Reading List 2012.Indd
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
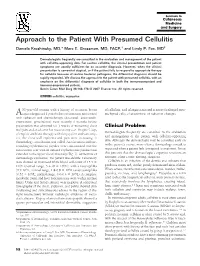
Approach to the Patient with Presumed Cellulitis Daniela Kroshinsky, MD,* Marc E
Approach to the Patient With Presumed Cellulitis Daniela Kroshinsky, MD,* Marc E. Grossman, MD, FACP,† and Lindy P. Fox, MD‡ Dermatologists frequently are consulted in the evaluation and management of the patient with cellulitic-appearing skin. For routine cellulitis, the clinical presentation and patient symptoms are usually sufficient for an accurate diagnosis. However, when the clinical presentation is somewhat atypical, or if the patient fails to respond to appropriate therapy for cellulitis because of routine bacterial pathogens, the differential diagnosis should be rapidly expanded. We discuss the approach to the patient with presumed cellulitis, with an emphasis on the differential diagnosis of cellulitis in both the immunocompetent and immunucompromised patient. Semin Cutan Med Surg 26:168-178 © 2007 Elsevier Inc. All rights reserved. KEYWORDS cellulitis, erysipelas 53-year-old woman with a history of recurrent breast of cellulitis, and telangiectasia and scattered enlarged mes- Acancer diagnosed 2 years before presentation and treated enchymal cells, characteristic of radiation changes. with radiation and chemotherapy (docetaxel, anastrozole, exemestane, gemcitabine) most recently 6 months before presentation was admitted for 3 weeks of worsening chest Clinical Problem wall pain and a rash over her mastectomy scar. Despite 5 days Dermatologists frequently are consulted in the evaluation of empiric antibiotic therapy with doxycycline and vancomy- and management of the patient with cellulitic-appearing cin, the chest wall erythema and pain were increasing. A dermatology consultation was called. An ulceration and sur- skin. Although the dermatologist may be consulted early on rounding erythematous papules were concentrated over the in the patient’s course, more often a dermatology consult is mastectomy scar with ill-defined erythematous patches that requested when a patient fails to respond to treatment. -

Bacterial Infections and Infectious Dermatologic Emergencies.Pdf
Learning Objectives Common Bacterial Infections recognition treatment complications Infectious Dermatologic Emergencies Necrotizing Fasciitis Toxic Shock Syndromes Normal Skin Flora Major function is to prevent skin infections Provides ecological competition for pathogens Hydrolyzes the lipids in sebum into free fatty acids which are toxic to many bacteria- linoleic and linolenic acid are more inhibitory of Staph Aureus Antimicrobial Peptides from lamellar bodies, Cathelicidins, and Defensins function to control overgrowth of pathogens Normal Skin Flora Aerobic Cocci Staphylococcus epidermidis Most common coccus on human skin All body sites, especially intertriginous areas Staphylococcus aureus More common in Atopic Dermatitis, Diabetes Mellitus, Hemodialysis, IVDU, Liver Disease, and HIV resident or contaminant? anterior nares- 20-35% perineum- 20% axillae and toe webs- 5-10% Normal Skin Flora Aerobic Coryneform Bacteria Corynebacterium minutissimum- intertriginous sites Erythrasma Anaerobic Coryneform Bacteria Propionibacterium acnes- sebaceous glands, hair follicles Acne vulgaris Gram Negative Bacteria Acinetobacter species- axillae, perineum, antecubital fossae - Requires moisture and maceration which increases pH and CO2 levels Yeast Pityrosporum ovale/Malassezia furfur- sebaceous sites Tinea Versicolor Introduction Strep and Staph cause the majority of skin infections in immunocompetent patients Immunodeficiency and underlying systemic disease result in severe infections which tend to be refractory to -

