Development and Validation of an Index Based on EAT-Lancet Recommendations: the Planetary Health Diet Index
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Negrutiu Et Al Resource Planetary Health Toolbox 12 05 2021.Odt
The Resource - Planetary Health Toolbox – taking the long view and a science-policy agenda for the next decade Ioan Negrutiu1*, Gérard Escher2, Jason D Whittington3, Ole P Ottersen4, Philippe Gil- let2, Nils C Stenseth3 1 Institut Michel Serres, RDP-IXXI, École Normale Supérieure de Lyon, France 2 Office of the president and Earth and Planetary Science Laboratory, EPFL - École Polytech- nique Fédérale de Lausanne, Switzerland 3Centre for Ecological and Evolutionary Synthesis (CEES), Department of Biosciences, Uni- versity of Oslo, Norway 4 Karolinska Institutet, Stockholm, Sweden * Correspondence : Ioan Negrutiu [email protected] Keywords: Adjusting needs and resources; Accounting and accountability; Convergence; Cultural shift; Demography; Ecological degrowth; Evidence-informed decision; Human rights and duties; Planetary health; Resource justice; State shift; Time boundary; Universal social protection floor. Abstract (218) Nature’s goods and services are the foundation of life and health. Humans are strongly health-minded, and are individually and collectively resource-driven. However, humans do not frame resources properly and the environmental crisis reflects the unsustainable manage- ment of resources, the signature landmark of the Great Acceleration in the Anthropocene. Current governance systems are not equipped to handle challenges such as the implementa- tion of the Sustainable Development Goals, as resource governance across sectors and institu- tions does not exist. To bring our governance systems more in line with sustainable use of and fair access to resources, the main question is: How to allocate accessible resources in ways that reconcile the basic needs of populations with the maintenance of the life-support functions of ecosystems? Here we describe a novel resource systems approach that integrates three principles (resource stewardship, human rights, and human duties) with the concept of planetary health (health for individuals, societies, and ecosystems). -

Eating a Low-Fiber Diet
Page 1 of 2 Eating a Low-fiber Diet What is fiber? Sample Menu Fiber is the part of food that the body cannot digest. Breakfast: It helps form stools (bowel movements). 1 scrambled egg 1 slice white toast with 1 teaspoon margarine If you eat less fiber, you may: ½ cup Cream of Wheat with sugar • Reduce belly pain, diarrhea (loose, watery stools) ½ cup milk and other digestive problems ½ cup pulp-free orange juice • Have fewer and smaller stools Snack: • Decrease inflammation (pain, redness and ½ cup canned fruit cocktail (in juice) swelling) in the GI (gastro-intestinal) tract 6 saltine crackers • Promote healing in the GI tract. Lunch: For a list of foods allowed in a low-fiber diet, see the Tuna sandwich on white bread back of this page. 1 cup cream of chicken soup ½ cup canned peaches (in light syrup) Why might I need a low-fiber diet? 1 cup lemonade You may need a low-fiber diet if you have: Snack: ½ cup cottage cheese • Inflamed bowels 1 medium apple, sliced and peeled • Crohn’s disease • Diverticular disease Dinner: 3 ounces well-cooked chicken breast • Ulcerative colitis 1 cup white rice • Radiation therapy to the belly area ½ cup cooked canned carrots • Chemotherapy 1 white dinner roll with 1 teaspoon margarine 1 slice angel food cake • An upcoming colonoscopy 1 cup herbal tea • Surgery on your intestines or in the belly area. For informational purposes only. Not to replace the advice of your health care provider. Copyright © 2007 Fairview Health Services. All rights reserved. Clinically reviewed by Shyamala Ganesh, Manager Clinical Nutrition. -

Celiac Disease Resource Guide for a Gluten-Free Diet a Family Resource from the Celiac Disease Program
Celiac Disease Resource Guide for a Gluten-Free Diet A family resource from the Celiac Disease Program celiacdisease.stanfordchildrens.org What Is a Gluten-Free How Do I Diet? Get Started? A gluten-free diet is a diet that completely Your first instinct may be to stop at the excludes the protein gluten. Gluten is grocery store on your way home from made up of gliadin and glutelin which is the doctor’s office and search for all the found in grains including wheat, barley, gluten-free products you can find. While and rye. Gluten is found in any food or this initial fear may feel a bit overwhelming product made from these grains. These but the good news is you most likely gluten-containing grains are also frequently already have some gluten-free foods in used as fillers and flavoring agents and your pantry. are added to many processed foods, so it is critical to read the ingredient list on all food labels. Manufacturers often Use this guide to select appropriate meals change the ingredients in processed and snacks. Prepare your own gluten-free foods, so be sure to check the ingredient foods and stock your pantry. Many of your list every time you purchase a product. favorite brands may already be gluten-free. The FDA announced on August 2, 2013, that if a product bears the label “gluten-free,” the food must contain less than 20 ppm gluten, as well as meet other criteria. *The rule also applies to products labeled “no gluten,” “free of gluten,” and “without gluten.” The labeling of food products as “gluten- free” is a voluntary action for manufacturers. -

