Crr 412/2002
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

May CARG 2020.Pdf
ISSUE 30 – MAY 2020 ISSUE 30 – MAY ISSUE 29 – FEBRUARY 2020 Promoting positive mental health in teenagers and those who support them through the provision of mental health education, resilience strategies and early intervention What we offer Calm Harm is an Clear Fear is an app to Head Ed is a library stem4 offers mental stem4’s website is app to help young help children & young of mental health health conferences a comprehensive people manage the people manage the educational videos for students, parents, and clinically urge to self-harm symptoms of anxiety for use in schools education & health informed resource professionals www.stem4.org.uk Registered Charity No 1144506 Any individuals depicted in our images are models and used solely for illustrative purposes. We all know of young people, whether employees, family or friends, who are struggling in some way with mental health issues; at ARL, we are so very pleased to support the vital work of stem4: early intervention really can make a difference to young lives. Please help in any way that you can. ADVISER RANKINGS – CORPORATE ADVISERS RANKINGS GUIDE MAY 2020 | Q2 | ISSUE 30 All rights reserved. No part of this publication may be reproduced or transmitted The Corporate Advisers Rankings Guide is available to UK subscribers at £180 per in any form or by any means (including photocopying or recording) without the annum for four updated editions, including postage and packaging. A PDF version written permission of the copyright holder except in accordance with the provision is also available at £360 + VAT. of copyright Designs and Patents Act 1988 or under the terms of a licence issued by the Copyright Licensing Agency, Barnard’s Inn, 86 Fetter Lane, London, EC4A To appear in the Rankings Guide or for subscription details, please contact us 1EN. -

City-REDI Policy Briefing Series
City-REDI Policy Briefing Series March Image Image 2018 Part B Carillion’s Collapse: Consequences Dr Amir Qamar & Professor Simon Collinson Carillion, the second-largest construction firm in the UK, were proud of their commitment to support regional growth and small-scale suppliers. As part of this commitment they directed 60% of project expenditure to local economies. Following the collapse of the firm, this positive multiplier effect became a significant, negative multiplier effect, particularly damaging to small-scale suppliers in the construction industry. The aim of this policy brief is to examine the consequences of Carillion’s demise, many of which are only now surfacing. One of the fundamental lessons that we can learn from Carillion’s collapse is about these ‘contagion’ effects. As we saw in the 2008 financial crisis, the businesses that underpin the economic health of the country are connected and strongly co-dependent. When a large flagship firm falls it brings down others. This does not mean we need more state intervention. But it does mean we need more intelligent state intervention. One of the fundamental lessons that the Government can learn from the Carillion episode is that it has a significant responsibility as a key customer, using public sector funds for public sector projects, to monitor the health of firms and assess the risks prior to issuing PPI and other contracts. 1 Introduction The collapse of Carillion, the second-largest construction firm in the UK, has had a significant, negative knock-on effect, particularly on small-scale suppliers in the industry. In total, Carillion was comprised of 326 subsidiaries, of which 199 were in the UK. -
![J Jarvis & Sons Ltd V Blue Circle Dartford Estates Ltd [2007]](https://docslib.b-cdn.net/cover/2296/j-jarvis-sons-ltd-v-blue-circle-dartford-estates-ltd-2007-322296.webp)
J Jarvis & Sons Ltd V Blue Circle Dartford Estates Ltd [2007]
