Histopathological Analysis of the Progression Pattern of Subungual
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Development and Maintenance of Epidermal Stem Cells in Skin Adnexa
International Journal of Molecular Sciences Review Development and Maintenance of Epidermal Stem Cells in Skin Adnexa Jaroslav Mokry * and Rishikaysh Pisal Medical Faculty, Charles University, 500 03 Hradec Kralove, Czech Republic; [email protected] * Correspondence: [email protected] Received: 30 October 2020; Accepted: 18 December 2020; Published: 20 December 2020 Abstract: The skin surface is modified by numerous appendages. These structures arise from epithelial stem cells (SCs) through the induction of epidermal placodes as a result of local signalling interplay with mesenchymal cells based on the Wnt–(Dkk4)–Eda–Shh cascade. Slight modifications of the cascade, with the participation of antagonistic signalling, decide whether multipotent epidermal SCs develop in interfollicular epidermis, scales, hair/feather follicles, nails or skin glands. This review describes the roles of epidermal SCs in the development of skin adnexa and interfollicular epidermis, as well as their maintenance. Each skin structure arises from distinct pools of epidermal SCs that are harboured in specific but different niches that control SC behaviour. Such relationships explain differences in marker and gene expression patterns between particular SC subsets. The activity of well-compartmentalized epidermal SCs is orchestrated with that of other skin cells not only along the hair cycle but also in the course of skin regeneration following injury. This review highlights several membrane markers, cytoplasmic proteins and transcription factors associated with epidermal SCs. Keywords: stem cell; epidermal placode; skin adnexa; signalling; hair pigmentation; markers; keratins 1. Epidermal Stem Cells as Units of Development 1.1. Development of the Epidermis and Placode Formation The embryonic skin at very early stages of development is covered by a surface ectoderm that is a precursor to the epidermis and its multiple derivatives. -

Nail Anatomy and Physiology for the Clinician 1
Nail Anatomy and Physiology for the Clinician 1 The nails have several important uses, which are as they are produced and remain stored during easily appreciable when the nails are absent or growth. they lose their function. The most evident use of It is therefore important to know how the fi ngernails is to be an ornament of the hand, but healthy nail appears and how it is formed, in we must not underestimate other important func- order to detect signs of pathology and understand tions, such as the protective value of the nail plate their pathogenesis. against trauma to the underlying distal phalanx, its counterpressure effect to the pulp important for walking and for tactile sensation, the scratch- 1.1 Nail Anatomy ing function, and the importance of fi ngernails and Physiology for manipulation of small objects. The nails can also provide information about What we call “nail” is the nail plate, the fi nal part the person’s work, habits, and health status, as of the activity of 4 epithelia that proliferate and several well-known nail features are a clue to sys- differentiate in a specifi c manner, in order to form temic diseases. Abnormal nails due to biting or and protect a healthy nail plate [1 ]. The “nail onychotillomania give clues to the person’s emo- unit” (Fig. 1.1 ) is composed by: tional/psychiatric status. Nail samples are uti- • Nail matrix: responsible for nail plate production lized for forensic and toxicology analysis, as • Nail folds: responsible for protection of the several substances are deposited in the nail plate nail matrix Proximal nail fold Nail plate Fig. -
The Integumentary System
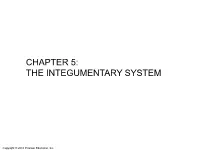
CHAPTER 5: THE INTEGUMENTARY SYSTEM Copyright © 2010 Pearson Education, Inc. OVERALL SKIN STRUCTURE 3 LAYERS Copyright © 2010 Pearson Education, Inc. Figure 5.1 Skin structure. Hair shaft Dermal papillae Epidermis Subpapillary vascular plexus Papillary layer Pore Appendages of skin Dermis Reticular • Eccrine sweat layer gland • Arrector pili muscle Hypodermis • Sebaceous (oil) gland (superficial fascia) • Hair follicle Nervous structures • Hair root • Sensory nerve fiber Cutaneous vascular • Pacinian corpuscle plexus • Hair follicle receptor Adipose tissue (root hair plexus) Copyright © 2010 Pearson Education, Inc. EPIDERMIS 4 (or 5) LAYERS Copyright © 2010 Pearson Education, Inc. Figure 5.2 The main structural features of the skin epidermis. Keratinocytes Stratum corneum Stratum granulosum Epidermal Stratum spinosum dendritic cell Tactile (Merkel) Stratum basale Dermis cell Sensory nerve ending (a) Dermis Desmosomes Melanocyte (b) Melanin granule Copyright © 2010 Pearson Education, Inc. DERMIS 2 LAYERS Copyright © 2010 Pearson Education, Inc. Figure 5.3 The two regions of the dermis. Dermis (b) Papillary layer of dermis, SEM (22,700x) (a) Light micrograph of thick skin identifying the extent of the dermis, (50x) (c) Reticular layer of dermis, SEM (38,500x) Copyright © 2010 Pearson Education, Inc. Figure 5.3a The two regions of the dermis. Dermis (a) Light micrograph of thick skin identifying the extent of the dermis, (50x) Copyright © 2010 Pearson Education, Inc. Q1: The type of gland which secretes its products onto a surface is an _______ gland. 1) Endocrine 2) Exocrine 3) Merocrine 4) Holocrine Copyright © 2010 Pearson Education, Inc. Q2: The embryonic tissue which gives rise to muscle and most connective tissue is… 1) Ectoderm 2) Endoderm 3) Mesoderm Copyright © 2010 Pearson Education, Inc. -