Confounding Factors in Discussions About What We Should Eat to Decrease Climate Change and Ensure Sustainable Food for All, Now and in the Future
Discussion document being compiled for Climate Friendly Bradford on Avon (CFBoA). (To be completed.) Ros Edwards, Lead for the CFBoA Sustainable Food and Drink Group 30.07.2019 Draft (Vs 1.3) of Confounding Factors in discussions about what we should eat to decrease climate change and ensure sustainable food for all, now and in the future. What gets in the way of communication and clarity around the issues? Sections: 1. The complexity of the issues P. 2 2. The way that the carbon footprint (CFP) of food is measured 2 3. Difficulty squaring the circle 4 4. Emissions: getting things in perspective 9 • UK Greenhouse Gas Emissions 9 • Other emissions related to the UK food chain not reflected in these figures 11 • Biogenic methane: when does methane count as a greenhouse gas? 12 5. Beans and pulses 15 6. Health recommendations on red meat and some studies into adequate nutrient intake 16 7. Dietary inclusions and exclusions 19 • Opening up the discussion 20 • What about vegetarianism? 21 • What about veganism? 22 • What about pescetarianism? 25 • The beef question 25 • Lab meat 27 8. Grassland versus cropland foods: food security 30 9. What about carbon storage in the soil and the fertility of the soil? 31 10. Land Use 11. Biodiversity 12. Food loss and Food Waste 41 13. Bioenergy 14. Conclusions 1 1) The complexity of the issues. 2) The way that the carbon footprint (CFP) of food is measured. This issue confounds all. It seems that the measures used to assess the carbon footprint almost always show that more intensively produced food is associated with a lower carbon footprint, which leads to a strong suspicion that many factors are not being taken into account. -
Eating for 2 Degrees New and Updated Livewell Plates Summary Report © J Oh N D a I E Ls / WWF
EATING FOR 2 DEGREES NEW AND UPDATED LIVEWELL PLATES SUMMARY REPORT © J OH N D A N I E LS / WWF Cover photo © Kelly Sillaste / Getty Images / WWF Contributors Gerard Kramer, Bart Durlinger, Lody Kuling, Willem-Jan van Zeist, Hans Blonk, Roline Broekema, Sarah Halevy Design madenoise.com CONTENTS May 2017 FOREWORD .............................................................................................4 About WWF KEY FINDINGS ........................................................................................6 WWF is the world’s leading independent conservation organisation. We’re CAll TO ACTION ...................................................................................7 creating solutions to the most important environmental challenges facing the WHAT WE SET OUT TO DO ...............................................................8 planet. We work with communities, businesses and governments in over METHODOLOGY .....................................................................................9 100 countries to help people and nature thrive. Together, we’re safeguarding the LIVEWell PRINCIPLES .................................................................... 10 natural world, tackling dangerous climate change and enabling people to use only ADULT 2020 PlATE ...........................................................................11 their fair share of natural resources. ADULT 2030 PlATE .......................................................................... 12 Food is at the heart of many key environmental issues -

