Dry Needling in the Pediatric Population
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
The Structure and Function of Breathing
CHAPTERCONTENTS The structure-function continuum 1 Multiple Influences: biomechanical, biochemical and psychological 1 The structure and Homeostasis and heterostasis 2 OBJECTIVE AND METHODS 4 function of breathing NORMAL BREATHING 5 Respiratory benefits 5 Leon Chaitow The upper airway 5 Dinah Bradley Thenose 5 The oropharynx 13 The larynx 13 Pathological states affecting the airways 13 Normal posture and other structural THE STRUCTURE-FUNCTION considerations 14 Further structural considerations 15 CONTINUUM Kapandji's model 16 Nowhere in the body is the axiom of structure Structural features of breathing 16 governing function more apparent than in its Lung volumes and capacities 19 relation to respiration. This is also a region in Fascla and resplrstory function 20 which prolonged modifications of function - Thoracic spine and ribs 21 Discs 22 such as the inappropriate breathing pattern dis- Structural features of the ribs 22 played during hyperventilation - inevitably intercostal musculature 23 induce structural changes, for example involving Structural features of the sternum 23 Posterior thorax 23 accessory breathing muscles as well as the tho- Palpation landmarks 23 racic articulations. Ultimately, the self-perpetuat- NEURAL REGULATION OF BREATHING 24 ing cycle of functional change creating structural Chemical control of breathing 25 modification leading to reinforced dysfunctional Voluntary control of breathing 25 tendencies can become complete, from The autonomic nervous system 26 whichever direction dysfunction arrives, for Sympathetic division 27 Parasympathetic division 27 example: structural adaptations can prevent NANC system 28 normal breathing function, and abnormal breath- THE MUSCLES OF RESPIRATION 30 ing function ensures continued structural adap- Additional soft tissue influences and tational stresses leading to decompensation. -

Thoracic and Lumbar Spine Anatomy
ThoracicThoracic andand LumbarLumbar SpineSpine AnatomyAnatomy www.fisiokinesiterapia.biz ThoracicThoracic VertebraeVertebrae Bodies Pedicles Laminae Spinous Processes Transverse Processes Inferior & Superior Facets Distinguishing Feature – Costal Fovea T1 T2-T8 T9-12 ThoracicThoracic VertebraeVertebrae andand RibRib JunctionJunction FunctionsFunctions ofof ThoracicThoracic SpineSpine – Costovertebral Joint – Costotransverse Joint MotionsMotions – All available – Flexion and extension limited – T7-T12 LumbarLumbar SpineSpine BodiesBodies PediclesPedicles LaminaeLaminae TransverseTransverse ProcessProcess SpinousSpinous ProcessProcess ArticularArticular FacetsFacets LumbarLumbar SpineSpine ThoracolumbarThoracolumbar FasciaFascia LumbarLumbar SpineSpine IliolumbarIliolumbar LigamentsLigaments FunctionsFunctions ofof LumbarLumbar SpineSpine – Resistance of anterior translation – Resisting Rotation – Weight Support – Motion IntervertebralIntervertebral DisksDisks RatioRatio betweenbetween diskdisk thicknessthickness andand vertebralvertebral bodybody heightheight DiskDisk CompositionComposition – Nucleus pulposis – Annulus Fibrosis SpinalSpinal LigamentsLigaments AnteriorAnterior LongitudinalLongitudinal PosteriorPosterior LongitudinalLongitudinal LigamentumLigamentum FlavumFlavum InterspinousInterspinous LigamentsLigaments SupraspinousSupraspinous LigamentsLigaments IntertransverseIntertransverse LigamentsLigaments SpinalSpinal CurvesCurves PosteriorPosterior ViewView SagittalSagittal ViewView – Primary – Secondary -

Active Release Techniques Spine Level 2
Active Release Techniques Spine Level 2 Dates of program- Montvale, NJ February 18-21, 2021 Colorado Springs, CO March 4-7, 2021 Orlando, FL June 10-13, 2021 Chicago, IL September 30 – October 3, 2021 Total Hours: 24 Summary: Active Release Techniques® Spine Level 2 offers intense training in 75 manual treatment protocols of the cervical, thoracic, and lumbar spine. ART® treatment utilizes manual techniques to move tissues and joints while under tension. The system allows for relative motion between the tissues and articulations. This seminar emphasizes the manipulation of the neuromusculoskeletal system to diagnose and correct alterations in tissue texture, tension, movement, and function between tissues. Evaluation and treatment occur simultaneously. Learning Outcomes: 1. By the end of the seminar, learners will be able to correctly identify (palpate) 75 facial seams of soft-tissue structures within the spine. 