO THE FOLLOWING SYMPTOMS IN THE PAST MONTH? CIRCLE YES OR NO Today’s Date: ______________ Name: _______________________________ Date of Birth: __________________ GENERAL GENITOURINARY Fatigue Y N Blood in Urine Y N Fever / Chills Y N Menstrual Irregularity Y N Night Sweats Y N Painful Menstrual Cycle Y N Weight Gain Y N Vaginal Discharge Y N Weight Loss Y N Vaginal Dryness Y N EYES Vaginal Itching Y N Vision Changes Y N Painful Sex Y N EAR, NOSE, & THROAT SKIN Hearing Loss Y N Hair Loss Y N Runny Nose Y N New Skin Lesions Y N Ringing in Ears Y N Rash Y N Sinus Problem Y N Pigmentation Change Y N Sore Throat Y N NEUROLOGIC BREAST Headache Y N Breast Lump Y N Muscular Weakness Y N Tenderness Y N Tingling or Numbness Y N Nipple Discharge Y N Memory Difficulties Y N CARDIOVASCULAR MUSCULOSKELETAL Chest Pain Y N Back Pain Y N Swelling in Legs Y N Limitation of Motion Y N Palpitations Y N Joint Pain Y N Fainting Y N Muscle Pain Y N Irregular Heart Beat Y N ENDOCRINE RESPIRATORY Cold Intolerance Y N Cough Y N Heat Intolerance Y N Shortness of Breath Y N Excessive Thirst Y N Post Nasal Drip Y N Excessive Amount of Urine Y N Wheezing Y N PSYCHOLOGY GASTROINTESTINAL Difficulty Sleeping Y N Abdominal Pain Y N Depression Y N Constipation Y N Anxiety Y N Diarrhea Y N Suicidal Thoughts Y N Hemorrhoids Y N HEMATOLOGIC / LYMPHATIC Nausea Y N Easy Bruising Y N Vomiting Y N Easy Bleeding Y N GENITOURINARY Swollen Lymph Glands Y N Burning with Urination Y N ALLERGY / IMMUNOLOGY Urinary -

How to Recognize a Suspected Cardiac Defect in the Neonate
Neonatal Nursing Education Brief: How to Recognize a Suspected Cardiac Defect in the Neonate https://www.seattlechildrens.org/healthcare- professionals/education/continuing-medical-nursing-education/neonatal- nursing-education-briefs/ Cardiac defects are commonly seen and are the leading cause of death in the neonate. Prompt suspicion and recognition of congenital heart defects can improve outcomes. An ECHO is not needed to make a diagnosis. Cardiac defects, congenital heart defects, NICU, cardiac assessment How to Recognize a Suspected Cardiac Defect in the Neonate Purpose and Goal: CNEP # 2092 • Understand the signs of congenital heart defects in the neonate. • Learn to recognize and detect heart defects in the neonate. None of the planners, faculty or content specialists has any conflict of interest or will be presenting any off-label product use. This presentation has no commercial support or sponsorship, nor is it co-sponsored. Requirements for successful completion: • Successfully complete the post-test • Complete the evaluation form Date • December 2018 – December 2020 Learning Objectives • Describe the risk factors for congenital heart defects. • Describe the clinical features of suspected heart defects. • Identify 2 approaches for recognizing congenital heart defects. Introduction • Congenital heart defects may be seen at birth • They are the most common congenital defect • They are the leading cause of neonatal death • Many neonates present with symptoms at birth • Some may present after discharge • Early recognition of CHD -

