Feeding Infants and Young Children in Kitui County, Kenya
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
A Water Infrastructure Audit of Kitui County
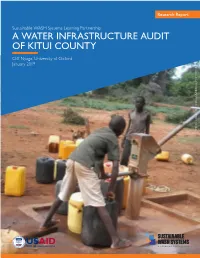
Research Report Research Report Sustainable WASH Systems Learning Partnership A WATER INFRASTRUCTURE AUDIT OF KITUI COUNTY Cliff Nyaga, University of Oxford January 2019 PHOTO CREDIT:PHOTO CLIFF NYAGA/UNIVERSITY OF OXFORD Prepared by: Cliff Nyaga, University of Oxford Reviewed by: Mike Thomas, Rural Focus; Eduardo Perez, Global Communities; Karl Linden, University of Colorado Boulder (UCB); and Pranav Chintalapati, UCB. Acknowledgements: The Kitui County Government would like to acknowledge the financial support received from the United States Agency for International Development (USAID). Further, the Kitui County Government appreciates its longstanding partnership with the University of Oxford and UNICEF Kenya through various collaborating programs, including the DFID-funded REACH Program. The leadership received from Emmanuel Kisangau, Kennedy Mutati, Philip Nzula, Augustus Ndingo, and Hope Sila — all from the County Ministry for Water Agriculture and Livestock Development — throughout the audit exercise is appreciated. The sub-county water officers were instrumental in logistics planning and in providing liaison between the field audit teams, communities, and County Ministries for Agriculture, Water, and Livestock Development and Administration and Coordination. A team of local enumerators led field data collection: Lucy Mweti, Grace Muisyo, Abigael Kyenze, Patrick Mulwa, Lydia Mwikali, Muimi Kivoko, Philip Muthengi, Mary Sammy, Ruth Mwende, Peter Musili, Annah Kavata, James Kimanzi, Purity Maingi, Felix Muthui, and Assumpta Mwikali. The technical advice and guidance received from Professor Rob Hope of the University of Oxford and Dr. Andrew Trevett of UNICEF Kenya throughout the planning, data collection, analysis, and preparation of this report is very much appreciated. Front cover: This Katanu Hand pump was developed in the late 1990s by the Government of Kenya and is the main water source for Nzamba Village in Ikutha Ward, Kitui. -

County Urban Governance Tools
County Urban Governance Tools This map shows various governance and management approaches counties are using in urban areas Mandera P Turkana Marsabit P West Pokot Wajir ish Elgeyo Samburu Marakwet Busia Trans Nzoia P P Isiolo P tax Bungoma LUFs P Busia Kakamega Baringo Kakamega Uasin P Gishu LUFs Nandi Laikipia Siaya tax P P P Vihiga Meru P Kisumu ga P Nakuru P LUFs LUFs Nyandarua Tharaka Garissa Kericho LUFs Nithi LUFs Nyeri Kirinyaga LUFs Homa Bay Nyamira P Kisii P Muranga Bomet Embu Migori LUFs P Kiambu Nairobi P Narok LUFs P LUFs Kitui Machakos Kisii Tana River Nyamira Makueni Lamu Nairobi P LUFs tax P Kajiado KEY County Budget and Economic Forums (CBEFs) They are meant to serve as the primary institution for ensuring public participation in public finances in order to im- Mom- prove accountability and public participation at the county level. basa Baringo County, Bomet County, Bungoma County, Busia County,Embu County, Elgeyo/ Marakwet County, Homabay County, Kajiado County, Kakamega County, Kericho Count, Kiambu County, Kilifi County, Kirin- yaga County, Kisii County, Kisumu County, Kitui County, Kwale County, Laikipia County, Machakos Coun- LUFs ty, Makueni County, Meru County, Mombasa County, Murang’a County, Nairobi County, Nakuru County, Kilifi Nandi County, Nyandarua County, Nyeri County, Samburu County, Siaya County, TaitaTaveta County, Taita Taveta TharakaNithi County, Trans Nzoia County, Uasin Gishu County Youth Empowerment Programs in urban areas In collaboration with the national government, county governments unveiled -

