Kweneng District Profile
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Performance of Goats and Sheep Under Communal Grazing in Botswana Using Various Growth Measures
B07 Performance of goats and sheep under communal grazing in Botswana using various growth measures L. Baleseng, O. E Kgosikoma, A. Makgekgenene | Department of Agricultural Research, Private | Gaborone | Botswana M. Coleman, P. Morley | Institute for Rural Futures, School of Behavioural, Cognitive and Social Sciences, University of New England | Armidale | Australia D. Baker, O. | UNE Business School, University of New England | Armidale | Australia S. Bahta | International Livestock Research Institute | Nairobi | Kenya DOI: 10.1481/icasVII.2016.b07 ABSTRACT We conducted a survey to evaluate the growth of goats and sheep under communal grazing, and to determine the relationship between weight, heart girth, shoulder height, and body condition score in Kweneng, Central and Kgalagadi districts, Botswana. The same animals were measured on two separate occasions, approximately one month apart, to allow growth rates to be recorded. Significant differences in growth rates between the three case study districts were found for both goats and sheep. Amongst the goats measured, gains in height and weight were significantly greater in the Kweneng district, while gains in heart girth measurement were greatest in the Central district. In the case of sheep, weight gain was significantly higher in the Central and Kgalagadi districts, increases in girth measurement were significantly higher in the Central district, and shoulder height gain was significantly greater in the Kweneng district. Statistical tests were used to determine the relationships between animal weight and the other measures taken for goats and sheep. Heart girth in both goats and sheep was shown to be a significant predictor of weight across all three districts. Likewise, shoulder height proved to be a statistically significant predictor of animal weight for both goats and sheep, across each district. -
List of Examination Centres by Region Bobirwa Region Centr Name Addres Place Phone 0101 Bobonong Primary School P.O
Primary School Leaving Examination 2010 List of Examination Centres by Region Bobirwa Region Centr Name Addres Place Phone 0101 Bobonong Primary School P.O. Box 48 BOBONONG 2619207 0103 Borotsi Primary School P.O. Box 136 BOBONONG 819208 0107 Gobojango Primary School Private Bag 8 BOBONONG 2645436 0108 Lentswe-Le-Moriti Primary School Private Bag 0019 BOBONONG 0110 Mabolwe Primary School P.O. Box 182 SEMOLALE 2645422 0111 Madikwe Primary School P.O. Box 131 BOBONONG 2619221 0112 Mafetsakgang primary school P.O. Box 46 BOBONONG 2619232 0114 Mathathane Primary School P.O. Box 4 MATHATHANE 2645110 0117 Mogapi Primary School P.O. Box 6 MOGAPI 2618545 0119 Molalatau Primary School P.O. Box 50 MOLALATAU 845374 0120 Moletemane Primary School P.O. Box 176 TSETSEBYE 2646035 0123 Sefhophe Primary School P.O. Box 41 SEFHOPHE 2618210 0124 Semolale Primary School P.O. Box 10 SEMOLALE 2645422 0131 Tsetsejwe Primary School P.O. Box 33 TSETSEJWE 2646103 0133 Modisaotsile Primary School P.O. Box 591 BOBONONG 2619123 0134 Motlhabaneng Primary School Private Bag 20 BOBONONG 2645541 0135 Busang Primary School P.O. Box 47 TSETSEBJE 2646144 0138 Rasetimela Primary School Private Bag 0014 BOBONONG 2619485 0139 Mabumahibidu Primary School P.O. Box 168 BOBONONG 2619040 0140 Lepokole Primary School P O Box 148 BOBONONG 4900035 0141 Agosi Primary School P O Box 1673 BOBONONG 71868614 0142 Motsholapheko Primary School P O Box 37 SEFHOPHE 2618305 0143 Mathathane DOSET P.O. Box 4 MATHATHANE 2645110 0144 Tsetsebye DOSET P.O. Box 33 TSETSEBYE 3024 Bobonong DOSET P.O. Box 483 BOBONONG 2619164 Saturday, September 25, List of Examination Centres by Region Page 1 of 39 Boteti Region Centr Name Addres Place Phone 0201 Adult Education Private Bag 1 ORAPA 0202 Baipidi Primary School P.O. -