The Failure of the Three R's and the Future of Animal Experimentation
University of Chicago Legal Forum Volume 2006 | Issue 1 Article 7 Reduce, Refine, Replace: The aiF lure of the Three R's and the Future of Animal Experimentation Darian M. Ibrahim [email protected] Follow this and additional works at: http://chicagounbound.uchicago.edu/uclf Recommended Citation Ibrahim, Darian M. () "Reduce, Refine, Replace: The aiF lure of the Three R's and the Future of Animal Experimentation," University of Chicago Legal Forum: Vol. 2006: Iss. 1, Article 7. Available at: http://chicagounbound.uchicago.edu/uclf/vol2006/iss1/7 This Article is brought to you for free and open access by Chicago Unbound. It has been accepted for inclusion in University of Chicago Legal Forum by an authorized administrator of Chicago Unbound. For more information, please contact [email protected]. Reduce, Refine, Replace: The Failure of the Three R's and the Future of Animal Experimentation DarianM Ibrahimt The debate in animal ethics is defined by those who advocate the regulation of animal use and those who advocate its aboli- tion.' The animal welfare approach, which focuses on regulating animal use, maintains that humans have an obligation to treat animals "humanely" but may use them for human purposes.2 The animal rights approach, which focuses on abolishing animal use, argues that animals have inherent moral value that is inconsis- tent with us treating them as property.3 The animal welfare approach is the dominant model of ani- mal advocacy in the United States.4 Animal experimentation provides a fertile ground for testing this model because a unique confluence of factors make experimentation appear susceptible to meaningful regulation. -

(Gekko Gecko LINNAEUS, 1758) Saliva on Angiogenesis
Jurnal Biologi Indonesia 13(2): 253-260 (2017) Effect of Tokay Gecko (Gekko gecko LINNAEUS, 1758) Saliva on Angiogenesis During Wound Healing Phase of Autotomized Tail in Common Sun Skink (Eutropis multifasciata KUHL, 1820) (Pengaruh Saliva Tokek (Gekko gecko, LINNEAUS 1758) Terhadap Angiogenesis Pada Fase Penyembuhan Luka Ekor Kadal Kebun (Eutropis multifasciata KUHL, 1820) Setelah Autotomi) Nurul Inayah1,2, Nyoman Puniawati Soesilo2 & Rarastoeti Pratiwi3 (1)Zoology Division, Research Center for Biology-Indonesian Institute of Sciences (LIPI) (2,3) Faculty of Biology, Gadjah Mada University Email: [email protected] Received: December 2016, Accepted: June 2017 ABSTRACT The purpose of this study was to investigate the effect of Tokay gecko saliva on morphology and angiogenesis response on the healing process of skink tail wound and also to characterize the protein profile of Gecko saliva. Twelve skinks were autotomized and wound surface of tail smeared by young gecko saliva, adult gecko saliva, and human’s saliva twice per day and control. The morphological changes of the wound surface were observed. The angiogenesis response was observed in vitro using Chorioallantois Membrane (CAM) of the ninth day's chick embryos. Protein profile of gecko saliva analyzed with SDS-PAGE. Generally, treated wound showed a better healing. Young gecko saliva able to stimulate angiogenesis in wound healing stage of sun skink tail after autotomy. Saliva protein of young and adult Gecko differences was not only in the size (or density) but also in the number of the bands. The young and adult Gecko revealed a striking consistency of protein patterns, indicating a profound physiological stability of the whole saliva. -

World Journal of Clinical Pediatrics
World Journal of W J C P Clinical Pediatrics Submit a Manuscript: http://www.f6publishing.com World J Clin Pediatr 2018 October 25; 7(4): 89-104 DOI: 10.5409/wjcp.v7.i4.89 ISSN 2219-2808 (online) REVIEW Perianal infectious dermatitis: An underdiagnosed, unremitting and stubborn condition Elena Daniela Serban Elena Daniela Serban, 2nd Department of Pediatrics, “Iuliu ficial inflammation of the perianal skin, which is of bac Hatieganu” University of Medicine and Pharmacy, Emergency terial origin (classically, group A betahemolytic strepto Hospital for Children, Cluj-Napoca 400177, Romania cocci). This narrative review aims to critically review and summarize the available scientific literature regarding ORCID number: Elena Daniela Serban (0000-0003-0906-1232). pediatric PID, being the first of its kind, to the best of Author contributions: Serban ED contributed to the paper’s the author’s knowledge. It also reports the first cases of conception and design, the data collection, extraction, analysis Romanian children with PID. Multiple databases were and evaluation, the interpretation of results, and the manuscript’s subjected to systematic literature search (from 1966 preparation, critical revision, editing and final submission. to April 30, 2018) to identify studies and case reports of children with PID. As such, this review provides up Conflict-of-interest statement: The author declares there are no dated information about essential aspects of PID (epi potential conflicts of interest relevant to this publication. demiology, etiology, pathogenesis, as well as clinical OpenAccess: This article is an open-access article which was features, required investigations and therapeutic options) selected by an in-house editor and fully peer-reviewed by external and of diagnostic pitfalls. -