J Jarvis & Sons Ltd v Blue Circle Dartford Estates Ltd [2007] APP.L.R. 05/14 JUDGMENT : MR JUSTICE JACKSON: TCC. 14th May 2007 1. This judgment is in seven parts, namely, Part 1 "Introduction"; Part 2 "The Facts"; Part 3 "The Present Proceedings"; Part 4 "The Law"; Part 5 "The Application for an Injunction"; Part 6 "Jarvis's Challenges to the Interim Award"; and Part 7 "Conclusion". Part 1: Introduction 2. This is an action brought by a main contractor in order to prevent the continuance of an arbitration. The contractor seeks to achieve that result either by means of an injunction or, alternatively, by challenging an Interim Award of the Arbitrator. This litigation has been infused with some urgency because it was launched just fifteen days before the date fixed for the start of arbitration hearing. 3. J Jarvis & Sons Limited is claimant in these proceedings and defendant in the arbitration. Prior to 18th February 1997, the name of this company was J Jarvis & Sons plc. I shall refer to the company as "Jarvis". Jarvis is the subsidiary company of Jarvis plc. Blue Circle Dartford Estates Limited is defendant in these proceedings and claimant in the arbitration. I shall refer to this party as "Blue Circle". Blue Circle is a subsidiary company of Blue Circle Industries plc. The solicitors for the parties will feature occasionally in the narrative. Squire & Co are solicitors for Jarvis. Howrey LLP are solicitors for Blue Circle. 4. I turn now to other companies which will feature in the narrative of events. GEFCO (UK) Limited are forwarding agents. -

Monitoring the London Plan Energy Policies Phase 3
Monitoring the London Plan Energy Policies Phase 3 Part 1 report FINAL December 2009 Prepared for: By: Greater London Authority Prof Tony Day, Princess Ogumka & City Hall Phil Jones The Queen’s Walk London South Bank University London SE1 2AA 103 Borough Road Tel 020 7983 4592 London SE1 0AA Tel: 020 7815 7656 E-mail: [email protected] Part 1 report FINAL Contents CONTENTS.................................................................................................................................2 EXECUTIVE SUMMARY.......................................................................................................3 1. INTRODUCTION .............................................................................................................8 2. RESULTS ......................................................................................................................... 10 2.1. Emissions.................................................................................................................................. 11 2.2. Savings..................................................................................................................................... 12 2.3. Analysis of Energy Efficiency contributions............................................................................... 17 2.4. Analysis of contributions from CHP with communal heating .................................................... 19 2.4.1. Contribution by CHP type........................................................................................................ -

Housing Audit: Assessing the Design Quality of New Homes
1 SENSE OF PLACE SENSE OF PLACE 2 APPROPRIATE ENCLOSURE ■ Main Street ■ Secondary Street ■ Tertiary Street / Lane / Courtyard 3 SAFETY ■ Is there active frontage on public spaces? ■ Is there overlooking frontage on public spaces? ■ Are the public spaces well lit? ■ Is there fenestration on two elevations at corners? 4 LEGIBILITY ■ Are there orientation markers? ■ Is there a series of events/spaces? 5 EXPLOITATION OF SITE’S ASSETS ■ Are existing buildings retained? ■ Is mature planting retained? ■ Does the layout respond to topography? 6 AVOIDANCE OF HIGHWAY DOMINANCE AND PEDESTRIAN REALM ROADS, PARKING ■ Do footpaths relate to building line? ■ Does the carriageway width vary? 7 PROMOTION OF NON-CAR TRAVEL ■ Is there a permeable network of routes? ■ Are the streets designed to calm traffic? ■ Are there dedicated bus/cycle lanes? ■ Is there safe cycle storage, close to homes? 8 CAR PARKING BUILDING FOR LIFE ■ Parking Type ■ Is it well integrated with public space? ■ Is parking visually unobtrusive? ■ Is it well integrated with planting? 9 SERVICING ■ Is the waste storage unobtrusive? ■ Are servicing arrangements well integrated? 10 MOVEMENT INTEGRATION ■ Are there connections to existing footpaths? ■ Are there multiple connections to the surrounding road network? ■ Is there easy access to main routes? ■ Does the development integrate with existing built development? 11 BESPOKE DESIGN DESIGN & CONSTRUCTION ■ Is bespoke design evident? ■ Is the local vernacular employed? 12 ARCHITECTURAL QUALITY ■ Are good quality materials used? ■ Is attention -