Towards Sustainable Charcoal Production and Trade in Kitui County Phosiso Sola1, Mieke Bourne1, Mary Njenga1, Anthony Kitema2, Siko Ignatius1 and Grace Koech1
CIFOR infobriefs provide concise, accurate, peer- reviewed information on current topics in forest research No. 297, September 2020 DOI: 10.17528/cifor/007721 | cifor.org Towards sustainable charcoal production and trade in Kitui County Phosiso Sola1, Mieke Bourne1, Mary Njenga1, Anthony Kitema2, Siko Ignatius1 and Grace Koech1 Key messages • Woodfuel, particularly charcoal, is an important livelihood source in Kitui County, with consumption largely in urban areas within and beyond the county, where it is still a critical energy source. • While charcoal movement out of the county has been banned since 2018, trade has continued in some form because of inadequate support, guidance and regulation. • While briquette production has been promoted, it has not seen substantial demand. • Because charcoal production has continued, a sustainable charcoal value chain in Kitui County has to be explored, including i) management of woodlands and sustainable harvesting of trees, e.g. through natural regeneration and enrichment planting of trees on degraded private and public lands; ii) promotion of efficient processing and carbonization; and iii) efficient and clean cooking. • Current institutional arrangements for guiding, supporting and controlling the value chain activities and actors can be improved to enhance the sustainability, enforcement, compliance, capacity and competitiveness of local value chains. • World Agroforestry (ICRAF), Adventist Development Relief Agency (ADRA) and partners undertook a number of activities in Kitui County and more widely in Kenya as a whole to generate evidence, knowledge and policy options, and to facilitate engagement for more sustainable woodfuel value chains under the project entitled Governing Multifunctional Landscapes (GML) in sub-Saharan Africa launched in 2018. -

Influence of Institutional Factors on Pupils
INFLUENCE OF INSTITUTIONAL FACTORS ON PUPILS’ PERFORMANCE IN KENYA CERTIFICATE OF PRIMARY EDUCATION IN PUBLIC PRIMARY SCHOOLS IN KANGUNDO DIVISION, MACHAKOS COUNTY, KENYA Timothy Musyoka Nthumo A Research Project Submitted in Partial Fulfillment of the Requirements for the Award of the Degree of Master of Education in Educational Administration University of Nairobi 2015 DECLARATION This research project is my original work and has not been presented for a degree in any other university. __________________________ Timothy Musyoka Nthumo E55/83715/2012 This research project has been submitted with our approval as university supervisors. _________________________ Dr. Mari Nelson Lecturer Department of Educational Administration and Planning University of Nairobi __________________________ Dr. Rose Obae Lecturer Department of Educational Administration and Planning University of Nairobi ii DEDICATION I dedicate this work to my wife Tabitha Musyoka, my children Dickson Kioko, Elizabeth Syokau, Solomon Ngete, my sister in-law Ruth Munyiva and my parents Samuel Nthumo and Naom Nthumo, for their patience , support and inspiration. iii ACKNOWLEDGEMENTS The successful completion of this study has been due to cooperation, assistance and encouragement of many people. Sincere