Effects of Local Handwashing Agents on Microbial
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
20210714 Access Snapshot- Tigray Region June 2021 V2
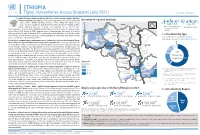
ETHIOPIA Tigray: Humanitarian Access Snapshot (July 2021) As of 31 July 2021 The conflict in Tigray continues despite the unilateral ceasefire announced by the Ethiopian Federal Government on 28 June, which resulted in the withdrawal of the Ethiopian National Overview of reported incidents July Since Nov July Since Nov Defense Forces (ENDF) and Eritrea’s Defense Forces (ErDF) from Tigray. In July, Tigray forces (TF) engaged in a military offensive in boundary areas of Amhara and Afar ERITREA 13 153 2 14 regions, displacing thousands of people and impacting access into the area. #Incidents impacting Aid workers killed Federal authorities announced the mobilization of armed forces from other regions. The Amhara region the security of aid Tahtay North workers Special Forces (ASF), backed by ENDF, maintain control of Western zone, with reports of a military Adiyabo Setit Humera Western build-up on both sides of the Tekezi river. ErDF are reportedly positioned in border areas of Eritrea and in SUDAN Kafta Humera Indasilassie % of incidents by type some kebeles in North-Western and Eastern zones. Thousands of people have been displaced from town Central Eastern these areas into Shire city, North-Western zone. In line with the Access Monitoring and Western Korarit https://bit.ly/3vcab7e May Reporting Framework: Electricity, telecommunications, and banking services continue to be disconnected throughout Tigray, Gaba Wukro Welkait TIGRAY 2% while commercial cargo and flights into the region remain suspended. This is having a major impact on Tselemti Abi Adi town May Tsebri relief operations. Partners are having to scale down operations and reduce movements due to the lack Dansha town town Mekelle AFAR 4% of fuel. -

Socio-Economic Base-Line Survey of Rural and Urban Households in Tana Sub-Basin, Amhara National Regional State
Socio-Economic Base-Line Survey of Rural and Urban Households in Tana Sub-Basin, Amhara National Regional State Kassahun Berhanu & Tegegne Gebre-Egziabher FSS Monograph No. 10 Forum for Social Studies (FSS) Addis Ababa © 2014 Forum for Social Studies (FSS) All rights reserved. Printed in Addis Ababa Typesetting & Layouts: Konjit Belete ISBN: 13: 978-99944-50-49-7 Forum for Social Studies (FSS) P.O. Box 25864 code 1000 Addis Ababa, Ethiopia Email: [email protected] Web: www.fssethiopia.org.et This monograph has been published with the financial support of the Civil Societies Support Program (CSSP). The contents of the monograph are the sole responsibilities of the authors and can under no circumstances be regarded as reflecting the position of the CSSP or the FSS. Table of Contents List of Tables vii Acronyms xvii I. INTRODUCTION 1 1.1 Background and Statement of the Problem 1 1.2 Objectives 9 1.3 Research Questions (Issues) 10 1.4 Methodology 11 1.4.1 Sampling 11 1.4.2 Types of Data, Data collection techniques, and 13 Data Sources 1.5 Significance and Policy Implications 15 1.6 Organization of the Report 15 II. POPULATION CHARACTERISTICS OF RURAL 17 HOUSHOLDS 2.1 Age-Sex Composition 17 2.2 Household Composition and Marital Status 20 2.3 Ethnic and Religious Composition 22 2.4 Educational characteristics 22 2.5 Primary Activity 25 III. AGRICULTURE 27 3.1 Crop Production 27 3.1.1 Land Ownership 27 3.1.2 Number of Plots Owned and Average Distance 28 Traveled to Farm Plots 3.1.3 Size of holding (ha) 29 3.1.4 Other Forms of Land Holding by Respondents 30 in Study Woredas 3.1.5 Possession of Private Fallow and Grazing Land 31 3.1.6 Land Use Certification and Security of Tenure 32 3.1.7 Possession of Plough Oxen 33 3.1.8 Usage of Farm Implements 33 3.1.9 Means and Ways of Engaging in Farming 34 Activities 3.1.10 Annual Production (Base Year 2004 EC) 38 3.1.11 Use of Agricultural Inputs 38 3.1.12 Irrigated Agriculture 42 3.2 Livestock Production and Services 47 IV. -