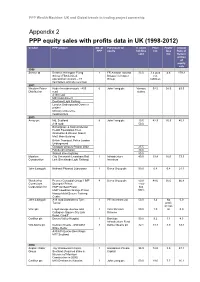
Appendix 2 PPP Equity Sales with Profits Data in UK (1998-2012)
PPP Wealth Machine: UK and Global trends in trading project ownership Appendix 2 PPP equity sales with profits data in UK (1998-2012) Vendor PPP project No. of Purchaser of % share Price Profit/ Annual PPP equity holding £m loss Rate of sold £m Return at time of equity sale 1998 Serco Ltd Defence Helicopter Flying 1 FR Aviation Ltd and 33.0 3.4 plus 4.6 179.3 School (FBS Limited, Bristow Helicopter net operational contract – 47 Group liabilities helicopters and site services) 2001 Western Power Hyder Investments plc - A55 6 John Laing plc Various 92.5 58.5 63.3 Distribution road stakes A130 road M40 road project Dockland Light Railway London Underground Connect project Ministry of Defence headquarters 2003 Amey plc M6, Scotland 8 John Laing plc 19.5 42.9 25.9 45.2 A19 road 50.0 Birmingham & Solihull Mental Health Foundation Trust (Erdington & Winson Green) MoD Main Building British Transport Police London Underground Glasgow schools-Project 2002 25.5 Edinburgh schools 30.0 Walsall street lighting 50.0 Mowlem City Greenwich Lewisham Rail 1 Infrastructure 40.0 19.4 16.0 73.3 Construction Link (Docklands Light Railway) Investors John Laing plc National Physical Laboratory 1 Serco Group plc 50.0 0.8 0.4 21.1 Wackenhut Premier Custodial Group: HMP 4 Serco Group plc 50.0 48.6 35.0 66.8 Corrections Dovegate Prison - now Corporation Inc HMP Ashfield Prison has HMP Lowdham Grange Prison 100% Hassockfield Secure Training Centre John Laing plc A19 road Dishforth to Tyne 1 PFI Investors Ltd 50.0 3.4 No 0.0 Tunnel profit or loss Vinci plc Lloyd George -

Safestyle UK Plc Annual Report & Accounts 2019 Safestyle UK Plc
safestyleukplc.co.uk Safestyle UK plc Annual Report & Accounts 2019 Safestyle UK plc Financial Overview Contents Revenue (£m) 2017 158.6 Safestyle UK plc 2018 116.4 -27% Annual Report 2019 2019 126.2 8% The UK’s No.1 for replacement Underlying profit / (loss) before taxation¹ (£m) 2017 15.1 windows and doors³ 2018 (8.7) -158% 01 Welcome page and Financial Overview 2019 (1.5) 83% Strategic Report Reported profit / (loss) before taxation (£m) 06 What we do 2017 13.8 20 Chairman’s Statement 22 CEO’s Statement 2018 (16.3) -218% 24 Financial Review 2019 (3.8) 76% 30 Risk Management 36 Corporate Social Responsibility 38 Our People Net cash² (£m) Governance 2017 11.0 2018 0.3 -98% 46 Board of Directors 48 Audit Committee Report 2019 0.4 71% 50 Directors’ Remuneration Report 58 Directors’ Report Average installed order value (£) 61 Independent Auditor’s Report 2017 3,232 Financials 2018 3,319 3% 68 Consolidated Income Statement 2019 3,337 1% 69 Consolidated Statement of Financial Position 70 Consolidated Statement of Changes in Equity 71 Consolidated Statement of Cash Flows Average frame price (£) 72 Notes to the Consolidated Financial Statements 2017 608 2018 646 6% 2019 678 5% Frames installed 2017 265,716 2018 184,184 -31% 2019 190,252 3% ¹ See the Financial Review for definition of underlying profit / (loss) before taxation ² See the Financial Review for definition of net cash Annual Report & Accounts 2019 01 ³ Based on Fensa data Safestyle UK plc Highly Recommended All figures from February 2020 Safestyle UK leading the way in customer reviews -
VPS SPD Consultation Statement