appreciation to my concerned supervisors Dr. Mari Nelson and Dr. Rose Obae both lecturers in the Department of Educational Administration and Planning at the University of Nairobi for their insight, scholarly criticisms, friendly guidance and direction throughout the entire period of study, my deep gratitude also goes to the library staff for their invaluable assistance. My gratitude would be incomplete without expressing my heartily thanks to my wife Tabitha Mutindi who gave all the love, moral support and encouragement throughout the study. -
Dated 30Th April 2021
COUNTY GOVERNMENT OF KITUI THE COUNTY TREASURY FY: 2021/2022 BUDGET NOTES DATED 30TH APRIL 2021 County Mission and Vision County Vision To be a prosperous county with vibrant rural and urban economies whose people enjoy a high quality of life. County Mission To provide effective county services and an enabling environment for inclusive and sustainable socio-economic development and improved livelihoods for all. 2 KITUI COUNTY BUDGET NOTES FY 2021/22 Ministry Programme Project Name Project Intended Activities Cost Location/ Ward Vote 3711: General Other Infrastructure County Construction and Civil 801,538,964 Office of Administratio and Civil Works- wide works the n and Support CLIDP (72% Governor Services Infrastructure) Other Infrastructure County Construction and Civil 212,500,000 and Civil Works- wide works CLIDP (25% Infrastructure) Other Infrastructure County Construction and Civil 25,500,000 and Civil Works- Headquart works CLIDP (3% ers Administration) Purchase of Motor Countywi Purchase of Motor 20,000,000 Vehicles de Vehicles Construction of County Governor's and Deputy 40,000,000 Buildings Headquart Governor's residence ers Construction of County Partitioning/Completio 7,000,000 Buildings Headquart n of the Governor's ers Administration Block National Scholarships and other Countywi Provision of education 45,000,000 Social Safety Educational Benefits de bursaries to needy Net (Pro-poor students in secondary Program) and and universities as well Monitoring as infrastructural and Research support to educational Services facilities. -

Governance of Woodfuel Value Chains in Kenya an Analysis of Policies, Legislative Frameworks and Institutional Mechanisms
OCCASIONAL PAPER Governance of woodfuel value chains in Kenya An analysis of policies, legislative frameworks and institutional mechanisms Phosiso Sola Mieke Bourne Irene Okeyo Ignatius Siko Mary Njenga Occasional Paper 214 Governance of woodfuel value chains in Kenya An analysis of policies, legislative frameworks and institutional mechanisms Phosiso Sola World Agroforestry (ICRAF) Mieke Bourne World Agroforestry (ICRAF) Irene Okeyo University of Queensland Ignatius Siko World Agroforestry (ICRAF) Mary Njenga World Agroforestry (ICRAF) Center for International Forestry Research (CIFOR) Occasional Paper 214 © 2020 Center for International Forestry Research (CIFOR) Content in this publication is licensed under a Creative Commons Attribution 4.0 International (CC BY 4.0), http://creativecommons.org/licenses/by/4.0/ ISBN: 978-602-387-148-3 DOI: 10.17528/cifor/007890 Sola P, Bourne M, Okeyo I, Siko I and Njenga M. 2020. Governance of woodfuel value chains in Kenya: An analysis of policies, legislative frameworks and institutional mechanisms. Occasional Paper 214. Bogor, Indonesia: CIFOR. Photo by Anthony Kitema/ADRA Charcoal sacks in Kitui East. CIFOR Jl. CIFOR, Situ Gede Bogor Barat 16115 Indonesia T +62 (251) 8622-622 F +62 (251) 8622-100 E [email protected] cifor.org We would like to thank all funding partners who supported this research through their contributions to the CGIAR Fund. For a full list of the ‘CGIAR Fund’ funding partners please see: http://www.cgiar.org/our-funders/ Any views expressed in this publication are those of the authors. They do not necessarily represent the views of CIFOR, the editors, the authors’ institutions, the financial sponsors or the reviewers. -