Sweat Glands • Oil Glands • Mammary Glands
Chapter 4 The Integumentary System Lecture Presentation by Steven Bassett Southeast Community College © 2015 Pearson Education, Inc. Introduction • The integumentary system is composed of: • Skin • Hair • Nails • Sweat glands • Oil glands • Mammary glands © 2015 Pearson Education, Inc. Introduction • The skin is the most visible organ of the body • Clinicians can tell a lot about the overall health of the body by examining the skin • Skin helps protect from the environment • Skin helps to regulate body temperature © 2015 Pearson Education, Inc. Integumentary Structure and Function • Cutaneous Membrane • Epidermis • Dermis • Accessory Structures • Hair follicles • Exocrine glands • Nails © 2015 Pearson Education, Inc. Figure 4.1 Functional Organization of the Integumentary System Integumentary System FUNCTIONS • Physical protection from • Synthesis and storage • Coordination of immune • Sensory information • Excretion environmental hazards of lipid reserves response to pathogens • Synthesis of vitamin D3 • Thermoregulation and cancers in skin Cutaneous Membrane Accessory Structures Epidermis Dermis Hair Follicles Exocrine Glands Nails • Protects dermis from Papillary Layer Reticular Layer • Produce hairs that • Assist in • Protect and trauma, chemicals protect skull thermoregulation support tips • Nourishes and • Restricts spread of • Controls skin permeability, • Produce hairs that • Excrete wastes of fingers and supports pathogens prevents water loss provide delicate • Lubricate toes epidermis penetrating epidermis • Prevents entry of -
Nails Develop from Thickened Areas of Epidermis at the Tips of Each Digit Called Nail Fields
Nail Biology: The Nail Apparatus Nail plate Proximal nail fold Nail matrix Nail bed Hyponychium Nail Biology: The Nail Apparatus Lies immediately above the periosteum of the distal phalanx The shape of the distal phalanx determines the shape and transverse curvature of the nail The intimate anatomic relationship between nail and bone accounts for the bone alterations in nail disorders and vice versa Nail Apparatus: Embryology Nail field develops during week 9 from the epidermis of the dorsal tip of the digit Proximal border of the nail field extends downward and proximally into the dermis to create the nail matrix primordium By week 15, the nail matrix is fully developed and starts to produce the nail plate Nails develop from thickened areas of epidermis at the tips of each digit called nail fields. Later these nail fields migrate onto the dorsal surface surrounded laterally and proximally by folds of epidermis called nail folds. Nail Func7on Protect the distal phalanx Enhance tactile discrimination Enhance ability to grasp small objects Scratching and grooming Natural weapon Aesthetic enhancement Pedal biomechanics The Nail Plate Fully keratinized structure produced throughout life Results from maturation and keratinization of the nail matrix epithelium Attachments: Lateral: lateral nail folds Proximal: proximal nail fold (covers 1/3 of the plate) Inferior: nail bed Distal: separates from underlying tissue at the hyponychium The Nail Plate Rectangular and curved in 2 axes Transverse and horizontal Smooth, although -

