18. Molepolole
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

The Parliamentary Constituency Offices
REPUBLIC OF BOTSWANA THE PARLIAMENTARY CONSTITUENCY OFFICES Parliament of Botswana P O Box 240 Gaborone Tel: 3616800 Fax: 3913103 Toll Free; 0800 600 927 e - mail: [email protected] www.parliament.gov.bw Introduction Mmathethe-Molapowabojang Mochudi East Mochudi West P O Box 101 Mmathethe P O Box 2397 Mochudi P O Box 201951 Ntshinoge Representative democracy can only function effectively if the Members of Tel: 5400251 Fax: 5400080 Tel: 5749411 Fax: 5749989 Tel: 5777084 Fax: 57777943 Parliament are accessible, responsive and accountable to their constituents. Mogoditshane Molepolole North Molepolole South The mandate of a Constituency Office is to act as an extension of Parliament P/Bag 008 Mogoditshane P O Box 449 Molepolole P O Box 3573 Molepolole at constituency level. They exist to play this very important role of bringing Tel: 3915826 Fax: 3165803 Tel: 5921099 Fax: 5920074 Tel: 3931785 Fax: 3931785 Parliament and Members of Parliament close to the communities they serve. Moshupa-Manyana Nata-Gweta Ngami A constituency office is a Parliamentary office located at the headquarters of P O Box 1105 Moshupa P/Bag 27 Sowa Town P/Bag 2 Sehithwa Tel: 5448140 Fax: 5448139 Tel: 6213756 Fax: 6213240 Tel: 6872105/123 each constituency for use by a Member of Parliament (MP) to carry out his or Fax: 6872106 her Parliamentary work in the constituency. It is a formal and politically neutral Nkange Okavango Palapye place where a Member of Parliament and constituents can meet and discuss P/Bag 3 Tutume P O Box 69 Shakawe P O Box 10582 Palapye developmental issues. Tel: 2987717 Fax: 2987293 Tel: 6875257/230 Tel: 4923475 Fax: 4924231 Fax: 6875258 The offices must be treated strictly as Parliamentary offices and must therefore Ramotswa Sefhare-Ramokgonami Selibe Phikwe East be used for Parliamentary business and not political party business. -

Bank of Botswana
PAPER 4 BANK OF BOTSWANA DIRECTORY OF FINANCIAL INSTITUTIONS OPERATING IN BOTSWANA AS AT DECEMBER 31, 2009 PREPARED AND DISTRIBUTED BY THE BANKING SUPERVISION DEPARTMENT BANK OF BOTSWANA Foreword This directory is compiled and distributed by the Banking Supervision Department of the Bank of Botswana. While every effort has been made to ensure the accuracy of the information contained in this directory, such information is subject to frequent revision, and thus the Bank accepts no responsibility for the continuing accuracy of the information. Interested parties are advised to contact the respective financial institutions directly for any information they require. This directory excludes Collective Investment Undertakings and International Financial Services Centre non-bank entities, whose regulation and supervision have been transferred to the Non-Bank Financial Institutions Regulatory Authority. Oabile Mabusa DIRECTOR BANKING SUPERVISION DEPARTMENT 1 DIRECTORY OF FINANCIAL INSTITUTIONS OPERATING IN BOTSWANA TABLE OF CONTENTS 1. CENTRAL BANK ............................................................................................................................................. 4 2. COMMERCIAL BANKS ................................................................................................................................... 6 2.1 ABN AMRO BANK (B OTSWANA ) LIMITED ..................................................................................................... 6 2.2 ABN AMRO BANK (B OTSWANA ) OBU LIMITED ........................................................................................... -