2. By the end of the seminars, learners will be able to correctly state the muscle actions of two adjacent spinal muscles. 3. By the end of the seminar, learners will be able to effectively recognize common symptom patterns of spinal neuromuscular injuries and disorders. 4. By the end of the seminar, learners will correctly identify the structure treated and associated concentric and eccentric muscle actions via video presentations. 5. By the end of the seminar, the learner will correctly move the muscle from its shortened position to elongated position using two-hand placement techniques. 6. By the end of the seminar, the learner can successfully differentiate between healthy and unhealthy tissue utilizing hands-on palpation techniques. 7. By the end of the seminar, the learner will proficiently palpate 75 anatomical soft-tissue structures within the spine, using an appropriate tension, depth, and motion to properly perform the treatment protocol. -

Trapezius Origin: Occipital Bone, Ligamentum Nuchae & Spinous Processes of Thoracic Vertebrae Insertion: Clavicle and Scapul
Origin: occipital bone, ligamentum nuchae & spinous processes of thoracic vertebrae Insertion: clavicle and scapula (acromion Trapezius and scapular spine) Action: elevate, retract, depress, or rotate scapula upward and/or elevate clavicle; extend neck Origin: spinous process of vertebrae C7-T1 Rhomboideus Insertion: vertebral border of scapula Minor Action: adducts & performs downward rotation of scapula Origin: spinous process of superior thoracic vertebrae Rhomboideus Insertion: vertebral border of scapula from Major spine to inferior angle Action: adducts and downward rotation of scapula Origin: transverse precesses of C1-C4 vertebrae Levator Scapulae Insertion: vertebral border of scapula near superior angle Action: elevates scapula Origin: anterior and superior margins of ribs 1-8 or 1-9 Insertion: anterior surface of vertebral Serratus Anterior border of scapula Action: protracts shoulder: rotates scapula so glenoid cavity moves upward rotation Origin: anterior surfaces and superior margins of ribs 3-5 Insertion: coracoid process of scapula Pectoralis Minor Action: depresses & protracts shoulder, rotates scapula (glenoid cavity rotates downward), elevates ribs Origin: supraspinous fossa of scapula Supraspinatus Insertion: greater tuberacle of humerus Action: abduction at the shoulder Origin: infraspinous fossa of scapula Infraspinatus Insertion: greater tubercle of humerus Action: lateral rotation at shoulder Origin: clavicle and scapula (acromion and adjacent scapular spine) Insertion: deltoid tuberosity of humerus Deltoid Action: -
Muscles of Mastication Muscles That Move the Head
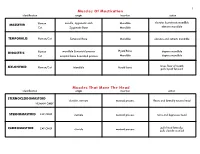
1 Muscles Of Mastication identification origin insertion action maxilla, zygomatic arch Mandible elevates & protracts mandible MASSETER Human Cat Zygomatic Bone Mandible elevates mandible TEMPORALIS Human/Cat Temporal Bone Mandible elevates and retracts mandible Hyoid Bone DIGASTRIC Human mandible & mastoid process depress mandible Cat occipital bone & mastoid process Mandible depress mandible raises floor of mouth; MYLOHYOID Human/Cat Mandible Hyoid bone pulls hyoid forward Muscles That Move The Head identification origin insertion action STERNOCLEIDOMAStoID clavicle, sternum mastoid process flexes and laterally rotates head HUMAN ONLY STERNOMAStoID CAT ONLY sternum mastoid process turns and depresses head pulls head laterally; CLEIDOMAStoID CAT ONLY clavicle mastoid process pulls clavicle craniad 2 Muscles Of The Hyoid, Larynx And Tongue identification origin insertion action Human Sternum Hyoid depresses hyoid bone STERNOHYOID Cat costal cartilage 1st rib Hyoid pulls hyoid caudally; raises ribs and sternum sternum Throid cartilage of larynx Human depresses thyroid cartilage STERNothYROID Cat costal cartilage 1st rib Throid cartilage of larynx pulls larynx caudad elevates thyroid cartilage and Human thyroid cartilage of larynx Hyoid THYROHYOID depresses hyoid bone Cat thyroid cartilage of larynx Hyoid raises larynx GENIOHYOID Human/Cat Mandible Hyoid pulls hyoid craniad 3 Muscles That Attach Pectoral Appendages To Vertebral Column identification origin insertion action Human Occipital bone; Thoracic and Cervical raises clavicle; adducts, -