Parking Standards Design and Good Practice Supplementary Planning Document Consultation Statement (Regulation 17 Statement) In the preparation of draft Supplementary Planning Guidance the Department for Communities and Local Government advises authorities to informally involve local communities and other stakeholders in the development of policies. Work on the Parking Standards Design and Good Practice document commenced in May 2007 by the forming of a Parking Standards Review Group. This group was led by officers of the Essex County Council Strategic Development section working with colleagues from both within Essex County Council and Essex local authorities. A list of those involved is included on page iii of the document. The development of the draft Parking Standards Design and Good Practice document has taken place over a 24-month period and comprised the following main activities: Residents Survey May- September 2007 (to complement a related existing survey undertaken in 2006) Group Site visits June – July 2007 Individual site visits, evening and weekends June – July 2007 Education meeting August 2007 Regular Review Group meetings May – April 2008 Review of other authority Parking Standards May – April 2008 SEA September 2008 – March 2009 Public Consultation March – April 2009 The scope and outcome of these activities are summarised below: 1. Residents Survey A survey was undertaken by Essex County Council term consultant’s Mouchel, to ascertain the opinions of local residents from housing developments that had recently been constructed -
Annual Report and Accounts 2006
ANNUAL REPORT AND ACCOUNTS 2006 MAKING TOMORROW A BETTER PLACE Report Section 01 Our Mission, Vision, Values and Strategy Section 02 A Year of Good Progress 02 Financial Highlights 03 Chairman’s Statement Section 03 What We Do 04 At a glance Section 04 Operating and Financial Review 06 Chief Executive’s Review 10 Markets and Outlook Defence/Education/Health Facilities Management and Services/Building Roads and Civil Engineering/Rail Middle East/Canada and the Caribbean 18 Financial Review 22 Corporate Social Responsibility Section 05 A Strong Team 24 Board of Directors Section 06 Accountability 26 Corporate Governance Report 31 Remuneration Report 39 Report of the Directors 42 Statement of Directors’ Responsibilities in Respect of the Annual Report and Financial Statements 43 Independent Auditors’ Report to the Members of Carillion plc Section 07 Financial Statements 44 Consolidated Income Statement 45 Consolidated Statement of Recognised Income and Expense 46 Consolidated Balance Sheet 47 Consolidated Statement of Cash Flows 48 Notes to the Consolidated Financial Statements 82 Company Balance Sheet 83 Notes to the Company Our mission Financial Statements Making tomorrow a better place. Section 08 Further Information Our vision 89 Five Year Review To be the leader in delivering integrated 91 Principal Subsidiary Undertakings, Jointly Controlled Entities and solutions for infrastructure, buildings Jointly Controlled Operations and services. 92 Shareholder Information IBC Advisers For the latest information, including Investor Relations and Sustainability, visit our website any time. www.carillionplc.com Cover – Restoration art The Ikon Gallery, Birmingham is now housed in a former neo-gothic school restored by Carillion to its former architec- tural glory. -

Here Possible
THIS DOCUMENT IS IMPORTANT AND REQUIRES YOUR IMMEDIATE ATTENTION If you are in any doubt as to the action you should take you should immediately seek advice from your stockbroker, bank manager, solicitor, accountant or other independent professional advisor duly authorised under the Financial Services and Markets Act 2000. If you have sold or otherwise transferred all of your shares in SIG plc, please forward this document and the Form of Proxy as soon as possible to the purchaser or transferee or to the stockbroker, bank or other agent through whom the sale or transfer was effected, for transmission to the purchaser or transferee. SIG plc (Registered in England No. 998314) Chairman’s Letter to Shareholders and Notice of Annual General Meeting The Annual General Meeting is to be held at the offices of SIG Plc, 10 Eastbourne Terrace, London, W2 6LG on Tuesday 30 June 2020 at 11am The Notice of Annual General Meeting is set out on pages 7 to 9 of this Document. A Form of Proxy for use at the Annual General Meeting is enclosed. SIG plc Notice of Annual General Meeting 2020 01 SIG Notice of Meeting-2020.indd 1 29/05/2020 16:37:24 26982 29 May 2020 4:37 pm Proof 10 SIG plc (Registered in England No. 998314) DIRECTORS: REGISTERED OFFICE A.J. Allner 10 Eastbourne Terrace S.R Francis London K.H.M Kearney-Croft W2 6LG H.C Allum I.B. Duncan G.D.C Kent A.C. Lovell 5 June 2020 Dear Shareholder, ANNUAL GENERAL MEETING 2020 NOTICE OF MEETING I am writing to explain in detail the items of business contained in the Notice of Annual General Meeting (the “AGM”) of SIG plc (the “Company”), to be held at 11am on Tuesday 30 June 2020 at the offices of SIG Plc, 10 Eastbourne Terrace, London, W2 6LG. -