Extracellular Vesicles in Skin Wound Healing
Preprints (www.preprints.org) | NOT PEER-REVIEWED | Posted: 2 August 2021 doi:10.20944/preprints202108.0004.v1 Review Extracellular vesicles in skin wound healing Deimantė Narauskaitė1#, Gabrielė Vydmantaitė1#, Justina Rusteikaitė2, Revathi Sampath2, Akvilė Rudaitytė1, Ga- bija Stašytė1, María Isabel Aparicio Calvente1, Aistė Jekabsone1,2*, 1 Laboratory of Pharmaceutical Sciences, Institute of Pharmaceutical Technologies, Faculty of Pharmacy, Medical Academy, Lithuanian University of Health Sciences, Kaunas, Lithuania; D.N.- [email protected]; [email protected]; [email protected]; G.S.- [email protected]; [email protected]; [email protected] 2 Preclinical Research Laboratory for Medicinal Products, Institute of Cardiology, Lithuanian University of Health Sciences, Kaunas, Lithuania; [email protected]; [email protected] # Contributed equally * Correspondence: [email protected]; Tel.: +370 675 94455 Abstract: Each year, millions of individuals suffer from a non-healing wound, abnormal scarring, or injuries accompanied by an infection. For these cases, scientists are searching for new therapeutic interventions, from which one of the most promising is the use of extracellular vesicles (EVs). Naturally, EV-based signalling takes part in all four wound healing phases: hemostasis, inflammation, proliferation and remodelling. Such an extensive involvement of EVs suggests exploiting their action to modulate the impaired healing phase. Furthermore, -
Evidence-Based Management of Skin and Soft-Tissue Infections In
VISIT US AT BOOTH # 203 AT THE ACEP PEDIATRIC ASSEMBLY IN NEW YORK, NY, MARCH 24-25, 2015 February 2015 Evidence-Based Management Volume 12, Number 2 Authors Of Skin And Soft-Tissue Jennifer E. Sanders, MD Pediatric Emergency Medicine Fellow, Department of Emergency Medicine, Icahn School of Medicine at Mount Sinai, Infections In Pediatric Patients New York, NY Sylvia E. Garcia, MD Assistant Professor of Pediatrics and Pediatric Emergency In The Emergency Department Medicine, Icahn School of Medicine at Mount Sinai, New York, NY Abstract Peer Reviewers Jeffrey Bullard-Berent, MD, FAAP, FACEP Skin and soft-tissue infections are among the most common condi- Health Sciences Professor, Emergency Medicine and Pediatrics, University of California – San Francisco, Benioff tions seen in children in the emergency department. Emergency de- Children’s Hospital, San Francisco, CA partment visits for these infections more than doubled between 1993 Carla Laos, MD, FAAP and 2005, and they currently account for approximately 2% of all Pediatric Emergency Medicine Physician, Dell Children’s Hospital, Austin, TX emergency department visits in the United States. This rapid increase CME Objectives in patient visits can be attributed largely to the pervasiveness of community-acquired methicillin-resistant Staphylococcus aureus. The Upon completion of this article, you should be able to: 1. Describe the pathophysiology of community-acquired emergence of this disease entity has created a great deal of controver- methicillin-resistant Staphylococcus aureus. sy regarding treatment regimens for skin and soft-tissue infections. 2. Differentiate the clinical presentation of common skin and soft-tissue infections. This issue of Pediatric Emergency Medicine Practice will focus on the 3. -