The Erector Spinae Group Is a Group of 3 Sets of Muscles—Spinalis, Longissimus, and Iliocostalis
The Erector Spinae Group is a group of 3 sets of muscles—spinalis, longissimus, and iliocostalis. The spinalis group are located off of the spinous processes of the vertebrae. The longissimus group are located off of the transverse processes of the vertebrae and the iliocostalis group are located off of the ribs. By knowing these regions we can see that the spinalis group is the most medial and the iliocostalis group is most lateral. 1 During full flexion the erector spinae are relaxed. When standing upright the muscles are active and extension is initiated by the hamstrings—so when you lift a load from the bent over position it causes injury to the erector spinae group. Always lift with a straight back, not when you are hunched over. 2 3 The interspinalis muscles are very tiny muscles that connect from one spinous process to another. The intertransversarii muscles connect between each transverse process. The multifidus lies deep to the erector spinae muscles and it connects from one transverse process to the next spinous process. 4 The rotatores differs from the multifidus by going from 1 transverse process to 2 spinous processes. 5 The external obliques are the most superficial of the oblique muscles. Notice the fibers angle downward and medially, which allows for lateral flexion to same side and rotation to the opposite side. What other muscle does that (neck muscle)?? Once again it takes both sides to contract to cause trunk flexion to occur and only 1 side to cause the rotation and lateral flexion. Now the internal obliques have the fibers directed more horizontally which allows for rotation to the same side when 1 side contracts unlike the external obliques. -
EMG Analysis of Latissimus Dorsi, Erector Spinae and Middle Trapezius Muscle Activity During Spinal Rotation: a Pilot Study Jamie Flint University of North Dakota
University of North Dakota UND Scholarly Commons Physical Therapy Scholarly Projects Department of Physical Therapy 2015 EMG Analysis of Latissimus Dorsi, Erector Spinae and Middle Trapezius Muscle Activity during Spinal Rotation: A Pilot Study Jamie Flint University of North Dakota Toni Linneman University of North Dakota Rachel Pederson University of North Dakota Megan Storstad University of North Dakota Follow this and additional works at: https://commons.und.edu/pt-grad Part of the Physical Therapy Commons Recommended Citation Flint, Jamie; Linneman, Toni; Pederson, Rachel; and Storstad, Megan, "EMG Analysis of Latissimus Dorsi, Erector Spinae and Middle Trapezius Muscle Activity during Spinal Rotation: A Pilot Study" (2015). Physical Therapy Scholarly Projects. 571. https://commons.und.edu/pt-grad/571 This Scholarly Project is brought to you for free and open access by the Department of Physical Therapy at UND Scholarly Commons. It has been accepted for inclusion in Physical Therapy Scholarly Projects by an authorized administrator of UND Scholarly Commons. For more information, please contact [email protected]. ------- ---- ------------------------------- EMG ANALYSIS OF LATISSIMUS DORSI, ERECTOR SPINAE AND MIDDLE TRAPEZIUS MUSCLE ACTIVITY DURING SPINAL ROTATION: A PILOT STUDY by Jamie Flint, SPT Toni Linneman, SPT Rachel Pederson, SPT Megan Storstad, SPT Bachelor of Science in Physical Education, Exercise Science and Wellness University of North Dakota, 2013 A Scholarly Project Submitted to the Graduate Faculty of the -
Chapter 7 Body Systems
Deep Muscles of the Back and Posterior Neck 1 Responsible for neck and head extension, lateral flexion, and rotation Affect trunk movements Play a role in maintaining proper spinal curve Complex column extending from sacrum to skull In these areas, massage is most effective when applied with a slow, sustained, broad-based compressive force. 2 Superficial group of back muscles 3 Intermediate group of back muscles – serratus posterior muscles 4 Deep group of back muscles – erector spinae muscles 5 Deep group of back muscles – transversospinales and segmental muscles and suboccipital muscles 6 Deep Posterior Cervical Muscles Splenius capitis and splenius cervicis What is the referred pain pattern of the splenius capitis and splenius cervicis? To the top of the skull, the eye, and the shoulder. 