Journal of Critical Reviews SOCIAL CONDITIONS of SHINASHA TRIALS in NORTHWESTERN ETHIOPIA
Journal of Critical Reviews ISSN- 2394-5125 Vol 7, Issue 9, 2020 SOCIAL CONDITIONS OF SHINASHA TRIALS IN NORTHWESTERN ETHIOPIA 1Abebe Ano Alula, 2Arjun Rao Kuthadi (Ph.D.) 1Ph.D. candidate in Department of History, College of Social Sciences and Art Osmania University, Hyderabad, India 2Professor of History ,Supervisor, Department of History, College of Social Sciences and Art Osmania University, Hyderabad, India Received: 24.03.2020 Revised: 14.04.2020 Accepted: 22.05.2020 Abstract This article is primarily concerned to explore the social conditions of the Shinasha community in northwestern Ethiopia. Shinasha is some of the Indigenous groups with Ca. 60,587 population in Ethiopia, Africa continent, who are living Benishangul-Gumuz Regional State, near the Sudanese borderland. They have different social practices that distinguish them from others. They were part of the historical Gonga people who once lived on edges of the River Abay. Where were the early places of settlement of the Shinasha? What were the Social conditions, social changes and continuity in the Shinasha community? I address these questions by historically juxtaposing with social conditions and its dynamics with my interviews with the key informants and observations of changes in conditions of the Shinasha. This study highlights the geographic and background of the study area. The study tries to focus on the early settlement of the Shinasha and their conquest under imperial rule. It attempted to analyze the social organization of the Shinasha society. The significance of the paper is contributed to the understanding of the Social conditions and social changes and continuity of the Shinasha community in the historical outline. -

Assessment of the Invasive Alien Plant Species Argemone Ochroleuca in North Gondar and West Gojam Zones, Amhara Region, Ethiopia
International Journal of Natural Resource Ecology and Management 2016; 1(3): 107-114 http://www.sciencepublishinggroup.com/j/ijnrem doi: 10.11648/j.ijnrem.20160103.16 Assessment of the Invasive Alien Plant Species Argemone ochroleuca in North Gondar and West Gojam Zones, Amhara Region, Ethiopia Amare Seifu Assefa *, Nigussie Seboka Tadesse, Taye Birhanu Belay, Ashenafi Ayenew Hailu, Edeget Merawi Betsiha, Girum Faris Beyene, Tesfaye Bekele Hordofa, Yibrehu Emshaw Ketema Genetic Resources Access and Benefit Sharing Directorate, Ethiopian Biodiversity Institute (EBI), Addis Ababa, Ethiopia Email address: [email protected] (A. S. Assefa) *Corresponding author To cite this article: Amare Seifu Assefa, Nigussie Seboka Tadesse, Taye Birhanu Belay, Ashenafi Ayenew Hailu, Edeget Merawi Betsiha, Girum Faris Beyene, Tesfaye Bekele Hordofa, Yibrehu Emshaw Ketema. Assessment of the Invasive Alien Plant Species Argemone ochroleuca in North Gondar and West Gojam Zones, Amhara Region, Ethiopia. International Journal of Natural Resource Ecology and Management . Vol. 1, No. 3, 2016, pp. 107-114. doi: 10.11648/j.ijnrem.20160103.16 Received : July 13, 2016; Accepted : July 22, 2016; Published : August 12, 2016 Abstract: Biological invasions are attracting far reaching attention from ecologists because of their significant ecological impacts and economic costs worldwide. They are more and more recognized as a key problem of conservation of biological diversity. Argemone ochroleuca is one of invasive worldwide plant. In Ethiopia its distribution is increasing from time to time. Therefore, the objective of this study was to assess the impacts, mode of entry, trends, status, distribution and management practices of Argemone ochroleuca in selected districts of North Gondar and West Gojam Zones. -

Flood Hazard Assessment Using Multi-Criteria Evaluation Approach in Dembiya Woreda, Amhara Region, Ethiopia
ERJSSH 5(2), December 2018 ORIGINAL ARITICLE Flood Hazard Assessment Using Multi-criteria Evaluation Approach in Dembiya Woreda, Amhara Region, Ethiopia Dessie Tegegne1, Ebrahim Esa2 and Assayew Nebere3 Abstract The current climate change scenario and various studies in the past related to climate change have shown that flood impact has increased vulnerability of people in the flood plains. The aim of this study was to examine the spatial distribution of flood hazard severity in Dembiya Woreda in Amhara Region using GIS and remote sensing techniques. The study employed the multi criteria evaluation (MCE) based flood hazard severity to examine the extent and magnitude of flood hazard severity in the study area. The flood hazard mapping was undertaken using GIS and remote sensing technique to show spa- tial distribution of flood hazard severity hotspots in the study woreda. The flood hazard map obtained from the overlay analysis of flood causative factors in the study area soundly agrees to each other. The flood hazard severity map indicated that about 40777ha (32.8%) and 81350ha (65.4%) of land were subjected to high and moderate flood hazard severity, respectively. These could have a tremendous im- pact on crop production in areas that are frequently being hit by flood hazards. Therefore, multi-criteria based flood hazard assessment is vital to show spatial distributions of different severity levels of flood hazard so that the required mitigation and adaptation strategies can be implemented. Keywords: MCE, flood hazard severity, hazards mapping, GIS, Remote sensing, mitigation and adap- tation strategies Introduction Background of the Study Flooding is defined as the spilling over of the normal limits for example river, lake, sea, stream or accumulation of water as a result of heavy precipitation through lack or ex- ceeding of the discharge capacity of drains, or snow melt, dams or dikes break affecting areas which are normally not submerged (Douben and Ratnayake, 2005). -