The Parliamentary Constituency Offices
REPUBLIC OF BOTSWANA THE PARLIAMENTARY CONSTITUENCY OFFICES Parliament of Botswana P O Box 240 Gaborone Tel: 3616800 Fax: 3913103 Toll Free; 0800 600 927 e - mail: [email protected] www.parliament.gov.bw Introduction Mmathethe-Molapowabojang Mochudi East Mochudi West P O Box 101 Mmathethe P O Box 2397 Mochudi P O Box 201951 Ntshinoge Representative democracy can only function effectively if the Members of Tel: 5400251 Fax: 5400080 Tel: 5749411 Fax: 5749989 Tel: 5777084 Fax: 57777943 Parliament are accessible, responsive and accountable to their constituents. Mogoditshane Molepolole North Molepolole South The mandate of a Constituency Office is to act as an extension of Parliament P/Bag 008 Mogoditshane P O Box 449 Molepolole P O Box 3573 Molepolole at constituency level. They exist to play this very important role of bringing Tel: 3915826 Fax: 3165803 Tel: 5921099 Fax: 5920074 Tel: 3931785 Fax: 3931785 Parliament and Members of Parliament close to the communities they serve. Moshupa-Manyana Nata-Gweta Ngami A constituency office is a Parliamentary office located at the headquarters of P O Box 1105 Moshupa P/Bag 27 Sowa Town P/Bag 2 Sehithwa Tel: 5448140 Fax: 5448139 Tel: 6213756 Fax: 6213240 Tel: 6872105/123 each constituency for use by a Member of Parliament (MP) to carry out his or Fax: 6872106 her Parliamentary work in the constituency. It is a formal and politically neutral Nkange Okavango Palapye place where a Member of Parliament and constituents can meet and discuss P/Bag 3 Tutume P O Box 69 Shakawe P O Box 10582 Palapye developmental issues. Tel: 2987717 Fax: 2987293 Tel: 6875257/230 Tel: 4923475 Fax: 4924231 Fax: 6875258 The offices must be treated strictly as Parliamentary offices and must therefore Ramotswa Sefhare-Ramokgonami Selibe Phikwe East be used for Parliamentary business and not political party business. -

A Heritage and Cultural Tourism Destination
MAKING GABORONE A STOP AND NOT A STOP-OVER: A HERITAGE AND CULTURAL TOURISM DESTINATION by Jane Thato Dewah (Student No: 12339556) A Dissertation submitted in fulfilment of the requirements for the degree of MAGISTER HEREDITATIS CULTURAEQUE SCIENTIAE (HERITAGE AND CULTURAL STUDIES) (TOURISM) In the Department of Historical and Heritage Studies at the Faculty of Humanities University of Pretoria SUPERVISOR: Prof. K.L Harris December 2014 DECLARATION OF AUTHENTICITY I, the undersigned, hereby declare that the work contained in this thesis is my own original work and has not been submitted previously at any other university for a degree. ............................................... Signature Jane Thato Dewah ................................................ Date ii Abstract The main objective of the study was to identify cultural heritage sites in and around Gaborone which could serve as tourist attractions. Gaborone, the capital city of Botswana, has been neglected in terms of tourism, although it has all the facilities needed to cater for this market. Very little information with regards to tourist attractions around Gaborone is available and therefore this study set out to identify relevant sites and discussed their history, relevance and potential for tourism. It also considers ways in which these sites can be developed in order to attract tourists. Due to its exclusive concentration on wildlife and the wilderness, tourism in Botswana tends to benefit only a few. Moreover, it is mainly concentrated in the north western region of the country, leaving out other parts of the country in terms of the tourism industry. To achieve the main objective of the study, which is to identify sites around the capital city Gaborone and to evaluate if indeed the sites have got the potential to become tourist attractions, three models have been used. -