8 Vertical Muscles Erector Spinae Group I Iliocostalis lumborum, iliocostalis thoracis, and iliocostalis cervicis What is the isometric function of the iliocostalis lumborum, iliocostalis thoracis, and iliocostalis cervicis? These muscles stabilize the spine and pelvis. 9 Vertical Muscles Erector Spinae Group II Longissimus thoracis, longissimus cervicis, and longissimus capitis Longissimus means “the longest”; the muscles pictured on the left relate to the thorax, neck, and head, respectively. 10 Spinalis thoracis, spinalis cervicis, and spinalis capitis What are the referred pain patterns of the spinalis thoracis, spinalis cervicis, and spinalis capitis? The scapular, lumbar, abdominal, and gluteal areas. Oblique Muscles Transversospinales Group I Semispinalis thoracis, semispinalis cervicis, and semispinalis capitis 12 Multifidus What does multifidus mean? Many split parts. What is the eccentric function of the semispinalis thoracis, semispinalis cervicis, and semispinalis capitis? These muscles engage in flexion and contralateral lateral flexion of the trunk, neck, and head. -

The Relationship Between the Angle of Curvature of the Spine and SEMG Amplitude of the Erector Spinae in Young School-Children
applied sciences Article The Relationship between the Angle of Curvature of the Spine and SEMG Amplitude of the Erector Spinae in Young School-Children Jacek Wilczy ´nski* , Przemysław Karolak, Sylwia Janecka, Magdalena Kabała and Natalia Habik-Tatarowska Department Posturology, Hearing and Balance Rehabilitation, Institute of Physiotherapy, Faculty of Medicine and Health Sciences, Jan Kochanowski University in Kielce, Al. IX Wieków Kielc 19, 25-317 Kielce, Poland * Correspondence: [email protected] Received: 11 July 2019; Accepted: 29 July 2019; Published: 1 August 2019 Abstract: The aim of the study was to analyze the relationship between the angle of spinal curvature and surface electromyography (SEMG) amplitude of the erector spinae in young school-children. A total of 251 children aged 7–8 participated in the study. The analysis involved 103 (41%) children with scoliosis, 141 (56.17%) with scoliotic posture, and seven (3.0%) with normal posture. Body posture was evaluated using the Diers formetric III 4D optoelectronic method. Analysis of SEMG amplitude of the erector spinae was performed with the Noraxon TeleMyo DTS apparatus. A significant correlation was found between the angle of spinal curvature and the SEMG amplitude of the erector spinae. The most important and statistically significant predictor of the SEMG amplitude and scoliosis angle in the scoliosis group was the standing position, chest segment, right side. The largest generalized SEMG amplitude of the erector spinae occurred in both boys and girls with scoliosis. Impaired balance of muscle tension in the erector spinae can trigger a set of changes that create a clinical and anatomopathological image of spinal curvature. -

Novel Dissection Approach of Equine Back Muscles
Published: November 19, 2018 RESEARCH ARTICLE Citation: Elbrønd V. et al. (2018). Novel dissection approach of equine back muscles: Novel dissection approach of equine back muscles: new advances in new advances in anatomy and topography - and anatomy and topography - and comparison to present literature. comparison to present literature. Science Publishing Group Journal Rikke Mark Schultz1, DVM, Vibeke Sødring Elbrønd2, DVM, Ph.D. 1(2). Author’s affiliations: Corresponding Author: 1. Equine Practice, Karlebovej 22, DK- 2980 Kokkedal. Vibeke Elbrønd Dept. of Animal and Veterinary 2. Dept. of Animal and Veterinary Sciences, Vet. Faculty, SUND, Sciences, Vet. Faculty, SUND, KU, KU, Denmark Denmark E-mail: [email protected] Abstract Keywords: back muscles, Knowledge of the anatomy and topography of the equine back are topography, m. iliocostalis, m. essential for a correct diagnosis and treatment as well as longissimus dorsi, m. spinalis communication among therapists, especially since different authors have not always agreed upon the anatomical topography of the epaxial back muscles. In this study, we performed a novel 3-D dissection procedure that focused on maintaining the integrity of the myofascial role in muscle topography. A total of 17 horses were carefully dissected, recorded and videotaped. The results revealed some interesting points. 1) The iliocostalis muscle (IL) was found to be clearly distinct from the longissimus dorsi muscle (LD) and positioned ventral to the lateral edge of LD. 2) Two distinct variations in the origin of the IL, i) from the Bogorozky tendon and the ventral epimysium of m. longissimus dorsi (LD) at the caudo-lateral region at L1 to L5, and ii) from the lumbar myofascia lateral to the lumbar transverse processes at the level of L2 to L4 have been found. -