Genotypic Characterization and Molecular Evolution of Avian Reovirus in Poultry Flocks from Brazil
Avian Pathology ISSN: (Print) (Online) Journal homepage: https://www.tandfonline.com/loi/cavp20 Genotypic characterization and molecular evolution of avian reovirus in poultry flocks from Brazil Silvia De Carli , Jonas Michel Wolf , Tiago Gräf , Fernanda K. M. Lehmann , André S. K. Fonseca , Cláudio W. Canal , Vagner R. Lunge & Nilo Ikuta To cite this article: Silvia De Carli , Jonas Michel Wolf , Tiago Gräf , Fernanda K. M. Lehmann , André S. K. Fonseca , Cláudio W. Canal , Vagner R. Lunge & Nilo Ikuta (2020): Genotypic characterization and molecular evolution of avian reovirus in poultry flocks from Brazil, Avian Pathology, DOI: 10.1080/03079457.2020.1804528 To link to this article: https://doi.org/10.1080/03079457.2020.1804528 View supplementary material Published online: 14 Sep 2020. Submit your article to this journal Article views: 83 View related articles View Crossmark data Full Terms & Conditions of access and use can be found at https://www.tandfonline.com/action/journalInformation?journalCode=cavp20 AVIAN PATHOLOGY https://doi.org/10.1080/03079457.2020.1804528 ORIGINAL ARTICLE Genotypic characterization and molecular evolution of avian reovirus in poultry flocks from Brazil Silvia De Carlia,c, Jonas Michel Wolfa, Tiago Gräfb, Fernanda K. M. Lehmanna, André S. K. Fonsecad, Cláudio W. Canalc, Vagner R. Lungea,d and Nilo Ikutaa,d aLaboratório de Diagnóstico Molecular, Programa de Pós-Graduação em Biologia Celular e Molecular aplicada à Saúde, Universidade Luterana do Brasil (ULBRA), Canoas, Brazil; bInstituto Gonçalo Moniz, Fundação Oswaldo Cruz, Salvador, Brazil; cLaboratório de Virologia, Faculdade de Veterinária, Universidade Federal do Rio Grande do Sul, Porto Alegre, Brazil; dSimbios Biotecnologia, Cachoeirinha, Brazil ABSTRACT ARTICLE HISTORY Avian reovirus (ARV) is one of the main causes of infectious arthritis/tenosynovitis and Received 2 April 2020 malabsorption syndrome (MAS) in poultry. -
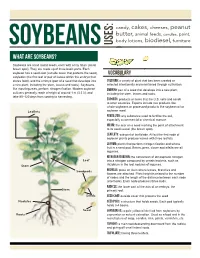
What Are Soybeans?
candy, cakes, cheeses, peanut butter, animal feeds, candles, paint, body lotions, biodiesel, furniture soybeans USES: What are soybeans? Soybeans are small round seeds, each with a tiny hilum (small brown spot). They are made up of three basic parts. Each soybean has a seed coat (outside cover that protects the seed), VOCABULARY cotyledon (the first leaf or pair of leaves within the embryo that stores food), and the embryo (part of a seed that develops into Cultivar: a variety of plant that has been created or a new plant, including the stem, leaves and roots). Soybeans, selected intentionally and maintained through cultivation. like most legumes, perform nitrogen fixation. Modern soybean Embryo: part of a seed that develops into a new plant, cultivars generally reach a height of around 1 m (3.3 ft), and including the stem, leaves and roots. take 80–120 days from sowing to harvesting. Exports: products or items that the U.S. sells and sends to other countries. Exports include raw products like whole soybeans or processed products like soybean oil or Leaflets soybean meal. Fertilizer: any substance used to fertilize the soil, especially a commercial or chemical manure. Hilum: the scar on a seed marking the point of attachment to its seed vessel (the brown spot). Leaflets: sub-part of leaf blade. All but the first node of soybean plants produce leaves with three leaflets. Legume: plants that perform nitrogen fixation and whose fruit is a seed pod. Beans, peas, clover and alfalfa are all legumes. Nitrogen Fixation: the conversion of atmospheric nitrogen Leaf into a nitrogen compound by certain bacteria, such as Stem rhizobium in the root nodules of legumes. -

Promoting Sustainable Food Systems in Mediterranean Countries
Promoting sustainable food systems in Mediterranean countries: a framework to implement recommendations and actions Marie Josephe Amiot-Carlin, Marlène Perignon, Nicole Darmon, Sophie Drogue, Carole Sinfort, Eric Verger, Jalila El Ati, . The Medina-Study Group To cite this version: Marie Josephe Amiot-Carlin, Marlène Perignon, Nicole Darmon, Sophie Drogue, Carole Sinfort, et al.. Promoting sustainable food systems in Mediterranean countries: a framework to implement recommen- dations and actions. Development of voluntary guidelines for the sustainability of the Mediterranean diet in the Mediterranean region, Food and Agriculture Organization (FAO). ITA.; International Cen- tre for Advanced Mediterranean Agronomic Studies (CIHEAM). INT., Mar 2017, Bari, Italy. 141 p. hal-01595254 HAL Id: hal-01595254 https://hal.archives-ouvertes.fr/hal-01595254 Submitted on 2 Jun 2020 HAL is a multi-disciplinary open access L’archive ouverte pluridisciplinaire HAL, est archive for the deposit and dissemination of sci- destinée au dépôt et à la diffusion de documents entific research documents, whether they are pub- scientifiques de niveau recherche, publiés ou non, lished or not. The documents may come from émanant des établissements d’enseignement et de teaching and research institutions in France or recherche français ou étrangers, des laboratoires abroad, or from public or private research centers. publics ou privés. Distributed under a Creative Commons Attribution - ShareAlike| 4.0 International License Technical Workshop Development of voluntary -