SC03-1610 RAYMOND JAMES FINANCIAL : SERVICES, INC., a Florida Corporation
SUPREME COURT OF FLORIDA TALLAHASSEE, FLORIDA CASE NO: SC03-1610 RAYMOND JAMES FINANCIAL : SERVICES, INC., a Florida corporation : and RICHARD VANDENBERG, : : Petitioners, : : v. : : STEVEN W. SALDUKAS and : STESAL INVESTMENTS, LLC., : : Respondents. : ___________________________________ : ON APPEAL FROM THE SECOND DISTRICT COURT OF APPEALS LAKELAND, FLORIDA RESPONDENTS’ BRIEF ON THE MERITS Christopher T. Vernon Attorneys for Respondent Florida Bar No. 0748110 Benjamin C. Iseman Florida Bar No. 0194506 Treiser, Collins & Vernon 3080 Tamiami Trail East Naples, Florida 34112 Telephone (239) 649-4900 Facsimile (239) 649-0823 F. Paul Bland, Jr. (Petition for pro hac vice admission pending) Trial Lawyers for Public Justice 1717 Massachusetts Avenue, NW Suite 800 Washington, D.C. 20036 Telephone (202) 797-8600 Facsimile (202) 232-7203 Attorneys for Respondents TABLE OF CONTENTS Page(s) STATEMENT OF THE CASE AND OF THE FACTS .................... 3 SUMMARY OF ARGUMENT .................................... 10 I. STANDARD OF REVIEW .................................. 13 II. A SHOWING OF PREJUDICE IS NOT REQUIRED TO ESTABLISH A WAIVER OF THE RIGHT TO ARBITRATE. .................. 15 A. UNDER THE FEDERAL ARBITRATION ACT, THIS COURT SHOULD ANALYZE THIS ISSUE UNDER GENERALLY APPLICABLE PRINCIPLES OF FLORIDA CONTRACT LAW. ............................................. 15 B. GENERALLY APPLICABLE PRINCIPLES OF FLORIDA CONTRACT LAW DO NOT REQUIRE A SHOWING OF PREJUDICE TO ESTABLISH THE WAIVER OF CONTRACTUAL RIGHT. ............................. 21 C. THE MORE PERSUASIVE FEDERAL AND STATE AUTHORITIES AGREE THAT A SHOWING OF PREJUDICE i IS NOT REQUIRED TO DEMONSTRATE THAT A PARTY HAS WAIVED ITS RIGHT TO ARBITRATE. ............... 26 1. Persuasive Federal Authorities Support the Plaintiffs Here ............................. 26 2. The Federal Cases Relied Upon by Defendants Are Not Persuasive .......................... 29 3. The Florida Cases Relied Upon By Defendants Are Not Persuasive ......................... -
Building Towards Sustainability
Building Towards Sustainability Performance and Progress Among the UK’s Leading Housebuilders Part of WWF’s One Million Sustainable Homes Campaign For further information go to: www.wwf.org.uk/sustainablehomes Introducing Insight Investment Upstream is a strategic sustainability consultancy specialising in the built environment sector. Upstream Insight Investment is the asset manager of UK assists its clients to develop strategies for economic, financial services company HBOS. It currently environmental and social responsibility, and to manages £67.8 billion. These funds represent the integrate and align them with their business goals. assets of millions of people in the form of their Upstream pensions, life insurance and other stock market- 70 Cowcross Street based investments. Insight has an explicit London EC1M 6EJ commitment to act as a responsible investor on behalf of its clients. For further information see Telephone: 020 7250 3900 Insight’s Investor Responsibility Policy, available online Fax: 020 7250 3580 at www.insightinvestment.com/corporate/responsibility www.upstreamstrategies.co.uk There are two principal reasons why Insight pursues a policy of engaging with companies in which it invests. First, Insight believes it is in its clients’ long-term financial interests that the companies in which it invests behave responsibly. Failure to do so typically provokes government and societal sanctions such as fines, litigation, new regulation and taxes, consumer boycotts and damage to reputation, all of which create material risks to long-term shareholder value. Insight therefore analyses and engages with companies to assess and to encourage them to operate according to best practice standards on a range of environmental, ethical and social issues.