The Lumbosacral Dorsal Rami of the Cat
J. Anat. (1976), 122, 3, pp. 653-662 653 With 1O figures Printed in Great Britain The lumbosacral dorsal rami of the cat NIKOLAI BOGDUK Department ofAnatomy, University ofSydney, Sydney, Australia (Accepted 2 December 1975) INTRODUCTION Several reflexes involving dorsal rami have been demonstrated in the cat (Pedersen, Blunck & Gardner, 1956; Bogduk & Munro, 1973). However, there is no adequate description in the literature of the anatomy of lumbosacral dorsal rami in this animal. The present study was therefore undertaken to provide such a description, hoping thereby to facilitate the design and interpretation of our own (Bogduk & Munro, 1973) and future research on reflexes involving lumbosacral dorsal rami, including reflexes possibly relevant to the understanding of back pain in man. These nerves are described in the present study in relation to a revised nomen- clature of the muscles in the dorsal lumbar region. Such a revision (Bogduk, 1975) was necessary because of the different nomenclatures and varied interpretations in the literature. METHODS Six laboratory cats (Felis domesticus) were embalmed with 10° formalin and studied by gross dissection. In addition, confirmatory observations were made on another 16 cats in the course of surgical procedures. Lateral branches of dorsal rami were first identified during reflexion of the skin and then during the resection of iliocostalis and longissimus lumborum. These branches were subsequently traced back to their origins from the dorsal rami, a dissecting microscope being used. The medial branches of the dorsal rami were then traced through the intertransversarii mediales into multifidus. Sinuvertebral nerves were also sought. Nerve roots were detached from the spinal cord before removing it from the vertebral canal. -

Passive Mechanical Properties of the Lumbar Multifidus Muscle Support Its Role As a Stabilizer$ ARTICLE in PRESS Journal of Biom
ARTICLE IN PRESS Journal of Biomechanics 42 (2009) 1384–1389 Contents lists available at ScienceDirect Journal of Biomechanics journal homepage: www.elsevier.com/locate/jbiomech www.JBiomech.com 2008 ASB Young Scientist Post-Doctoral Award Passive mechanical properties of the lumbar multifidus muscle support its role as a stabilizer$ Samuel R. Ward a,b,c, Akihito Tomiya a, Gilad J. Regev a, Bryan E. Thacker c, Robert C. Benzl a, Choll W. Kim a, Richard L. Lieber a,c,Ã a Department of Orthopaedic Surgery, University of California and Veterans Administration Medical Centers, San Diego, USA b Department of Radiology, University of California and Veterans Administration Medical Centers, San Diego, USA c Department of Bioengineering, University of California and Veterans Administration Medical Centers, San Diego, USA article info abstract Article history: The purpose of this study was to compare the passive mechanical properties and titin isoform sizes of Accepted 25 September 2008 the multifidus, longissimus, and iliocostalis muscles. Given our knowledge of each muscle’s architecture and the multifidus’ operating range, we hypothesized that multifidus would have higher elastic Keywords: modulus with corresponding smaller titin isoforms compared to longissimus or iliocostalis muscles. Lumbar multifidus Single-fiber and fiber-bundle material properties were derived from passive stress–strain tests of Muscle mechanics excised biopsies (n 47). Titin isoform sizes were quantified via sodium dodecyl sulfate-vertical ¼ Lumbar spine agarose gel electrophoresis (SDS-VAGE) analysis. We found that, at the single-fiber level, all muscles had similar material properties and titin isoform sizes. At the fiber-bundle level, however, we observed significantly increased stiffness ( 45%) in multifidus compared to longissimus and iliocostalis muscles.