Emergency Site Assessment: Northern Ethiopia Crisis 4 Data Collection: 2 — 23 March 2021 Publication Date: 14 April 2021 KEY FINDINGS
Emergency Site Assessment: Northern Ethiopia Crisis 4 Data Collection: 2 — 23 March 2021 Publication Date: 14 April 2021 KEY FINDINGS BACKGROUND: 1,064,176 IDPs* In early November 2020, the regional party of Tigray allegedly attacked the Northern Command of Ethiopia’s National Defense Force in Mekelle, Tigray region, prompting a military offensive from the federal government of Ethiopia. Following this, conflict broke out in the north of Ethiopia and 235,882 IDP this has displaced many from their homes. Households* OVERVIEW: From 2 — 23 March 2021, the Displacement Tracking Matrix (DTM) deployed its Emergency Site Assessment to capture internal displacement related to the Northern Ethiopia Crisis. This 178 sites multisectoral location assessment assesses the number of internally displaced persons (IDPs) and covered* collects basic information on the multisectoral needs of IDPs at site level. In this fourth round, 1,064,176 IDPs (235,882 households)* were found to be displaced across Conflict was 178 sites in Tigray, Amhara and Afar regions. 1,000,052 IDPs (218,246 households)* were found in the primary Tigray region, 45,343 IDPs (8,325 households) in Afar region and 18,781 IDPs (9,311 households) reason for in Amhara region. It should be noted that access and insecurity were considerable challenges for displacement this round. DISPLACEMENT CASELOADS IN TIGRAY, AMHARA AND AFAR REGIONS Adi Daero Chila Laelay Adiabo ERITREA TIGRAY Selekleka Shire town Asgede Adi Hageray Egela Erob Seyemti Adyabo Gulo Mekeda Tahtay Koraro Tahtay Adiyabo Ahsea -

Epidemiology of Intestinal Parasitic Infections in Preschool and School
Chelkeba et al. BMC Public Health (2020) 20:117 https://doi.org/10.1186/s12889-020-8222-y RESEARCH ARTICLE Open Access Epidemiology of intestinal parasitic infections in preschool and school-aged Ethiopian children: a systematic review and meta-analysis Legese Chelkeba1,2*, Zeleke Mekonnen3, Yonas Alemu3 and Daniel Emana3 Abstract Background: Numerous studies have been carried out on assessing the prevalence of intestinal parasites infections (IPIs) amongpreschool and school-age children in Ethiopia, but there is lack of study systematically gathered and analyzedinformation for policymakers. Therefore, the aim of this systematic review and meta-analysis was to provide a summary on prevalence, geographical distribution and trends of IPIs among preschool and school-age childrenin Ethiopia. Methods: The search were carried out in Medline via PubMed, Scopus, Science Direct, Web of Science, and Google Scholar from 1996to July2019 for studies describing prevalence of IPIs among preschooland school-age children. We conducted meta-regression to understand the trends and the source of heterogeneity and pooled the prevalence using ‘metaprop’ command using STATA software version 14. Results: Eighty-three(83) studies examining 56,786 fecal specimens were included. The prevalence of IPIs was 48%(95%CI: 42 to 53%) and showedsignificantly decreasing trends 17% (95% CI: 2.5 to 32%) for each consecutive 6 years) and was similar in males and females. The pooled prevalence in years 1997–2002, 2003–2008, 2009–2014 and > 2014 was 71% (95% CI: 57 to 86%), 42% (95% CI: 27 to 56%), 48% (95% CI: 40 to 56%) and 42% (95% CI: 34 to 49%), respectively. -
Fogera Woreda (Case 2)
Working Paper No. 2012/44 Service Delivery and State Legitimacy: Multi-Stakeholder Processes in Water and Sanitation in Ethiopia Fenta Mandefro1, Mina Noor² and Nora Stel³ November 2012 © The authors, 2012 ¹ School of Business and Public Administration – Addis Ababa University ² Maastricht School of Management ³ Maastricht School of Management The Maastricht School of Management is a leading provider of management education with worldwide presence. Our mission is to enhance the management capacity of professionals and organizations in and for emerging economies and developing countries with the objective to substantially contribute to the development of these societies. www.msm.nl The views expressed in this publication are those of the author(s). Publication does not imply endorsement by the School or its sponsors, of any of the views expressed. Further reading: - http://research.msm.nl/News/News/Latest-News/MSM-Plays-Coordination-Role-in-Peace,-Security- and.aspx - http://research.msm.nl/Research-Themes/Research-Focus-Areas/Sustainable-Development- Center/Projects/Multi-stakeholder-Processes.aspx Service Delivery and State Legitimacy: Multi-Stakeholder Processes in Water and Sanitation in Ethiopia November 2011 Research in the context of “Multi-Stakeholder Processes, Services and State Institutions” consortium – Country Report, Ethiopia Fenta Mandefro School of Business and Public Administration – Addis Ababa University With: Mina Noor and Nora Stel – Maastricht School of Management 1 Working Group Members: Maastricht School of Management Wageningen University Utrecht University Oxfam Novib Clingendael This publication is an outcome of the 2008 established „Network for Peace, Security and Development‟. The PSD Network is an initiative under the Schokland Agreements in 2007. More information on the PSD Network and other millennium agreements: www.milleniumakkoorden.nl. -