Bank of Botswana
PAPER 4 BANK OF BOTSWANA DIRECTORY OF FINANCIAL INSTITUTIONS OPERATING IN BOTSWANA AS AT DECEMBER 31, 2009 PREPARED AND DISTRIBUTED BY THE BANKING SUPERVISION DEPARTMENT BANK OF BOTSWANA Foreword This directory is compiled and distributed by the Banking Supervision Department of the Bank of Botswana. While every effort has been made to ensure the accuracy of the information contained in this directory, such information is subject to frequent revision, and thus the Bank accepts no responsibility for the continuing accuracy of the information. Interested parties are advised to contact the respective financial institutions directly for any information they require. This directory excludes Collective Investment Undertakings and International Financial Services Centre non-bank entities, whose regulation and supervision have been transferred to the Non-Bank Financial Institutions Regulatory Authority. Oabile Mabusa DIRECTOR BANKING SUPERVISION DEPARTMENT 1 DIRECTORY OF FINANCIAL INSTITUTIONS OPERATING IN BOTSWANA TABLE OF CONTENTS 1. CENTRAL BANK ............................................................................................................................................. 4 2. COMMERCIAL BANKS ................................................................................................................................... 6 2.1 ABN AMRO BANK (B OTSWANA ) LIMITED ..................................................................................................... 6 2.2 ABN AMRO BANK (B OTSWANA ) OBU LIMITED ........................................................................................... -

Land Tenure Reforms and Social Transformation in Botswana: Implications for Urbanization
Land Tenure Reforms and Social Transformation in Botswana: Implications for Urbanization. Item Type text; Electronic Dissertation Authors Ijagbemi, Bayo, 1963- Publisher The University of Arizona. Rights Copyright © is held by the author. Digital access to this material is made possible by the University Libraries, University of Arizona. Further transmission, reproduction or presentation (such as public display or performance) of protected items is prohibited except with permission of the author. Download date 06/10/2021 17:13:55 Link to Item http://hdl.handle.net/10150/196133 LAND TENURE REFORMS AND SOCIAL TRANSFORMATION IN BOTSWANA: IMPLICATIONS FOR URBANIZATION by Bayo Ijagbemi ____________________ Copyright © Bayo Ijagbemi 2006 A Dissertation Submitted to the Faculty of the DEPARTMENT OF ANTHROPOLOGY In Partial Fulfillment of the Requirements For the Degree of DOCTOR OF PHILOSOPHY In the Graduate College THE UNIVERSITY OF ARIZONA 2006 2 THE UNIVERSITY OF ARIZONA GRADUATE COLLEGE As members of the Dissertation Committee, we certify that we have read the dissertation prepared by Bayo Ijagbemi entitled “Land Reforms and Social Transformation in Botswana: Implications for Urbanization” and recommend that it be accepted as fulfilling the dissertation requirement for the Degree of Doctor of Philosophy _______________________________________________________________________ Date: 10 November 2006 Dr Thomas Park _______________________________________________________________________ Date: 10 November 2006 Dr Stephen Lansing _______________________________________________________________________ Date: 10 November 2006 Dr David Killick _______________________________________________________________________ Date: 10 November 2006 Dr Mamadou Baro Final approval and acceptance of this dissertation is contingent upon the candidate’s submission of the final copies of the dissertation to the Graduate College. I hereby certify that I have read this dissertation prepared under my direction and recommend that it be accepted as fulfilling the dissertation requirement. -
Directory of Financial Institutions Operating in Botswana As at December 31, 2019
PAPER 4 BANK OF BOTSWANA DIRECTORY OF FINANCIAL INSTITUTIONS OPERATING IN BOTSWANA AS AT DECEMBER 31, 2019 PREPARED AND DISTRIBUTED BY THE BANKING SUPERVISION DEPARTMENT BANK OF BOTSWANA Foreword This directory is compiled and distributed by the Banking Supervision Department of the Bank of Botswana. While every effort has been made to ensure the accuracy of the information contained in this directory, such information is subject to frequent revision, and thus the Bank accepts no responsibility for the continuing accuracy of the information. Interested parties are advised to contact the respective financial institutions directly for any information they require. This directory excludes collective investment undertakings and International Financial Services Centre non-bank entities, whose regulation and supervision falls within the purview of the Non-Bank Financial Institutions Regulatory Authority. Lesedi S Senatla DIRECTOR BANKING SUPERVISION DEPARTMENT 2 DIRECTORY OF FINANCIAL INSTITUTIONS OPERATING IN BOTSWANA TABLE OF CONTENTS 1. CENTRAL BANK ..................................................................................................................................... 5 2. COMMERCIAL BANKS ........................................................................................................................... 7 2.1 ABSA BANK BOTSWANA LIMITED ........................................................................................................... 7 2.2 AFRICAN BANKING CORPORATION OF BOTSWANA LIMITED .................................................................. -

The Big Governance Issues in Botswana
MARCH 2021 THE BIG GOVERNANCE ISSUES IN BOTSWANA A CIVIL SOCIETY SUBMISSION TO THE AFRICAN PEER REVIEW MECHANISM Contents Executive Summary 3 Acknowledgments 7 Acronyms and Abbreviations 8 What is the APRM? 10 The BAPS Process 12 Ibrahim Index of African Governance Botswana: 2020 IIAG Scores, Ranks & Trends 120 CHAPTER 1 15 Introduction CHAPTER 2 16 Human Rights CHAPTER 3 27 Separation of Powers CHAPTER 4 35 Public Service and Decentralisation CHAPTER 5 43 Citizen Participation and Economic Inclusion CHAPTER 6 51 Transparency and Accountability CHAPTER 7 61 Vulnerable Groups CHAPTER 8 70 Education CHAPTER 9 80 Sustainable Development and Natural Resource Management, Access to Land and Infrastructure CHAPTER 10 91 Food Security CHAPTER 11 98 Crime and Security CHAPTER 12 108 Foreign Policy CHAPTER 13 113 Research and Development THE BIG GOVERNANCE ISSUES IN BOTSWANA: A CIVIL SOCIETY SUBMISSION TO THE APRM 3 Executive Summary Botswana’s civil society APRM Working Group has identified 12 governance issues to be included in this submission: 1 Human Rights The implementation of domestic and international legislation has meant that basic human rights are well protected in Botswana. However, these rights are not enjoyed equally by all. Areas of concern include violence against women and children; discrimination against indigenous peoples; child labour; over reliance on and abuses by the mining sector; respect for diversity and culture; effectiveness of social protection programmes; and access to quality healthcare services. It is recommended that government develop a comprehensive national action plan on human rights that applies to both state and business. 2 Separation of Powers Political and personal interests have made separation between Botswana’s three arms of government difficult. -