Anatomy and Physiology of the Nail
Anatomy and physiology of the nail Christian Dumontier Institut de la Main & hôpital saint Antoine, Paris Anatomy of the nail • The osteo-ligamentous support • Nail plate • All surrounding tissues, i.e. the perionychium The distal phalanx • Is reinforced laterally by the the Flint’s ligament • Which protect the neuro-vascular structures Flint’s ligament The ligamentous support • The nail is fixed onto the bone through a highly vascularized dermis • The nail is fixed onto the bone through two strong ligaments The ligamentous structures • All the ligaments merge together with • The extensor tendon • The flexor tendon • The collateral ligaments • Flint’s ligament • Guero’s dorsal ligament • (Hyponychial ligament) Clinical implications • A normal nail cannot grow on an abnormal support +++ • Large phalanx = racket nails • bony malunion = nail dystrophy • arthrosis = Pincer nail,... The nail plate • Is produced by the germinal matrix • ItsKeratinic shape depends structure, on the bonypartiall supporty transparent and the and integritycurved both of the longitudinall soft-tissuesy arandound transv it ersally • Three different layers • 0,5 mm thickness, 20% of water Clinical applications • The nail plate is often intact in crushing trauma due to its flexibility • And must be removed in order to explore all the lesions +++ The perionychium • Include all the soft- tissues located under the nail plate • Nail (germinal) matrix, • Nail bed, • Hyponychium The perionychium • Soft-tissues aroud the plate (paronychium) proximal and lateral nail wall (fold) -

The Nail Bed, Part I. the Normal Nail Bed Matrix, Stem Cells, Distal Motion and Anatomy
Central Journal of Dermatology and Clinical Research Review Article *Corresponding author Nardo Zaias, Department of Dermatology Mount Sinai Medical Center, Miami Beach, FL. 33140, 4308 The Nail Bed, Part I. The Normal Alton rd. Suite 750, USA, Email: [email protected] Submitted: 25 November 2013 Nail Bed Matrix, Stem Cells, Distal Accepted: 28 December 2013 Published: 31 December 2013 Copyright Motion and Anatomy © 2014 Zaias Nardo Zaias* OPEN ACCESS Department of Dermatology Mount Sinai Medical Center, USA Abstract The nail bed (NB) has its own matrix that originates from distinctive stem cells. The nail bed matrix stem cells (NBMSC) lie immediately distal to the nail plate (NP) matrix cells and are covered by the keratogenous zone of the most distal NPM (LUNULA). The undivided NBMS cells move distally along the NB basement membrane toward the hyponychium; differentiating and keratinizing at various locations, acting as transit amplifying cells and forming a thin layer of NB corneocytes that contact the overlying onychocytes of the NP, homologous to the inner hair root sheath. At the contact point, the NB corneocytes express CarcinoEmbryonic Antigen (CEA), a glycoprotein-modulating adherence which is also found in hair follicles and tumors. Only when both the NP and the NB are normal do they synchronously move distally. The normal NB keratinizes, expressing keratin K-5 and K-17 without keratohyaline granules. However, during trauma or disease states, it reverts to keratinization with orthokeratosis and expresses K-10, as seen in developmental times. Psoriasis is the only exception. Nail Bed epidermis can express hyperplasia and giant cells in some diseases. -