Land Tenure Reforms and Social Transformation in Botswana: Implications for Urbanization
Land Tenure Reforms and Social Transformation in Botswana: Implications for Urbanization. Item Type text; Electronic Dissertation Authors Ijagbemi, Bayo, 1963- Publisher The University of Arizona. Rights Copyright © is held by the author. Digital access to this material is made possible by the University Libraries, University of Arizona. Further transmission, reproduction or presentation (such as public display or performance) of protected items is prohibited except with permission of the author. Download date 06/10/2021 17:13:55 Link to Item http://hdl.handle.net/10150/196133 LAND TENURE REFORMS AND SOCIAL TRANSFORMATION IN BOTSWANA: IMPLICATIONS FOR URBANIZATION by Bayo Ijagbemi ____________________ Copyright © Bayo Ijagbemi 2006 A Dissertation Submitted to the Faculty of the DEPARTMENT OF ANTHROPOLOGY In Partial Fulfillment of the Requirements For the Degree of DOCTOR OF PHILOSOPHY In the Graduate College THE UNIVERSITY OF ARIZONA 2006 2 THE UNIVERSITY OF ARIZONA GRADUATE COLLEGE As members of the Dissertation Committee, we certify that we have read the dissertation prepared by Bayo Ijagbemi entitled “Land Reforms and Social Transformation in Botswana: Implications for Urbanization” and recommend that it be accepted as fulfilling the dissertation requirement for the Degree of Doctor of Philosophy _______________________________________________________________________ Date: 10 November 2006 Dr Thomas Park _______________________________________________________________________ Date: 10 November 2006 Dr Stephen Lansing _______________________________________________________________________ Date: 10 November 2006 Dr David Killick _______________________________________________________________________ Date: 10 November 2006 Dr Mamadou Baro Final approval and acceptance of this dissertation is contingent upon the candidate’s submission of the final copies of the dissertation to the Graduate College. I hereby certify that I have read this dissertation prepared under my direction and recommend that it be accepted as fulfilling the dissertation requirement. -

Department of Road Transport and Safety Offices
DEPARTMENT OF ROAD TRANSPORT AND SAFETY OFFICES AND SERVICES MOLEPOLOLE • Registration & Licensing of vehicles and drivers • Driver Examination (Theory & Practical Tests) • Transport Inspectorate Tel: 5920148 Fax: 5910620 P/Bag 52 Molepolole Next to Molepolole Police MOCHUDI • Registration & Licensing of vehicles and drivers • Driver Examination (Theory & Practical Tests) • Transport Inspectorate P/Bag 36 Mochudi Tel : 5777127 Fax : 5748542 White House GABORONE Headquarters BBS Mall Plot no 53796 Tshomarelo House (Botswana Savings Bank) 1st, 2nd &3rd Floor Corner Lekgarapa/Letswai Road •Registration & Licensing of vehicles and drivers •Road safety (Public Education) Tel: 3688600/62 Fax : Fax: 3904067 P/Bag 0054 Gaborone GABORONE VTS – MARUAPULA • Registration & Licensing of vehicles and drivers • Driver Examination (Theory & Practical Tests) • Vehicle Examination Tel: 3912674/2259 P/Bag BR 318 B/Hurst Near Roads Training & Roads Maintenance behind Maruapula Flats GABORONE II – FAIRGROUNDS • Registration & Licensing of vehicles and drivers • Driver Examination : Theory Tel: 3190214/3911540/3911994 Fax : P/Bag 0054 Gaborone GABORONE - OLD SUPPLIES • Registration & Licensing of vehicles and drivers • Transport Permits • Transport Inspectorate Tel: 3905050 Fax :3932671 P/Bag 0054 Gaborone Plot 1221, Along Nkrumah Road, Near Botswana Power Corporation CHILDREN TRAFFIC SCHOOL •Road Safety Promotion for children only Tel: 3161851 P/Bag BR 318 B/Hurst RAMOTSWA •Registration & Licensing of vehicles and drivers •Driver Examination (Theory & Practical -