UNIVERSITY of CALIFORNIA RIVERSIDE Causes And
UNIVERSITY OF CALIFORNIA RIVERSIDE Causes and Consequences of Parasitism in the California Fiddler Crab, Uca Crenulata A Dissertation submitted in partial satisfaction of the requirements for the degree of Doctor of Philosophy in Evolution, Ecology, and Organismal Biology by Adrienne Brooke Mora December 2013 Dissertation Committee: Dr. Marlene Zuk, Chairperson Dr. Daphne Fairbairn Dr. Bradley Mullens Copyright by Adrienne Brooke Mora 2013 The Dissertation of Adrienne Brooke Mora is approved: _______________________________________________ _______________________________________________ _______________________________________________ Committee Chairperson University of California, Riverside ! ACKNOWLEDGEMENTS I owe a large debt of gratitude to the many people who contributed to the completion of this dissertation. First and foremost, I would like to thank my advisor, Dr. Marlene Zuk. Marlene, you always encouraged me to push myself and taught me to develop my own voice and mind. You were also a strong advocate for my research, and with your support I was inspired to reach beyond my comfort zone and take on new challenges that greatly contributed to my intellectual and personal growth. I would also like to thank Dr. Daphne Fairbairn for her help and guidance throughout my graduate career. Daphne, you gave me great insights into the life of an academic, and helped me learn to think critically and set high standards for myself. When my working space was jeopardized, you jumped in and offered your lab space to me. I am forever grateful to you for your support during this time, as I would not have been able to complete my experiments were it not for you. I consider both you and Marlene to be great role models. -
56 AAVLD Diagnostic Pathology Slide Session
56th AAVLD Diagnostic Pathology Slide Session American Association of Veterinary Laboratory Diagnosticians San Diego, California Saturday, October 19, 2013 3:30-6:00 PM 56th AAVLD Diagnostic Pathology Slide Seminar 56thAAVLD Diagnostic Pathology Slide Session October 19, 2013 San Diego, California 2013 AAVLD Diagnostic Pathology Slide Seminar Presenters Case # Presenter Species Institution 1 Marcia R. S. Ilha Canine TVDIL-UGA 2 Alison Tucker Swine NCVDLS 3 Scott D. Fitzgerald Raccoon DCPAH-MSU 4 Bailey L. Wilberts Bovine ISU 5 Kelly Hughes Canine OSU-VDL 6 Dodd Sledge Chicken DCPAH-MSU 7 Tuddow Thaiwong Canine DCPAH-MSU 8 Kelli Almes Feline KSVDL-KSU 9 Chanran Ganta Swine KSVDL-KSU 10 Mahogany Caesar Equine NCVDLS 11 Panayiotis Loukopoulos Pacific gopher snake CAHFS-UCDavis 12 Andrew Brooks Canine AHL-UofG 13 Donal O’Toole Canine WSVL-UW 14 Sandra Scholes Bovine AHVLA 15 Leslie W. Woods Pacific fisher CAHFS-UCDavis 16 Francisco A. Uzal Bovine CAHFS-UCDavis 17 Jeffrey R. Hayes Swine Ohio ADDL 18 Tim Cushing Feline CVDC 2 56th AAVLD Diagnostic Pathology Slide Seminar 56thAAVLD Diagnostic Pathology Slide Session October 19, 2013 San Diego, California 2013 AAVLD Diagnostic Pathology Slide Seminar Diagnoses Case # Presenter Species Diagnosis Page # 1 Ilha Canine Extra-adrenal paraganglioma 4 2 Tucker Swine Idiopathic vesicular disease of swine 5 3 Fitzgerald Raccoon Canine distemper and infectious canine hepatitis 6 4 Wilberts Bovine Mannheimiosis and adenoviral infection 7 5 Hughes Canine Canine meningeal polyarteritis 8-9 6 Sledge Chicken -