Cornification of Nail Keratinocytes Requires Autophagy for Bulk Degradation of Intracellular Proteins While Sparing Components of the Cytoskeleton
UC Davis UC Davis Previously Published Works Title Cornification of nail keratinocytes requires autophagy for bulk degradation of intracellular proteins while sparing components of the cytoskeleton. Permalink https://escholarship.org/uc/item/0fk9m9qq Journal Apoptosis : an international journal on programmed cell death, 24(1-2) ISSN 1360-8185 Authors Jaeger, Karin Sukseree, Supawadee Zhong, Shaomin et al. Publication Date 2019-02-01 DOI 10.1007/s10495-018-1505-4 Peer reviewed eScholarship.org Powered by the California Digital Library University of California Apoptosis (2019) 24:62–73 https://doi.org/10.1007/s10495-018-1505-4 Cornification of nail keratinocytes requires autophagy for bulk degradation of intracellular proteins while sparing components of the cytoskeleton Karin Jaeger1 · Supawadee Sukseree1 · Shaomin Zhong1 · Brett S. Phinney2 · Veronika Mlitz1 · Maria Buchberger1 · Marie Sophie Narzt1,3 · Florian Gruber1,3 · Erwin Tschachler1 · Robert H. Rice4 · Leopold Eckhart1 Published online: 14 December 2018 © The Author(s) 2018 Abstract Epidermal keratinocytes undergo cornification to form the cellular building blocks of hard skin appendages such as nails and the protective layer on the surface of the skin. Cornification requires the cross-linking of structural proteins and the removal of other cellular components to form mechanically rigid and inert corneocytes. Autophagy has been proposed to contribute to this intracellular remodelling process, but its molecular targets in keratinocytes, if any, have remained elusive. Here, we deleted the essential autophagy factor Atg7 in K14-positive epithelia of mice and determined by proteomics the impact of this deletion on the abundance of individual proteins in cornified nails. The genetic suppression of autophagy in keratinocytes resulted in a significant increase in the number of proteins that survived cornification and in alterations of their abundance in the nail proteome. -

•Nail Structure •Nail Growth •Nail Diseases, Disorders, and Conditions
•Nail Structure Nail Theory •Nail Growth •Nail Diseases, Disorders, and Conditions Onychology The study of nails. Nail Structure 1. Free Edge – Extends past the skin. 2. Nail Body – Visible nail area. 3. Nail Wall – Skin on both sides of nail. 4. Lunula – Whitened half-moon 5. Eponychium – Lies at the base of the nail, live skin. 6. Mantle – Holds root and matrix. Nail Structure 7. Nail Matrix – Generates cells that make the nail. 8. Nail Root – Attached to matrix 9. Cuticle – Overlapping skin around the nail 10. Nail Bed – Skin that nail sits on 11. Nail Grooves – Tracks that nail slides on 12. Perionychium – Skin around nail 13. Hyponychium – Underneath the free edge Hyponychium Nail Body Nail Groove Nail Bed Lunula Eponychium Matrix Nail Root Free Edge Nail Bed Eponychium Matrix Nail Root Nail Growth • Keratin – Glue-like protein that hardens to make the nail. • Rate of Growth – 4 to 6 month to grow new nail – Approx. 1/8” per month • Faster in summer • Toenails grow faster Injuries • Result: shape distortions or discoloration – Nail lost due to trauma. – Nail lost through disease. Types of Nail Implements Nippers Nail Clippers Cuticle Pusher Emery Board or orangewood stick Nail Diseases, Disorders and Conditions • Onychosis – Any nail disease • Etiology – Cause of nail disease, disorder or condition. • Hand and Nail Examination – Check for problems • Six signs of infection – Pain, swelling, redness, local fever, throbbing and pus Symptoms • Coldness – Lack of circulation • Heat – Infection • Dry Texture – Lack of moisture • Redness -