Local History of Ethiopia Ama - Amzanaghir © Bernhard Lindahl (2005)
Local History of Ethiopia Ama - Amzanaghir © Bernhard Lindahl (2005) ama, hamaa (O) honeybadger, Egyptian mongoose, Herpestes ichneumon HDM13 Ama 09°11'/39°39' 1627 m 09/39 [Gz] JDH46 Ama Yusefo 09°28'/41°18' 1587 m 09/41 [Gz] HDU52c Amad Washo (recorded in 1841) 10/39 [Ha] HEC38 Amadamit, see Amedamit amado: amedu (amädu) (A) the ashes; amed washa, ash cave; ado amo (Afar) white head JEA77 Amado (area) 11/40 [WO 20] Site in the upper Mille valley south of the volcano Gura Ale and only about a couple of square kilometres in size. In October 1973 the International Afar Research Expedition with 18 people in four LandRovers visited Amado. "Amado is noteworthy for its thick, fluviatile, crystalline tuffs containing beautiful translucent fossil wood and hundreds of monkey and baboon fossils. Coppens and Guérin judged the elephants and rhinos to be between 3 and 4 million years old. Some of the associated sediments looked like hot spring deposits, and the fossil wood looked like palm." The expedition in five days collected nearly 400 fossils, a quarter of them being monkeys. [J Kalb 2001 p 100] JEC01 Amadu (Lo Ammadu, Amadoo) (plain) 10/41 [Gu WO Ha] HCJ80 Amaia (Ammaia), see Ameya HCS44 Amairaba 07°39'/37°54' 2460 m 07/37 [WO Gz] amaja: ameja, amija (A) kind of shrub or small tree, Hypericum revolutum, H. quartinianum JDJ12 Amaja (Amagia) (saddle), see under Grawa 09/41 [+ Gu] cf Ameja, Amija ?? Amajah ../.. [Pa] A Muslim settlement in eastern Shewa, near the Kessem river, "the population of which /in the 1530s/ welcomed Grañ's forces, and prayed for the latter's victory". -

The Origin of Blin: an Overview
The Origin of Blin: an overview To be presented on the Blin Democracy and Cultural Day workshop in Stockholm, Sweden in September 09, 2006 Fitsum Asfaha Haile ([email protected]) Overview Today, in Eritrea there are three main races: Nilotic, Hamatic (Cushitic) and Semitic. These three races had had different modes of life, and physical appearances. 1. The Nilotic: They are the indigenous people of East Africa originating from the region of the Nile River, after which there are named. They have often a taller and slimmer physical appearance than the average human being. This race used to dominate most of the African parts thousands years ago before BC. They used to depend on wild fruits and hunting for their daily life. Eventually due to climate change they started to develop agriculture; and slowly they moved in towards the central highlands looking for fertile areas. Today we find some remnant cereals of this people like “Barer” and “Badenay”, which indicate that they used to grow crops. The second reason they were driven in is due to the invasion of Cushitic people from the North East Africa. Usually these people are associated with cattle herding. Currently they are found in the Sudan, Kenya, Tanzania, Uganda, Ethiopia, and Eritrea. In Eritrea they are represented by Baria (Nara) and Baden (kunama). 2. The Cushitic/Hamatic: This race is named after the Biblical figure Cush (Ham). This race entered East Africa from the North starting from Egypt to the western coastal areas of the Red Sea around 5000-3000BC (Ghaber 1995). It was the era which had witnessed severe drought. -