Botswana Semiology Research Centre Project Seismic Stations In
BOTSWANA SEISMOLOGICAL NETWORK ( BSN) STATIONS 19°0'0"E 20°0'0"E 21°0'0"E 22°0'0"E 23°0'0"E 24°0'0"E 25°0'0"E 26°0'0"E 27°0'0"E 28°0'0"E 29°0'0"E 30°0'0"E 1 S 7 " ° 0 0 ' ' 0 0 ° " 7 S 1 KSANE Kasane ! !Kazungula Kasane Forest ReserveLeshomo 1 S Ngoma Bridge ! 8 " ! ° 0 0 ' # !Mabele * . MasuzweSatau ! ! ' 0 ! ! Litaba 0 ° Liamb!ezi Xamshiko Musukub!ili Ivuvwe " 8 ! ! ! !Seriba Kasane Forest Reserve Extension S 1 !Shishikola Siabisso ! ! Ka!taba Safari Camp ! Kachikau ! ! ! ! ! ! Chobe Forest Reserve ! !! ! Karee ! ! ! ! ! Safari Camp Dibejam!a ! ! !! ! ! ! ! X!!AUD! M Kazuma Forest Reserve ! ShongoshongoDugamchaRwelyeHau!xa Marunga Xhauga Safari Camp ! !SLIND Chobe National Park ! Kudixama Diniva Xumoxu Xanekwa Savute ! Mah!orameno! ! ! ! Safari Camp ! Maikaelelo Foreset Reserve Do!betsha ! ! Dibebe Tjiponga Ncamaser!e Hamandozi ! Quecha ! Duma BTLPN ! #Kwiima XanekobaSepupa Khw!a CHOBE DISTRICT *! !! ! Manga !! Mampi ! ! ! Kangara # ! * Gunitsuga!Njova Wazemi ! ! G!unitsuga ! Wazemi !Seronga! !Kaborothoa ! 1 S Sibuyu Forest Reserve 9 " Njou # ° 0 * ! 0 ' !Nxaunxau Esha 12 ' 0 Zara ! ! 0 ° ! ! ! " 9 ! S 1 ! Mababe Quru!be ! ! Esha 1GMARE Xorotsaa ! Gumare ! ! Thale CheracherahaQNGWA ! ! GcangwaKaruwe Danega ! ! Gqose ! DobeQabi *# ! ! ! ! Bate !Mahito Qubi !Mahopa ! Nokaneng # ! Mochabana Shukumukwa * ! ! Nxabe NGAMILAND DISTRICT Sorob!e ! XurueeHabu Sakapane Nxai National Nark !! ! Sepako Caecae 2 ! ! S 0 " Konde Ncwima ° 0 ! MAUN 0 ' ! ! ' 0 Ntabi Tshokatshaa ! 0 ° ! " 0 PHDHD Maposa Mmanxotai S Kaore ! ! Maitengwe 2 ! Tsau Segoro -

2011 Population & Housing Census Preliminary Results Brief
2011 Population & Housing Census Preliminary Results Brief For further details contact Census Office, Private Bag 0024 Gaborone: Tel 3188500; Fax 3188610 1. Botswana Population at 2 Million Botswana’s population has reached the 2 million mark. Preliminary results show that there were 2 038 228 persons enumerated in Botswana during the 2011 Population and Housing Census, compared with 1 680 863 enumerated in 2001. Suffice to note that this is the de-facto population – persons enumerated where they were found during enumeration. 2. General Comments on the Results 2.1 Population Growth The annual population growth rate 1 between 2001 and 2011 is 1.9 percent. This gives further evidence to the effect that Botswana’s population continues to increase at diminishing growth rates. Suffice to note that inter-census annual population growth rates for decennial censuses held from 1971 to 2001 were 4.6, 3.5 and 2.4 percent respectively. A close analysis of the results shows that it has taken 28 years for Botswana’s population to increase by one million. At the current rate and furthermore, with the current conditions 2 prevailing, it would take 23 years for the population to increase by another million - to reach 3 million. Marked differences are visible in district population annual growths, with estimated zero 3 growth for Selebi-Phikwe and Lobatse and a rate of over 4 percent per annum for South East District. Most district growth rates hover around 2 percent per annum. High growth rates in Kweneng and South East Districts have been observed, due largely to very high growth rates of villages within the proximity of Gaborone. -