(Nail Care) Services
7/8 TLE BEAUTY CARE (Nail Care) SERVICES Module 4: Nail Shapes in Nail Care Services Quarter 1, Week 4 LYNNE B. GAHISAN M```````````````````````````````````````````````````````````````````````````````````````````````````````````````````````````````````````````````````````` ```````````````````````````````` (SUPPORT MATERIAL FOR INDEPENDENT LEARNING ENGAGEMENT) A Joint Project of SCHOOLS DIVISION OF DIPOLOG CITY and the DIPOLOG CITY GOVERNMENT TLE – Grade 7/8 Alternative Delivery Mode Quarter 1 – Module 4: Nail Shapes in Nail Care Services First Edition, 2020 Development Team of the Module Writer: Lynne B. Gahisan Editor: Lynne B. Gahisan Reviewers: Rosel P. Patangan Illustrator: Layout Artist: Management Team: Virgilio P. Batan Jr. – Schools Division Superintendent Jay S. Montealto – Asst. Schools Division Superintendent Amelinda D. Montero – Chief, Education Supervisor, CID Nur N. Hussien – Chief, Education Supervisor, SGOD Ronillo S. Yarag – Education Program Supervisor, LRMS Leo Martinno O. Alejo – Project Development Officer II, LRMS Printed in the Philippines by ________________________ Department of Education – Region IX –SCHOOLS DIVISION OF DIPOLOG CITY Office Address: Purok Farmers’, Olingan, Dipolog City ____________________________________________ Telefax: ____________________________________________ E-mail Address: ____________________________________________ 7/8 TLE Module 4: Nail Shapes in Nail Care Services Week 4 Learning Outcome 1: Identify Nail Structure and Shapes TLE_HEBC7/8MT-0j-6 Notes to the Teacher This contains helpful tips or strategies that will help you in guiding the learners. The following are some reminders in using this module: 1. Use the module with care. Do not put unnecessary mark/s on any part of the module. Use a separate sheet of paper in answering the exercises. 2. Don’t forget to answer What I Know before moving on to the other activities included in the module. -

433 Dermatology Team Structure of Skin
433 Dermatology Team structure of skin Lecture (4) Structure of skin [email protected] 1 | P a g e 433 Dermatology Team structure of skin Objectives: • To be familiar with the different structures of the skin. • To have basic knowledge of anatomy and function of the skin. • To be familiar with different tools to investigate skin disorders. • The relation between anatomy and diseases. • To have a general idea about different therapeutic options used in dermatology practice. Color index: slides, doctor notes, 432 notes 2 | P a g e 433 Dermatology Team structure of skin Functions of Skin: Prevent infections via innate and adaptive immunity Maintain a barrier Repair injury Provide circulation Communicate Provide nutrition Regulate temperature Attract attention Pathologies affecting functions of skin: Infections Autoimmunity Cancers Dehydration Eczema Ulcers Infarction Vasculitis Sensory neuropathy Pruritus Vitiligo Alopecia Hyperthermia Vitamin D deficiency The Skin as an organ: General structure and embryological origins Epidermis (ectoderm) Dermal- Epidermal junction is called basement membrane, Weakest part in the skin usual site of blisters Dermis (mesoderm) Subcutaneous fat and skin appendages (ectoderm and mesoderm Palms, soles, genitalia and scalp skin have slightly different structure 3 | P a g e 433 Dermatology Team structure of skin Epidermis: • Keratinocytes: 95% of the cells in epidermis. Division of these cells only occur in the basal layer where 10% of them are stem cells. • The normal transit time of a differentiating keratinocyte from basal layer to the outer surface of the stratum corneum is 28 days. (in psoriasis it is much shorter). • The epidermis doesn’t have blood vessels it obtains its nutrients from the blood vessel of dermis diffusing through the dermoeoidermal junction (papillary layer of dermis). -

The Biology and Science of Hair, Skin and Nails Hair There Are
900 E. Hill Ave Suite 380 Knoxville, TN 37915 www.athomeprep.com 1-800-952-0910 The Biology and Science of Hair, Skin and Nails Hair There are approximately 5 million hair follicles on the body with 100-150 thousand located on the scalp. By 22 weeks gestation, the fetus has all of the hair follicles that it will ever have and no more are added during its lifetime. The hair follicles are more dense as a young child and become less so as our body grows. The primary functions of hair are protection against UV rays and heat loss. Hair cells are called trichocytes and are among the most rapidly dividing cells in the body - doubling every 23-72 hours. The trichocytes are located in the hair follicle, which in turn is located in the dermis of the skin. Each hair follicle has a follicular papilla which is fed by capillaries (small blood vessels). The papilla surrounds the bulb from which the hair grows. This entire complex is located in the dermis of the skin overlying the cranium (also known as the scalp). The follicle has two layers, an outer and an inner. The outer layer continues up to the sebaceous gland and the inner follows the hair shaft and ends below the opening of the sebaceous gland. Each follicle also contains an arrector pili muscle which attaches to the outer sheath just below the sebaceous gland. This causes hair to stand on end when you are frightened or scared or cold. The sebaceous gland produces sebum which acts as a natural conditioner.