Kitui County
A: Population Projections by Special Groups by- Sub-County and by Sex, 2017 Number Children Household Leadership by Subcounty and Sex KITUI COUNTY GENDER DATA SHEET County, Sub - 3 - 5 years 6 -17 years 200 186 county/Age group 177 Total Male Female Total Male Female 171 180 163 154 INTRODUCTION 160 148 Total County 113,972 58,051 55,922 405,482 206,091 199,391 142 139 141 Kitui County covers an area of 30,515 Km2. It borders Machakos and Makueni counties 140 128 128 Mwingi North 17,880 8,949 8,930 56,681 28,533 28,146 118 120 121 to the west, Tana River County to the east, TaitaTaveta to the south, Embu and 120 106 COUNCIL OF GOVERNORS Mwingi West 11,290 5,798 5,493 43,976 22,414 21,562 TharakaNithi counties to the north. It is located between latitudes 0°10 South and 3°0 100 87 South and longitudes 37°50 East and 39°0 East. Mwingi Central 16,754 8,565 8,189 55,171 28,150 27,022 Number 80 Kitui West 10,245 5,173 5,071 42,139 21,378 20,761 60 A: POPULATION/HOUSEHOLDS 40 Kitui Rural 11,049 5,688 5,361 42,983 21,935 21,049 20 - COUNTY GOVERNMENT OF KITUI Kitui Central 12,449 6,381 6,068 48,897 24,623 24,271 A1: Population Projections by sex, 2014-2020 Mwingi Mwingi Mwingi Kitui Kitui Kitui Kitui Kitui Kitui East 14,573 7,280 7,292 48,019 24,555 23,466 Number North West Central West Rural Central East South 2014 2015 2016 2017 2018 2020 Kitui South 19,733 10,216 9,517 67,615 34,503 33,113 COUNTY GENDER DATA SHEET Boys Girls Total 1,075,866 1,086,599 1,097,687 1,108,981 1,120,394 1,141,592 Source: Kenya Population and Housing Census 2009 -

5.8 Result of Test Drilling at 3 Target Communities
5.8 Result of Test Drilling at 3 Target Communities Depth Depth (GL-m) (GL-m) Well structure Geological log Discription Well structure Geological log Discription Well structure Geological log Discription 0 Top red soil 11" Top clay soil Top red soil 0 11" 2 2.8 2 1.2 11" 2 3.6 Highly weathered gneiss 11" 6 11" Highly weathered gneiss Permanent 6" Slightly weathered gneiss 11" Permanent 8 Weathered gneiss Casing 8 10 Permanen 6" Biotite gneiss Casing 6" 10 Weathered gneiss 10 t Casing 6"uPCV 14 Slightly weatered gneiss Bentonite Partly weathered gneiss 14 16 Casing Biotite gneiss Seal 18 Slightly weathered gneiss 20 6"uPCV 18 Weathered gneiss 19.0 20 Massive Bentonite Casing 22 Seal 22 Partly weathered biotite gneiss Bentonite 6"uPCV 25.0 Weathered gneiss biotite gneiss 27.0 Seal Casing 28 28 30 30 30.0 Highly weathered gneiss 30 31.0 31.0 32 6"uPCV Weathered trachyte 33.0 Gravel 34.0 6"uPCV Screen 36 Packing Partly fractured Screen Weathered & fractured 40 Gravel 40.0 φ2-9mm biotite gneiss gneiss 40 Packing 43.0 Gravel Packing 44 φ2-9mm 46.0 6"uPCV Bbiotite gneiss Screen 48 φ2-9mm 48.0 48 50 49.0 Massive 50 52.0 52 biotite gneiss 51.0 54.0 55.0 Partly weathered Partly fractured biotite gneiss A5-8-1 58.0 60 61.0 biotite gneiss 61.0 60 60.0 Slightly weathered gneiss 60 64.0 Massive 67.0 biotite gneiss 66.0 70 70.0 70 73.0 73.0 72 Partly fractured 72.0 72 76.0 76 biotite gneiss 75.0 78.0 80 80 79.0 80 82.0 Biotite gneiss Weathered gneiss 85.0 84 85.0 84.0 Massive 90 91.0 91.0 biotite gneiss 90.0 90 90 94.0 Fractured biotite gneiss 94.0 100 100.0 100.0 100 103.0 103 103.0 103 110 110 5.9 Result of Wind Velocity Survey Possible Term to Start Pump up and Possible Time to Work about Windmill Pump Possible Term to Start Possible Time to Work(Hour) District Site No. -