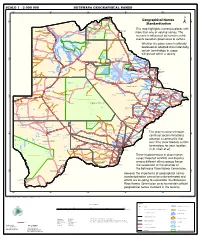
Geographical Names Standardization BOTSWANA GEOGRAPHICAL
SCALE 1 : 2 000 000 BOTSWANA GEOGRAPHICAL NAMES 20°0'0"E 22°0'0"E 24°0'0"E 26°0'0"E 28°0'0"E Kasane e ! ob Ch S Ngoma Bridge S " ! " 0 0 ' ' 0 0 ° Geographical Names ° ! 8 !( 8 1 ! 1 Parakarungu/ Kavimba ti Mbalakalungu ! ± n !( a Kakulwane Pan y K n Ga-Sekao/Kachikaubwe/Kachikabwe Standardization w e a L i/ n d d n o a y ba ! in m Shakawe Ngarange L ! zu ! !(Ghoha/Gcoha Gate we !(! Ng Samochema/Samochima Mpandamatenga/ This map highlights numerous places with Savute/Savuti Chobe National Park !(! Pandamatenga O Gudigwa te ! ! k Savu !( !( a ! v Nxamasere/Ncamasere a n a CHOBE DISTRICT more than one or varying names. The g Zweizwe Pan o an uiq !(! ag ! Sepupa/Sepopa Seronga M ! Savute Marsh Tsodilo !(! Gonutsuga/Gonitsuga scenario is influenced by human-centric Xau dum Nxauxau/Nxaunxau !(! ! Etsha 13 Jao! events based on governance or culture. achira Moan i e a h hw a k K g o n B Cakanaca/Xakanaka Mababe Ta ! u o N r o Moremi Wildlife Reserve Whether the place name is officially X a u ! G Gumare o d o l u OKAVANGO DELTA m m o e ! ti g Sankuyo o bestowed or adopted circumstantially, Qangwa g ! o !(! M Xaxaba/Cacaba B certain terminology in usage Nokaneng ! o r o Nxai National ! e Park n Shorobe a e k n will prevail within a society a Xaxa/Caecae/Xaixai m l e ! C u a n !( a d m a e a a b S c b K h i S " a " e a u T z 0 d ih n D 0 ' u ' m w NGAMILAND DISTRICT y ! Nxai Pan 0 m Tsokotshaa/Tsokatshaa 0 Gcwihabadu C T e Maun ° r ° h e ! 0 0 Ghwihaba/ ! a !( o 2 !( i ata Mmanxotae/Manxotae 2 g Botet N ! Gcwihaba e !( ! Nxharaga/Nxaraga !(! Maitengwe -

Botswana. Supervisor of Elections. . Report to the Minister of State on the General Elections, 1974
Botswana. Supervisor of Elections. Report to the Minister of State on the general elections, 1974. Gaborone, Government Printer [1974?] / 30p. 29cm. 1. Botswana-Pol. & govt. 2. Elections- Botswana. I • INDEX Page. Report to the Minister of State on the General Elections, 1974 Evaluation and Recommendations *"* Conclusion ...... 2 - • • • • 4 Title Appendix lA' A list of Constituencies, Polling Districts and Polling Stations showing the number of registered voters by constituency and polling station Appendix '/?' Authenticating Officers appointed in accordance with the Presidential Elections (Supplementary Provisions) Act >;• 12 Appendix 'C A list of Returning Officers for the Parliamentary Elections • ! l 13 Appendix Z)' A list of Returning Officers for the Local Government Elections .. ^ . 14 Appendix 'ZT Summary of the Parliamentary election results Appendix lF 17 A list of candidates in the Parliamentary Election showing the number of votes cast for each, number of votes in each constituency, and the majority gained by the winning can- didate and the percentage poll 18 Appendix '6" Summary of Local Government Election results by District or Town Council 20 Appendix 'IT A list of candidates in the Local Government election showing the number of votes cast tor each, the number of voters in each Polling District, the majority gained by the win- ning candidate, and the percentage poll / 22 Appendix T A list of political Parries registered under Section 149 of the Electoral Act 1969 30 Appendix ' J" A Report on-expenditure on the 1974 General Election 30 Sir, REPORT TO ™E MINISTER. OF STATE ON THE GENERAL ELECTIONS, 1974 SSSITOSSS: S.»=^^HS£s~rr?' Lo^l Government Election* become generally available to the public - - - > »S5S^S^as: • l^^sstsss^aSSSS^5^^-^-"5 5.