Inside Gabane Murder
THE MIDWEEK SUN www.themidweeksun.co.bw • WEDNESDAY APRIL 29 2020 1 11 WEDNESDAYWEDNESDAY APRILAPRIL 2929 20202020 •• www.themidweeksun.co.bwwww.themidweeksun.co.bw THETHE MIDWEEKMIDWEEK SUNSUN CURRENT SITUATION IN NUMBERS TESTS & RESULTS 6548 NEGATIVE 6525 POSETIVE CASES 23 TOTAL DEATHS 1 RECOVERIES 5 WEDNESDAY 29 APRIL, 2020 P8.00 NEW COMFIRMED CASES 1 WEDNESDAY 22 APRIL 2020 themidweeksun.co.bw P8.00 Poor local musicians resort to manhandling COSBOTS HUNGRY, BEGGARLY AND ANGRY P22 million in COSBOTS coffers – claim I only received P300 – Rapper Scar cries I am broke, I have nothing to eat – Jazz star, Thabang Lezibo calls for reforms at COSBOTS 10 INSIDE GABANE MURDER Why this boy may have killed his father 12 PAGE 8 2 22 WEDNESDAYWEDNESDAY APRIL APRIL 29 2020 29 2020• www.themidweeksun.co.bw • www.themidweeksun.co.bw NEWS THETHE MIDWEEK MIDWEEK SUN SUN NEWS 2 WEDNESDAY APRIL 29 2020 • www.themidweeksun.co.bw NEWS THE MIDWEEK SUN NEWS COVID-19 THE COVID DONATIONS DeBeers AFTERMATH Group’s P1.7m testing Workers may not cope after Covid-19 machine Employers urged to offer BY DIKARABO RAMADUBU psychosocial support DeBeers Group this week donated a COVID-19 testing Some companies will lay machine to government worth off their workers P1.7 million in line with what the company calls their “in- kind support for Government’s BY TLOTLO MBAZO response to the COVID-19 In addition, a review of 24 studies pandemic.” that looked at the psychological The highly sought-after state- eightened stress level is impact of quarantining people, of-the-art testing machine, one of the biggest impacts has shown that people who which was presented to the of the Covid-19 pandemic are quarantined are likely to Minister of Health and Wellness onH employees, according to newly experience low mood, insomnia, Dr Lemogang Kwape, is to be released Covid-19 Work Impact stress, anxiety, anger, irritability, installed at the National Health Assessment report. -
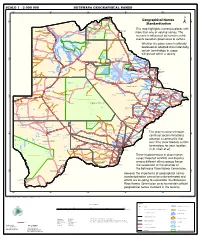
Geographical Names Standardization BOTSWANA GEOGRAPHICAL
SCALE 1 : 2 000 000 BOTSWANA GEOGRAPHICAL NAMES 20°0'0"E 22°0'0"E 24°0'0"E 26°0'0"E 28°0'0"E Kasane e ! ob Ch S Ngoma Bridge S " ! " 0 0 ' ' 0 0 ° Geographical Names ° ! 8 !( 8 1 ! 1 Parakarungu/ Kavimba ti Mbalakalungu ! ± n !( a Kakulwane Pan y K n Ga-Sekao/Kachikaubwe/Kachikabwe Standardization w e a L i/ n d d n o a y ba ! in m Shakawe Ngarange L ! zu ! !(Ghoha/Gcoha Gate we !(! Ng Samochema/Samochima Mpandamatenga/ This map highlights numerous places with Savute/Savuti Chobe National Park !(! Pandamatenga O Gudigwa te ! ! k Savu !( !( a ! v Nxamasere/Ncamasere a n a CHOBE DISTRICT more than one or varying names. The g Zweizwe Pan o an uiq !(! ag ! Sepupa/Sepopa Seronga M ! Savute Marsh Tsodilo !(! Gonutsuga/Gonitsuga scenario is influenced by human-centric Xau dum Nxauxau/Nxaunxau !(! ! Etsha 13 Jao! events based on governance or culture. achira Moan i e a h hw a k K g o n B Cakanaca/Xakanaka Mababe Ta ! u o N r o Moremi Wildlife Reserve Whether the place name is officially X a u ! G Gumare o d o l u OKAVANGO DELTA m m o e ! ti g Sankuyo o bestowed or adopted circumstantially, Qangwa g ! o !(! M Xaxaba/Cacaba B certain terminology in usage Nokaneng ! o r o Nxai National ! e Park n Shorobe a e k n will prevail within a society a Xaxa/Caecae/Xaixai m l e ! C u a n !( a d m a e a a b S c b K h i S " a " e a u T z 0 d ih n D 0 ' u ' m w NGAMILAND DISTRICT y ! Nxai Pan 0 m Tsokotshaa/Tsokatshaa 0 Gcwihabadu C T e Maun ° r ° h e ! 0 0 Ghwihaba/ ! a !( o 2 !( i ata Mmanxotae/Manxotae 2 g Botet N ! Gcwihaba e !( ! Nxharaga/Nxaraga !(! Maitengwe -