Explaining Resource Use, Management and Productivity Among the Akamba, Orma and Somali in the Former Eastern Statelands of Kenya
©Kamla-Raj 2004 Stud. Tribes Tribals, 2(1): 55-63 (2004) Common Range, Different Tribes: Explaining Resource Use, Management and Productivity among the Akamba, Orma and Somali in the former Eastern Statelands of Kenya Dickson Mong’are Nyariki1 and Jan Van den Abeele2 1. Department of Range Management, University of Nairobi P.O. Box 29053, Nairobi, Kenya Email: [email protected] 2. Forestry Development Support Programme, Belgian Technical Cooperation, P.O. Box 30513, Nairobi, Kenya KEYWORDS Common use; range management; resource conflicts; Eastern Statelands; Kenya ABSTRACT This paper describes the major livelihood activities of three ethnic communities who use in common the former Kenyan Eastern Statelands. It also looks at how the livelihoods and the range could be improved while maintaining the common access to resources, so as to avoid potential conflicts. It is suggested that for improvement of range management the unsettled lands should be accessed by all the communities under ranching societies without having to exclude non-members. A number of approaches should be instituted, including bush control and reseeding. Bush control can be achieved through exploitation of trees of low timber value for charcoal production to earn income for households. To increase livestock productivity, it is proposed that proper livestock and grazing management be practised, including the introduction of superior breeds, improved livestock facilities, adequate animal healthcare and rotational grazing through paddocking. INTRODUCTION and improve the living standards of the communities, the stakeholders and development The colonial government in Kenya set aside agents should rethink the use and management the former Eastern Statelands for State of this resource. -

Registered Voters Per Caw for 2017 General Elections
REGISTERED VOTERS PER CAW FOR 2017 GENERAL ELECTIONS NO. OF COUNTY CONST_ CAW_ COUNTY_NAME CONSTITUENCY_NAME CAW_NAME VOTERS POLLING _CODE CODE CODE STATIONS 001 MOMBASA 001 CHANGAMWE 0001 PORT REITZ 17,082 26 001 MOMBASA 001 CHANGAMWE 0002 KIPEVU 13,608 22 001 MOMBASA 001 CHANGAMWE 0003 AIRPORT 16,606 26 001 MOMBASA 001 CHANGAMWE 0004 CHANGAMWE 17,586 29 001 MOMBASA 001 CHANGAMWE 0005 CHAANI 21,449 33 001 MOMBASA 002 JOMVU 0006 JOMVU KUU 22,269 36 001 MOMBASA 002 JOMVU 0007 MIRITINI 16,899 27 001 MOMBASA 002 JOMVU 0008 MIKINDANI 30,139 46 001 MOMBASA 003 KISAUNI 0009 MJAMBERE 22,384 34 001 MOMBASA 003 KISAUNI 0010 JUNDA 23,979 37 001 MOMBASA 003 KISAUNI 0011 BAMBURI 17,685 28 001 MOMBASA 003 KISAUNI 0012 MWAKIRUNGE 4,946 9 001 MOMBASA 003 KISAUNI 0013 MTOPANGA 17,539 28 001 MOMBASA 003 KISAUNI 0014 MAGOGONI 14,846 23 001 MOMBASA 003 KISAUNI 0015 SHANZU 24,772 39 001 MOMBASA 004 NYALI 0016 FRERE TOWN 20,215 33 001 MOMBASA 004 NYALI 0017 ZIWA LA NG'OMBE 20,747 31 001 MOMBASA 004 NYALI 0018 MKOMANI 19,669 31 001 MOMBASA 004 NYALI 0019 KONGOWEA 24,457 38 001 MOMBASA 004 NYALI 0020 KADZANDANI 18,929 32 001 MOMBASA 005 LIKONI 0021 MTONGWE 13,149 23 001 MOMBASA 005 LIKONI 0022 SHIKA ADABU 13,089 21 001 MOMBASA 005 LIKONI 0023 BOFU 18,060 28 001 MOMBASA 005 LIKONI 0024 LIKONI 10,855 17 001 MOMBASA 005 LIKONI 0025 TIMBWANI 32,173 51 001 MOMBASA 006 MVITA 0026 MJI WA KALE/MAKADARA 19,927 34 001 MOMBASA 006 MVITA 0027 TUDOR 20,380 35 001 MOMBASA 006 MVITA 0028 TONONOKA 21,055 36 001 MOMBASA 006 MVITA 0029 SHIMANZI/GANJONI 17,312 33 001 MOMBASA -