The Impact of Jesuit Interlude During the Seventeenth Century Ethiopia: Risks and Uncertainities
International Journal of Development in Social Sciences and Humanities http://www.ijdssh.com (IJDSSH) 2020, Vol. No. 9, Issue 1, Jan-Jun e-ISSN: 2455-5142; p-ISSN: 2455-7730 THE IMPACT OF JESUIT INTERLUDE DURING THE SEVENTEENTH CENTURY ETHIOPIA: RISKS AND UNCERTAINITIES Bitwoded Admasu Dagnaw Assistant Professor of Civics and Ethical Studies Dean of Students, University of Gondar, Maraki Campus College of Social Sciences and the Humanities University of Gondar Received:15th January, 2020; Accepted:24th January, 2020; Published:28th February,2020 ABSTRACT The notion of Ethiopia as the land of Prester John inspired the head of the Roman Catholic Church. The Ethiopian orthodox church theologian initial contacts with the Jesuits led to the critical period for the 17th century practice and development of alien religious dissemination and conversion in Ethiopia in the 16th to the mid-17th centuries under the pretext of difficult military support relationship between Roman Catholic and Ethiopian Orthodox Christianity. The Jesuits were entrusted with the anticipated conversion of the Ethiopian Orthodox within the realm of Prester John from the Monophysite spiritual sphere. In 1520 the first Portuguese delegation reached Ethiopia which became sympathy to a most fascinating encounter between incomprable religions and cultures. The Ethiopian monarchial authority, this time, was under pressure to hamper state disintegration against the wat of Ahmed Gragn. In fact, the Portuguese armed co-operation with the Ethiopian monarchy paved the way for the Portuguese deliberate interests in their regional competition with the Ottoman Turks for control of the trade routes in the Red Sea and the North-Western quarter of the Indian Ocean. -

Local History of Ethiopia Ma - Mahoya © Bernhard Lindahl (2005)
Local History of Ethiopia Ma - Mahoya © Bernhard Lindahl (2005) HES37 Ma 12°58'/38°13' 2093 m, near Deresge 12/38 [Gz] HES37 Ma Abo (church) 12°59'/38°12' 2549 m 12/38 [Gz] JEH61 Maabai (plain) 12/40 [WO] HEM61 Maaga (Maago), see Mahago HEU35 Maago 2354 m 12/39 [LM WO] HEU71 Maajeraro (Ma'ajeraro) 13°20'/39°31' 2345 m 13/39 [Gz] south of Mekele HCC.. Maale 05/36 [x] Area in Gemu-Gofa east of Jinka. In the late 1800s, Maale submitted peacefully to the army of Ras Welde Giyorgis, which had just ravaged Welayta and was continuing south-westward. The Maale, who had recently lost considerable territory in a war with their neighbours, the Bako, invited the intervention of the northerners. text D. Donham, From ritual kings to Ethiopian landlords in Maale, in The southern marches of Imperial Ethiopia, Cambridge 1986 p 69-95. ?? Maana, east of Ankar in the north-west 12/37? [n] During Februari 1941 Arthur Bentinck moved eastward to Maana and made contact with the local Patriot chief, Ras Wubneh. Bimbashi L.F. Sheppard arrived and was to take over from Bentinck who was unwell. Mission 101 North tried to win over the Kamant to the Patriot side without success. On 26 March the Kamant attacked the camp at Maana and were only driven off with difficulty by Bentinck's small force consisting of himself, Sheppard, four Sudanese, six Yemenis, and Mohamed Effendi and his banda of 25 soldiers. [Shirreff 1995 p 89, 157] JEJ40 Maandita (area) 12/41 [WO] HFF31 Maaquddi, see Meakudi maar (T) honey HFC45 Maar (Amba Maar) 14°01'/37°06' 1151 m 14/37 [Gz] HEU62 Maara 13°14'/39°35' 1940 m 13/39 [Gu Gz] JEJ42 Maaru (area) 12/41 [WO] JEJ52 Maassarra (area) 12/41 [WO] Ma.., see also Me.