Copyright Government of Botswana CHAPTER 69:04
CHAPTER 69:04 - PUBLIC ROADS: SUBSIDIARY LEGISLATION INDEX TO SUBSIDIARY LEGISLATION Declaration of Public Roads and Width of Public Roads Order DECLARATION OF PUBLIC ROADS AND WIDTH OF PUBLIC ROADS ORDER (under section 2 ) (11th March, 1960 ) ARRANGEMENT OF PARAGRAPHS PARAGRAPHS 1. Citation 2. Establishment and declaration of public roads 3. Width of road Schedule G.N. 5, 1960, L.N. 84, 1966, G.N. 46, 1971, S.I. 106, 1971, S.I. 94, 1975, S.I. 95, 1975, S.I. 96, 1975, S.I. 97, 1982, S.I. 98, 1982, S.I. 99, 1982, S.I. 100, 1982, S.I. 53, 1983, S.I. 90, 1983, S.I. 6, 1984, S.I. 7, 1984, S.I. 151, 1985, S.I. 152, 1985. 1. Citation This Order may be cited as the Declaration of Public Roads and Width of Public Roads Order. 2. Establishment and declaration of public roads The roads described in the Schedule hereto are established and declared as public roads. 3. Width of road The width of every road described in the Schedule hereto shall be 30,5 metres on either side of the general run of the road. SCHEDULE Description District Distance in kilometres RAMATLABAMA-LOBATSE Southern South 48,9 East Commencing at the Botswana-South Africa border at Ramatlabama and ending at the southern boundary of Lobatse Township as shown on Plan BP225 deposited with the Director of Surveys and Lands, Gaborone. LOBATSE-GABORONE South East 65,50 Copyright Government of Botswana ("MAIN ROAD") Leaving the statutory township boundary of Lobatse on the western side of the railway and entering the remainder of the farm Knockduff No. -

Family Medicine in Botswana
10/11/2019 Objectives, 2 • To present a robust opportunity for a clinical rotation in a regional hospital that has served dozens of North American residents very well, while respecting the primacy of Botswanan learners Family Medicine in Botswana: • To present an outline for a new rotation that would take Family Successes, Challenges, and a Pathway to Collaboration Medicine residents, both American and Botswanan, into the community to build capacity in a broader context Timothy L. Herrick MD MS MA Oregon Health & Sciences University Kristen M. Otto MD MSc Oregon Health & Sciences University 4 Disclaimer Methodology • Neither Dr. Otto nor Dr. Herrick have any conflicts of interest to The information for this talk was gathered from: disclose. • Literature review • Site visits of academic and clinical teaching facilities in Gaborone, Maun, and Molepolole • Interviews with key stakeholders • Firsthand participation in existing clinical rotation 2 5 Objectives Botswana • To provide an overview of the state of Family Medicine training and • Independent from Great Britain in 1966 practice in Botswana, including successes and challenges, with a • 2.3 million people living in an area about the size of Texas view to better understanding the status quo and also understanding • Much of the area is Kalahari desert and Okavanga Delta ways that collaboration with North American family medicine could • English widely spoken, Setswana the national language be beneficial to both parties. • Strong economic development, stable government • Uneven development, reliance on diamonds, significant health care disparities, HIV/TB 3 6 1 10/11/2019 7 10 8 11 2009 Medical School begins operating 9 12 2 10/11/2019 Medical School Interns reporting for duty at Scottish Livingstone in Molepolole - Med school began in 2009 with 36 in the class. -