Kitui County Climate Information Services Strategic Plan January 2015
Kitui County Climate Information Services Strategic Plan January 2015 Kenya Meteorological Department REPUBLIC OF KENYA THE MINISTRY OF ENVIRONMENT, WATER AND NATURAL RESOURCES STATE DEPARTMENT OF ENVIRONMENT, AND NATURAL RESOURCES KENYA METEOROLOGICAL SERVICE Kitui County Climate Information Services Strategic Plan A Vision 2030 implementing Agency December 2015 Page 2 of 37 Index Forward by KMS Director Forward by Kitui County Government Executive summary 1.0 Background and Context 1.1 Background 1.2 Context 1.3 Climate in Kitui County 2.0 Proposed framework for developing the Kitui County Climate Information Services Plan (KCCISP) 2.1 Aims 2.2 Principles 2.3 Roles and Responsibilities of County Directors of Meteorological Services 2.4 Linkages with related CIS initiatives 2.5 Situational Analysis of the County’s observational network 2.6 Proposed strengthening of the County’s observational network 2.7 Process of providing CIS 2.8 CIS intermediaries 2.9 Awareness raising and promoting uptake of CIS 2.10 Monitoring and evaluation 2.11 Planning and budgeting Annexes Annex 1 CIS intermediary key contacts Annex 2 Proposed CIS intermediaries and Training Annex 3 Timetable of activities for Ada CIS and CAF activities in Kitui Annex 4 Summary baseline of current use of CIS in Kitui County Annex 5 Summary KMS Forecasts Skill Scores Annex 6 References Figures Figure 1: Population in Kitui County by Principal Livelihood groups Figure 2: Average rainfall distribution in Kitui over March April May and October November December rainy seasons Figure -

County Name County Code Location
COUNTY NAME COUNTY CODE LOCATION MOMBASA COUNTY 001 BANDARI COLLEGE KWALE COUNTY 002 KENYA SCHOOL OF GOVERNMENT MATUGA KILIFI COUNTY 003 PWANI UNIVERSITY TANA RIVER COUNTY 004 MAU MAU MEMORIAL HIGH SCHOOL LAMU COUNTY 005 LAMU FORT HALL TAITA TAVETA 006 TAITA ACADEMY GARISSA COUNTY 007 KENYA NATIONAL LIBRARY WAJIR COUNTY 008 RED CROSS HALL MANDERA COUNTY 009 MANDERA ARIDLANDS MARSABIT COUNTY 010 ST. STEPHENS TRAINING CENTRE ISIOLO COUNTY 011 CATHOLIC MISSION HALL, ISIOLO MERU COUNTY 012 MERU SCHOOL THARAKA-NITHI 013 CHIAKARIGA GIRLS HIGH SCHOOL EMBU COUNTY 014 KANGARU GIRLS HIGH SCHOOL KITUI COUNTY 015 MULTIPURPOSE HALL KITUI MACHAKOS COUNTY 016 MACHAKOS TEACHERS TRAINING COLLEGE MAKUENI COUNTY 017 WOTE TECHNICAL TRAINING INSTITUTE NYANDARUA COUNTY 018 ACK CHURCH HALL, OL KALAU TOWN NYERI COUNTY 019 NYERI PRIMARY SCHOOL KIRINYAGA COUNTY 020 ST.MICHAEL GIRLS BOARDING MURANGA COUNTY 021 MURANG'A UNIVERSITY COLLEGE KIAMBU COUNTY 022 KIAMBU INSTITUTE OF SCIENCE & TECHNOLOGY TURKANA COUNTY 023 LODWAR YOUTH POLYTECHNIC WEST POKOT COUNTY 024 MTELO HALL KAPENGURIA SAMBURU COUNTY 025 ALLAMANO HALL PASTORAL CENTRE, MARALAL TRANSZOIA COUNTY 026 KITALE MUSEUM UASIN GISHU 027 ELDORET POLYTECHNIC ELGEYO MARAKWET 028 IEBC CONSTITUENCY OFFICE - ITEN NANDI COUNTY 029 KAPSABET BOYS HIGH SCHOOL BARINGO COUNTY 030 KENYA SCHOOL OF GOVERNMENT, KABARNET LAIKIPIA COUNTY 031 NANYUKI HIGH SCHOOL NAKURU COUNTY 032 NAKURU HIGH SCHOOL NAROK COUNTY 033 MAASAI MARA UNIVERSITY KAJIADO COUNTY 034 MASAI TECHNICAL TRAINING INSTITUTE KERICHO COUNTY 035 KERICHO TEA SEC. SCHOOL