2015 Do Not Enter Social Security Numbers on This Form As It May Be Made Public
l efile GRAPHIC p rint - DO NOT PROCESS I As Filed Data - I DLN: 93491320033496 OMB No 1545-0052 Form 990-PF Return of Private Foundation or Section 4947 ( a)(1) Trust Treated as Private Foundation Department of the Treasury 2015 Do not enter social security numbers on this form as it may be made public. Internal Revenue Service ► ► Information about Form 990- PF and its instructions is at www. irs.gov /form99Opf . • • ' For calendar year 2015 , or tax year beginning 01-01 - 2015 , and ending 12-31-2015 Name of foundation A Employer identification number JANET DE CARLI CHARITABLE FOUNDATION 94-3288290 Number and street (or P 0 box number if mail is not delivered to street address) BTelephone number (see instructions) 11640 REGNART CANYON DR (408) 872-3156 City or town, state or province , country, and ZIP or foreign postal code C If exemption application is pending, check here ► CUPERTINO, CA 95014 P G Check all that apply [Initial return [Initial return former public charity of a D 1. Foreign organizations , check here ► F-Final return F-A mended return P F-Address change F-Name change 2. Foreign organizations meeting the 85% test, check here and attach computation ► E If private foundation status was terminated H Check type of organization [Section 501( c)(3) exempt private foundation under section 507(b)(1)(A), check here ► F Section 4947( a)(1) nonexempt charitable trust Other taxable private foundation IFair market value of all assets at end JAccounting method [Cash F-Accrual F If the foundation is in a 60-month termination of year (from Pa,t II, col (c), [Other( specify) under section 507(b)(1)(B), check here ► F Ime 248 , 060 (Part I, column (d) must be on cash basis Disbursements Analysis of Revenue and Expenses Revenue and (The total of amounts n columns (b), (c), and (d) may not Net investment Adjusted net for charitable expensese per necessarily equal the amounts n column (a) (see (b) ncome (c) ncome purposes (a) books Instructions) ) (d) (cash basis only) 1 Contributions, gifts, grants, etc , received (attach schedule) . -

UTFPR • Sisu 2018 2 • RESULTADO DA 2A CHAMADA
UTFPR • SiSU 2018_2 • RESULTADO DA 2a CHAMADA Os candidatos na situação MATRICULADO ETAPA 1 devem confirmar a matrícula nos dias 02 e 03 de agosto de 2018, conforme item 9.2 do Edital 18/2018. Os candidatos na situação AGUARDANDO VAGA devem acompanhar a convocação da 3a Chamada (Chamada Nominal), dia 08/agosto/2018. CÂMPUS MEDIANEIRA Classificação Curso Categoria Nome do Candidato Situação (na cota) ALIMENTOS Cat. 3S PAMELA DA SILVA SOARES 2 MATRICULADO ETAPA 1 ALIMENTOS Cat. 3S GLADIS ADRIANA DE MORAIS 3 MATRICULADO ETAPA 1 ALIMENTOS Cat. 3S ISRAEL AZAF GONCALVES 4 MATRICULADO ETAPA 1 ALIMENTOS Cat. 3S CAROLAINE CRISTINA DE SANTANA 5 MATRICULADO ETAPA 1 ALIMENTOS Não cotista MARIVANI TERESINHA FRIZZO 2 MATRICULADO ETAPA 1 ALIMENTOS Não cotista CARLA ELOISA CANOVA 3 MATRICULADO ETAPA 1 ALIMENTOS Não cotista MARCOS ANTONIO FABRIN 4 MATRICULADO ETAPA 1 ALIMENTOS Não cotista LUANA SUZIN 5 MATRICULADO ETAPA 1 ALIMENTOS Não cotista TAIANARA SOARES SOUZA SANTOS 6 MATRICULADO ETAPA 1 ALIMENTOS Não cotista ARGEL AMARAL ROGLIN 8 MATRICULADO ETAPA 1 ALIMENTOS Não cotista LUCAS DE LIMA FACHIN 10 MATRICULADO ETAPA 1 ALIMENTOS Não cotista JEFERSON JUNIOR CAMARGO FERREIRA 11 MATRICULADO ETAPA 1 ALIMENTOS Não cotista ERICA LAIANA VASCONCELOS DE CARLI 12 MATRICULADO ETAPA 1 ALIMENTOS Não cotista KETLEN RAUANE CORDEIRO 13 MATRICULADO ETAPA 1 ALIMENTOS Não cotista CRISTIANE APARECIDA GONCALVES DA SILVA 14 MATRICULADO ETAPA 1 ALIMENTOS Não cotista PAULO LEMES CORDEIRO 15 MATRICULADO ETAPA 1 CIÊNCIA DA COMPUTAÇÃO Cat. 1S LUCAS BEDIN MARCHI 1 MATRICULADO ETAPA 1 CIÊNCIA DA COMPUTAÇÃO Cat. 3S EMANUELLY CARNIEL PERES 1 MATRICULADO ETAPA 1 CIÊNCIA DA COMPUTAÇÃO Cat. -