Botswana Non-Profits
Botswana Non-Profits Note that other than the Botswana-UPenn Partnership, we do not endorse any of the following agencies. They are listed for information purposes only as non-profit organizations that may accept volunteers. Botswana-UPenn Partnership Location: Gaborone, Botswana Mission: To help build capacity in, clinical care, education, and research. Volunteer positions: clinical researchers Contact: Andrew Steenhoff, MD [email protected] Bana ba Keletso Orphan Day Care Centre Location: Molepolole, Botswana Mission: The broad based goal of the Centre is to support the children in the community who are orphaned. This involves providing them with the necessary skills, information, and training to reduce the psychological and social effects of being orphaned, and to reduce the risk of HIV/AIDS infection. The Centre's serves as a feeding centre, preschool and centre for school going children where they can receive counseling, as well as support for school work and mentorship. Volunteer positions: Contact: http://www.orfundfoundation.com/programs/ Elephants Without Borders Location: Kasane, Botswana Mission: Elephants Without Borders is a charitable organization dedicated to conserving wildlife and natural resources; through innovative research, education, and information sharing with all people. Volunteer positions: Contact: Michael Chase Phone/Fax: ++267 625-0202 New York State Affiliate office: EWB, Inc. 168 S. Marlin Rd., Grand Island, NY 14072, USA Phone: 001 (716) 773-1012 http://www.elephantswithoutborders.org/ Flying Mission Location: Gaborone, Botswana Mission: Flying mission serves by facilitating the spread of the Gospel of Jesus Christ through aviation, training and care ministries in Botswana, Zambia, and surrounding areas. Volunteer positions: Nurses / Fundraising / IT / Web design / Support / HR / Marketing etc. -

Botswana Kweneng
Botswana Kweneng Kweneng District is located in the south-eastern part of Botswana. It borders Central District in northeast, Kgatleng District on the east, South-East District in southeast, Southern District in south, Kgalagadi District in the west, Ghanzi District in the north. The district is administered by a district administration and district council which are responsible for local administration. The seat of the district’s government is Molepolole.* Kweneng District Council (KwDC), through its Public Health Department is responsible for solid waste management in the district. KwDC provides waste collection and disposal services in some parts of the district. In other parts of the district, solid waste is collected by private operators under a franchise agreement with KwDC. In the district, there is one incineration facility (only for medical waste) and one engineered sanitary landfill located 30 kilometres from the district centre. The landfill is a regional landfill, i.e. solid waste from Kweneng District and other surrounding districts, including the capital Gaborone, are disposed at this landfill. Source: * Wikipedia, Kweneng District, accessed 15 April 2019, <https://en.wikipedia.org/wiki/Kweneng_District> Information Population 726,056 (2017) Population growth (annual %) N/A Area (km2)* 35,890 Climate Hot, semi-arid climate Main industries* Agriculture, mining, construction Currency** USD 1: BWP 10.65 (Botswana pula) (August 2018) Sources: * Wikipedia, Kweneng District, accessed 15 April 2019, <https://en.wikipedia.org/wiki/Kweneng_District> **Cuex.com Current SWM Situation Item Outline Institutional System Legal system The Waste Management Act (1998). Policy/Plan Currently, there is no waste management plan. Implementation KwDC provides sweeping, waste collection and disposal services. -