Acute Wound Healing Potential of Marine Worm, Diopatra Claparedii Grube, 1878 Aqueous Extract on Sprague Dawley Rats
Hindawi Evidence-Based Complementary and Alternative Medicine Volume 2020, Article ID 6688084, 14 pages https://doi.org/10.1155/2020/6688084 Research Article Acute Wound Healing Potential of Marine Worm, Diopatra claparedii Grube, 1878 Aqueous Extract on Sprague Dawley Rats Nor ‘Awatif Che Soh,1,2 Hannah Syahirah Rapi,1,2 Nurul Shahirah Mohd Azam,1,2 Ramesh Kumar Santhanam,3 Suvik Assaw,3 Mohd Nizam Haron,4 Abdul Manaf Ali,5 M. Maulidiani ,3 Izwandy Idris ,6 and Wan Iryani Wan Ismail 1,2 1Cell Signaling and Biotechnology Research Group (CeSBTech), Faculty of Science and Marine Environment, Universiti Malaysia Terengganu, 21030 Kuala Nerus, Terengganu, Malaysia 2Biological Security and Sustainability (BioSeS) Research Group, Faculty of Science and Marine Environment, Universiti Malaysia Terengganu, 21030 Kuala Nerus, Terengganu, Malaysia 3Faculty of Science and Marine Environment, Universiti Malaysia Terengganu, 21030 Kuala Nerus, Terengganu, Malaysia 4School of Animal Science, Faculty of Bioresources and Food Industry, Universiti Sultan Zainal Abidin, 22200 Besut, Terengganu, Malaysia 5School of Agriculture Science and Biotechnology, Faculty of Bioresources and Food Industry, Universiti Sultan Zainal Abidin, 22200 Besut, Terengganu, Malaysia 6South China Sea Repository and Reference Centre, Institute of Oceanography and Environment (INOS), Universiti Malaysia Terengganu, Kuala Terengganu, Terengganu, Malaysia Correspondence should be addressed to Wan Iryani Wan Ismail; [email protected] Received 20 October 2020; Revised 27 November 2020; Accepted 4 December 2020; Published 28 December 2020 Academic Editor: Newman Osafo Copyright © 2020 Nor ‘Awatif Che Soh et al. *is is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. -

2016 AALAS National Meeting Charlotte, North Carolina
Journal of the American Association for Laboratory Animal Science Vol 55, No 5 Copyright 2016 September 2016 by the American Association for Laboratory Animal Science Pages 606–710 Abstracts of Scientific Presentations 2016 AALAS National Meeting Charlotte, North Carolina Poster Sessions blood collection method called the “one man.” The rat is manually restrained and bled by one person. In preparation for this technique, P1 A Novel Vascular Button Connection Using Combined Tech- rats are handled daily. The increase in handling reduces the amount nologies while Allowing for Social Enrichment by Pair Housing of stress the animal will have while being restrained. To restrain the animal is held in a vertical position and is grasped under each axilla, AJ Hehman*1, A Zuvich1, KA Adams2, D Shuey1 using the thumb and middle finger. The pad of the forefinger is used to pull the head back. To aid in visualizing the jugular vein, the 1Toxicology, Incyte Corporation, Wilmington, DE; 2Laboratory thoracic portion of the rat’s chest is shaved and wiped with an Animal Resources, Incyte Corporation, Wilmington, DE alcohol. Once the vein is located, a 25g needle attached to a 1 or 3mL syringe is inserted into the vessel and a blood sample obtained. After Traditional practice has been to single-house vessel-cannulated the appropriate amount of blood is collected, the needle is removed rodents post surgically to protect exposed exteriorized catheters. A and digital pressure is applied. A sample size of up to 2mLs can be port/protective cap model is available that allows for pair and group obtained. -

Supplementary Information for 'Effect of Common Infections on the Incidence of Post-Stroke Dementia: a Cohort Study Using
Supplementary information for ‘Effect of common infections on the incidence of post-stroke dementia: a cohort study using the Clinical Practice Research Datalink’ Contents Appendix 1: Read code lists for major infections (lower respiratory tract infection, urinary tract infection, skin and soft tissue infection) ........................................................................... 2 LRTI codelist ........................................................................................................................... 2 UTI codelist ............................................................................................................................ 7 SSTI codelist ........................................................................................................................... 9 Appendix 2: Read code list for dementia................................................................................. 15 Appendix 3: Multivariable Cox regression models for early and late dementia by all characteristics included in analysis .......................................................................................... 19 Appendix 4: Multivariable Cox regression model for sensitivity analysis excluding infections in first 3 months ....................................................................................................................... 20 Appendix 5: Multivariable Cox regression model for effect of first infection type on dementia .................................................................................................................................