Fresh Fruit Cereal GF, DF, VG Serves: 1
Fresh Fruit Cereal GF, DF, VG Serves: 1 Ingredients Directions • 1 apple 1. Dice up the apple and banana and place into a bowl. • ½ banana 2. Option to chop up the nuts of your • 1 cup unsweetened choice and add them to the bowl almond milk along with the seeds and coconut. • 1 tablespoon pumpkin 3. Sprinkle the cinnamon or cocoa seeds powder over everything to taste. • 12 walnuts (or preferred 4. Pour in the milk and enjoy. nut of choice) • ¼ cup unsweetened shredded coconut • 1 tsp cinnamon or cocoa powder Food Restriction Codes GF – Gluten Free DF – Dairy Free VG – Vegetarian NF – Nut Free Healthy Blueberry Smoothie GF, VG Serves: 1 Ingredients Directions • 1 cup unsweetened 1. Add almond milk and ice into the almond milk blender, followed by avocado, protein powder, and blueberries. • 1 cup ice 2. Blend. • ¼ avocado, cubed • 1 scoop vanilla protein powder • ½ cup blueberries Food Restriction Codes GF – Gluten Free DF – Dairy Free VG – Vegetarian NF – Nut Free Golden Overnight Oats GF, VG, NF Serves: 1 Ingredients Directions • ⅓ cup rolled oats (if you 1. In a bowl, whisk turmeric, cinnamon, do not eat gluten, make cloves honey sure the oats are labeled as gluten-free) 2. Place oats in an air tight container (we like to reuse glass jars from nut • ⅔ cup milk butters and pasta sauces). • ¼ tsp turmeric 3. Pour the milk mixture over the oats and briefly stir. • ⅛ tsp cinnamon 4. Refrigerate with lid on tight for a • 1 pinch cloves minimum of 8 hours. And it can last • ⅛ tsp vanilla up to 5 days. -

Architecture Canada
Journal of the Society for the Study of Journal de la Société pour l’étude de l’ ARCHITECTUREARCHITECTURE inin // auau CANADACANADA CONTENTS / TABLE DES MATIÈRES Luc Noppen 2 Présentation / Presentation ANALYSES / ANALYSES Rhodri Windsor-Liscombe 3 Grounding the New Perspectives of Modernism: Canadian Airports and the Reconfiguration of the Cultural and Political Territory Marie-Josée Therrien 15 Diplomatic Malaise. The Challenge of Representing Canada Abroad Olga Zorzi Pugliese 25 The Mosaic Workers of the Angelo Principe Thomas Foster Memorial ESSAIS / ESSAYS André Casault 31 House Hunting Or I’Ve Never “Lived” In My House Yves Deschamps 43 L’art nécessaire. Quelques réflexions sur le Nigog et l’architecture RAPPORT / REPORT Jean Bélisle 49 Le moulin Légaré, Saint-Eustache (Québec) COMPTE RENDU / REVIEW Isabelle Caron 63 Martin Dubois Architecture contemporaine à Québec : 112 repères urbains Volume / Tome 28, numéros / numbers 1, 2 (2003) PRÉSENTATION PRESENTATION e numéro d’Architecture Canada présente une sélection de his issue of Architecture Canada presents a selection of articles textes soumis à la rédaction par des membres bien connus submitted to the Editorial Committee by some of SEAC’s Cde la SÉAC, mais aussi par de nouvelles figures qui proviennent Tregular members, but also by some new figures coming from d’horizons variés et qui se joignent à la Société, intéressés par la various spheres who adhere to the Society, interested by the jour- revue dans son nouveau format. nal’s new format. Cette fois, dans la section analyses, Rhodri Windsor-Liscom- This time, in the analyses section, Rhodri Windsor-Liscombe be examine le rôle qu’a joué l’architecture des aéroports cana- examines the role played by postwar Canadian airports’ archi- diens de l’après-guerre dans la construction d’une identité tecture in the development of a modern Canadian identity.