Cutaneous Manifestations of Abdominal Arteriovenous Fistulas
Cutaneous Manifestations of Abdominal Arteriovenous Fistulas Jessica Scruggs, MD; Daniel D. Bennett, MD Abdominal arteriovenous (A-V) fistulas may be edema.1-3 We report a case of abdominal aortocaval spontaneous or secondary to trauma. The clini- fistula presenting with lower extremity edema, ery- cal manifestations of abdominal A-V fistulas are thema, and cyanosis that had been previously diag- variable, but cutaneous findings are common and nosed as venous stasis dermatitis. may be suggestive of the diagnosis. Cutaneous physical examination findings consistent with Case Report abdominal A-V fistula include lower extremity A 51-year-old woman presented to the emergency edema with cyanosis, pulsatile varicose veins, department with worsening lower extremity swelling, and scrotal edema. redness, and pain. Her medical history included a We present a patient admitted to the hospital diagnosis of congestive heart failure, chronic obstruc- with lower extremity swelling, discoloration, and tive pulmonary disease, hepatitis C virus, tobacco pain, as well as renal insufficiency. During a prior abuse, and polysubstance dependence. Swelling, red- hospitalization she was diagnosed with venous ness, and pain of her legs developed several years stasis dermatitis; however, CUTISher physical examina- prior, and during a prior hospitalization she had been tion findings were not consistent with that diagno- diagnosed with chronic venous stasis dermatitis as sis. Imaging studies identified and characterized well as neurodermatitis. an abdominal aortocaval fistula. We propose that On admission, the patient had cool lower extremi- dermatologists add abdominal A-V fistula to the ties associated with discoloration and many crusted differential diagnosis of patients presenting with ulcerations. Aside from obesity, her abdominal exam- lower extremity edema with cyanosis, and we ination was unremarkable and no bruits were noted. -

Statewide Heart Failure Service, Heart Failure Daily Diary
Available online at www.sciencedirect.com Journal of Science and Medicine in Sport 13 (2010) 288–294 Position statement Exercise & Sports Science Australia Position Statement on exercise training and chronic heart failure Steve E. Selig a,b,∗, Itamar Levinger a,b, Andrew D. Williams c, Neil Smart d, David J. Holland e, Andrew Maiorana f,g, Daniel J. Green h,i, David L. Hare b,j a Institute for Sport, Exercise and Active Living, School of Sport and Exercise Science, Victoria University, Melbourne, Australia b Department of Cardiology, Austin Health, Melbourne, Australia c School of Human Life Sciences, University of Tasmania, Tasmania, Australia d Faculty of Health Science and Medicine, Bond University, QLD, Australia e School of Medicine, University of Queensland, Brisbane, Australia f Cardiac Transplant Unit, Royal Perth Hospital, Australia g School of Physiotherapy, Curtin University of Technology, Australia h School of Sport Science, Exercise and Health, University of Western Australia, Australia i Research Institute for Sport and Exercise Sciences, Liverpool John Moores University, United Kingdom j School of Medicine, University of Melbourne, Australia Received 18 September 2009; received in revised form 18 January 2010; accepted 19 January 2010 Abstract Chronic heart failure (CHF) is a complex syndrome characterised by progressive decline in left ventricular function, low exercise tolerance and raised mortality and morbidity. Regular exercise participation has been shown to be a safe and effective treatment modality in the majority of CHF patients, partially reversing some of the maladaptations evident in myocardial and skeletal muscle function, and resulting in improvements in physical fitness and quality of life, and perhaps reduced mortality. -
Documenting History at a Glance
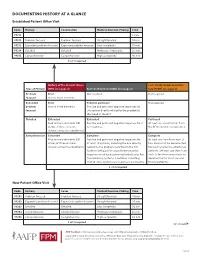
DOCUMENTING HISTORY AT A GLANCE Established Patient Office Visit Code History Examination Medical Decision-Making Time 99211 — — — 5 min. 99212 Problem focused Problem focused Straightforward 10 min. 99213 Expanded problem focused Expanded problem focused Low complexity 15 min. 99214 Detailed Detailed Moderate complexity 25 min. 99215 Comprehensive Comprehensive High complexity 40 min. 2 of 3 required History of the Present Illness Past, Family and/or Social His- Type of History (HPI) (see page 2) Review of Systems (ROS) (see page 2) tory (PFSH) (see page 2) Problem Brief Not required Not required focused One to three elements Expanded Brief Problem pertinent Not required problem One to three elements Positive and pertinent negative responses for focused the system directly related to the problem(s) identified in the HPI. Detailed Extended Extended Pertinent Four or more elements (OR Positive and pertinent negative responses for 2 At least one specific item from status of three or more to 9 systems. the PFSH must be documented. chronic or inactive conditions) Comprehensive Extended Complete Complete Four or more elements (OR Positive and pertinent negative responses for At least one item from each of status of three or more at least 10 systems, including the one directly two areas must be documented chronic or inactive conditions) related to the problem identified in the HPI. for most services to established Systems with positive or pertinent negative patients. (At least one item from responses must be documented individually. For each of the three areas must be the remaining systems, a notation indicating documented for most services that all other systems are negative is permissible.