Cut-Off Date for Census of Properties Affected
MINISTRY OF TRANSPORT AND COMMUNICATIONS PUBLIC NOTICE ANNOUNCEMENT OF CUT-OFF DATE FOR CENSUS OF PROPERTIES AFFECTED BY THE PROJECT ALONG GREATER GABORONE The Ministry of Transport and Communications wishes to inform members of the public that the cut-off date to consult Project Affected Parties (PAPs) for the Design, Build and Transfer of Selected Urban Road Intersections in Greater Gaborone is 10 October 2020 at 1630 hrs. The project is preparing a Resettlement Action Plan (RAP) to facilitate compensation for the project as per the approved Project Resettlement Policy Framework. Known affected parties have been consulted individually. However, should there be any omitted Project Affected Parties (PAPs) they should immediately contact the Ministry through the following channels: Tel: 361 2000 Email: [email protected] Written letters to be addressed to: Permanent Secretary Private Bag 00414 Gaborone, Botswana Marked “Design, Build and Transfer of Selected Urban Road Intersections in Greater Gaborone” on the envelope. Or Hand Deliver to: Registry Ministry of Transport and Communications Headquarters Westgate Mall, Plot Number 54690, Western By-Pass The Ministry is currently undertaking a project for layout improvement of selected road intersections in Gaborone in order to facilitate smooth traffic flow as well as to improve pedestrian and cyclist safety. The Project entails road markings of 89 intersections, construction of additional lanes at various strategic spots within the Greater Gaborone area. This is a World Bank funded project in collaboration with the Government of the Republic of Botswana. The project will be implemented in phases and is currently at the design phase. Details of each phase are presented below. -

Public Primary Schools
PRIMARY SCHOOLS CENTRAL REGION NO SCHOOL ADDRESS LOCATION TELE PHONE REGION 1 Agosi Box 378 Bobonong 2619596 Central 2 Baipidi Box 315 Maun Makalamabedi 6868016 Central 3 Bobonong Box 48 Bobonong 2619207 Central 4 Boipuso Box 124 Palapye 4620280 Central 5 Boitshoko Bag 002B Selibe Phikwe 2600345 Central 6 Boitumelo Bag 11286 Selibe Phikwe 2600004 Central 7 Bonwapitse Box 912 Mahalapye Bonwapitse 4740037 Central 8 Borakanelo Box 168 Maunatlala 4917344 Central 9 Borolong Box 10014 Tatitown Borolong 2410060 Central 10 Borotsi Box 136 Bobonong 2619208 Central 11 Boswelakgomo Bag 0058 Selibe Phikwe 2600346 Central 12 Botshabelo Bag 001B Selibe Phikwe 2600003 Central 13 Busang I Memorial Box 47 Tsetsebye 2616144 Central 14 Chadibe Box 7 Sefhare 4640224 Central 15 Chakaloba Bag 23 Palapye 4928405 Central 16 Changate Box 77 Nkange Changate Central 17 Dagwi Box 30 Maitengwe Dagwi Central 18 Diloro Box 144 Maokatumo Diloro 4958438 Central 19 Dimajwe Box 30M Dimajwe Central 20 Dinokwane Bag RS 3 Serowe 4631473 Central 21 Dovedale Bag 5 Mahalapye Dovedale Central 22 Dukwi Box 473 Francistown Dukwi 2981258 Central 23 Etsile Majashango Box 170 Rakops Tsienyane 2975155 Central 24 Flowertown Box 14 Mahalapye 4611234 Central 25 Foley Itireleng Box 161 Tonota Foley Central 26 Frederick Maherero Box 269 Mahalapye 4610438 Central 27 Gasebalwe Box 79 Gweta 6212385 Central 28 Gobojango Box 15 Kobojango 2645346 Central 29 Gojwane Box 11 Serule Gojwane Central 30 Goo - Sekgweng Bag 29 Palapye Goo-Sekgweng 4918380 Central 31 Goo-Tau Bag 84 Palapye Goo - Tau 4950117